经皮置钉与后路开放手术治疗胸腰段脊柱骨折的Meta 分析
2016-11-24 02:18:34孙祥耀张希诺海涌
中国骨与关节杂志 2016年11期
孙祥耀 张希诺 海涌
. Mata 分析 Meta-analysis .
经皮置钉与后路开放手术治疗胸腰段脊柱骨折的Meta 分析
孙祥耀张希诺海涌
目的系统评价经皮椎弓根螺钉内固定术 ( percutaneous pedicle screw fixation ) 与后路开放椎弓根螺钉内固定术 ( posterior open pedicle screw fixation ) 治疗胸腰段脊柱骨折的疗效,为胸腰段骨折的治疗提供更好的科学依据。方法检索并收集经皮椎弓根螺钉内固定术与后路开放手术治疗胸腰段脊柱骨折的比较性研究。计算机检索下列数据库:Pubmed ( 1966 年至 2016 年 3 月 )、Cochrane 图书馆 ( 2016 年第 3 期 )、Embase ( 1966 年至 2016 年 3 月 )。人工检索期刊 ( 1990 年至 2016 年 3 月 ) The Journal of Bone and Joint Surgery、Spine、European Spine Journal。2 名脊柱外科专业评价员根据纳入与排除标准,独立筛选文献,使用 Cochrane 协作网提供的 RevMan5.3 进行 Meta 分析。结果最终纳入 5 项随机对照试验 ( randomized controlled trail,RCT ),共计 318 例,其中经皮椎弓根螺钉内固定术 158 例,后路开放椎弓根螺钉内固定术 160 例。Meta 分析后结果显示,经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组相比,手术时间短 [ WMD=-0.67,95% CI ( -1.20,-0.14 ),P=0.01 ],出血量少 [ WMD=-2.83,95% CI ( -4.15,-1.51 ),P<0.0001 ],术后总体疼痛视觉模拟评分 ( visual analogue scale,VAS ) 小 [ WMD=-2.79,95% CI ( -3.80,-1.77 ),P<0.0001 ],术后 3 个月 VAS 评分小 [ WMD=-2.33,95% CI ( -3.08,-1.58 ),P<0.00001 ],住院时间短 [ WMD=-1.79,95% CI ( -2.48,-1.11 ),P<0.00001 ],而两者术后 1 周内 VAS 评分 [ WMD=-4.02,95% CI ( -8.98,0.94 ),P=0.11 ]、术后手术节段 Cobb’s 角 [ WMD=-0.72,95% CI ( -2.32,0.89),P=0.38 ]、术后手术节段 Cobb’s 角矫正度丢失 [ WMD=-0.05,95% CI ( -0.40,0.31 ),P=0.80 ]、手术并发症发生率 [ RR=0.57,95% CI ( 0.19,1.67 ),P=0.30 ]、椎弓根螺钉位置异常发生率 [ RR=0.69,95% CI ( 0.20,2.37 ),P=0.55 ]、术后感染发生率[ RR=0.34,95% CI ( 0.04,3.18 ),P=0.34 ] 相比,差异均无统计学意义。结论经皮椎弓根螺钉内固定术与后路开放椎弓根螺钉内固定术相比,手术时间短,出血量少,住院时间短,术后 3 个月时 VAS 评分较低,但是两者术后 1 周内 VAS 评分、术后 Cobb’s 角大小及术后矫正度丢失、手术并发症的发生率相比,差异均无统计学意义。
脊柱骨折;胸椎;腰椎;最小侵入性外科手术;Meta 分析
胸腰段脊柱骨折约占脊柱骨折总数的 75%,为脊柱最常见的骨折[1]。胸腰段骨折通常为高能量损伤,会引起疼痛、畸形以及功能丧失[2]。近来,经皮椎弓根螺钉内固定术已经应用到胸腰段脊柱骨折患者的治疗之中,意在降低手术区域软组织的损伤以及手术并发症的发生率[3-4]。目前,对于经皮椎弓根螺钉内固定术治疗胸腰段脊柱骨折与后路开放手术治疗的差异尚有争议,为此笔者搜集已发表的关于经皮椎弓根螺钉内固定术治疗胸腰段脊柱骨折与后路开放手术治疗比较的随机对照试验,对两种术式的手术时间、术中出血量、住院时间、术后疼痛,术后 Cobb’s 角变化以及相关并发症等进行分析,从而探讨两种治疗方法的差异。
资料与方法
一、文献检索
检索并收集经皮椎弓根螺钉内固定术与后路开放手术治疗胸腰段脊柱骨折的比较性研究。计算机检索下列数据库:Pubmed ( 1966 年至 2016 年 3 月 )、Cochrane 图书馆 ( 2016 年第 3 期 )、Embase ( 1966 年至 2016 年 3 月 )。人工检索期刊 ( 1990 年至 2016 年3 月 ) The Journal of Bone and Joint Surgery、Spine、European Spine Journal。检索关键词有 thoracolumbar fracture、lumbar fracture、percutaneous pedical screw fixation、open fixation、posterior surgery、sextant、traditional fixation、conventional fixation、minimally invasive surgery、comparative study、randomized controlled trail、clinical trail。
二、文献纳入与排除标准
1. 纳入标准:( 1 ) 国内外公开发表的比较经皮椎弓根螺钉内固定与后路开放手术治疗胸腰段脊柱骨折的随机对照研究;( 2 ) 术前辅助检查提示累及单个椎体的胸腰段脊柱骨折,前柱爆裂骨折,后柱完整或轻度韧带及骨性损伤,椎间盘未见明显损伤,轴位椎管内占位比<1 / 3,无神经功能障碍,无骨质疏松,伤后 2 周内的新鲜骨折;( 3 ) 平均随访时间>12 个月;( 4 ) 患者国籍、性别、年龄、种族不限。
2. 排除标准:( 1 ) 动物实验;( 2 ) 伴有神经损伤、其它合并损伤或疾病; ( 3 ) 平均随访时间<12 个月;( 4 ) 陈旧性胸腰段脊柱骨折;( 5 ) 非随机对照研究。
三、文献质量评价与资料提取
2 名脊柱外科专业评价员根据上述纳入与排除标准,独立筛选文献,如有异议,通过咨询第三方解决。采用 Furlan 质量评价标准对检索出的随机对照实验的方法学质量进行评估[5]。其中 Furlan 质量评价总分≥6 分 ( 总分 12 分 ) 为高质量方法学研究最终纳入到此研究中。如果出现分歧,通过第三人裁定解决。
四、结局指标
( 1 ) 手术时间 ( duration of surgery );( 2 ) 术中出血量 ( intraoperative blood loss );( 3 ) 术后 VAS 评分 ( postoperative visual analogue scale );( 4 ) 住院时间 ( hospital length of stay );( 5 ) 术后 Cobb’s 角( postoperative Cobb angle );( 6 ) 术后 Cobb’s 角矫正度丢失 ( postoperative Cobb angle correction loss );( 7 )手术并发症发生率 ( complication rate ),包括椎弓根螺钉位置异常 ( pedicle screw misplacement rate )、术后感染 ( postoperative infection rate )。
五、统计学处理
使用 Cochrane 协作网提供的 RevMan5.3 进行Meta 分析。采用 χ2检验对各研究间的异质性进行分析,当各研究间异质性检验差异无统计学意义 ( P>0.1,I2<50% ) 时,采用固定效应模型进行分析;如果各研究之间异质性检验差异有统计学意义 ( P<0.1,I2>50% ) 时,则采用随机效应模型进行分析。二分类变量采用 OR 值,采用 95% CI 表示。
结 果
一、文献检索结果及质量评价
根据上述检索策略,共检索到相关文献 1477篇。根据其题目和摘要进行筛选,排除非临床研究、非随机对照试验、重复发表等不合格文献,进一步阅读全文后排除低质量文献以及无法提取数据的文献,最终纳入 4 篇文章,共 5 项随机对照试验[6-9],共计 318 例,其中经皮椎弓根螺钉内固定术 ( percutaneous pedicle screw fixation ) 158 例,后路开放椎弓根螺钉内固定术 ( posterior open pedicle screw fixation ) 160 例;其中 Lyu 等[7]将其研究设计为将患者随机分为数量相等的经皮跨伤椎椎弓根螺钉内固定组( MIF4 )、经皮经伤椎椎弓根螺钉内固定组 ( MIF6 )以及后路开放经伤椎固定组进行比较,因此将其视为 2 篇随机对照研究进行分析,相当于总共纳入了5 项研究 ( 表1 )。
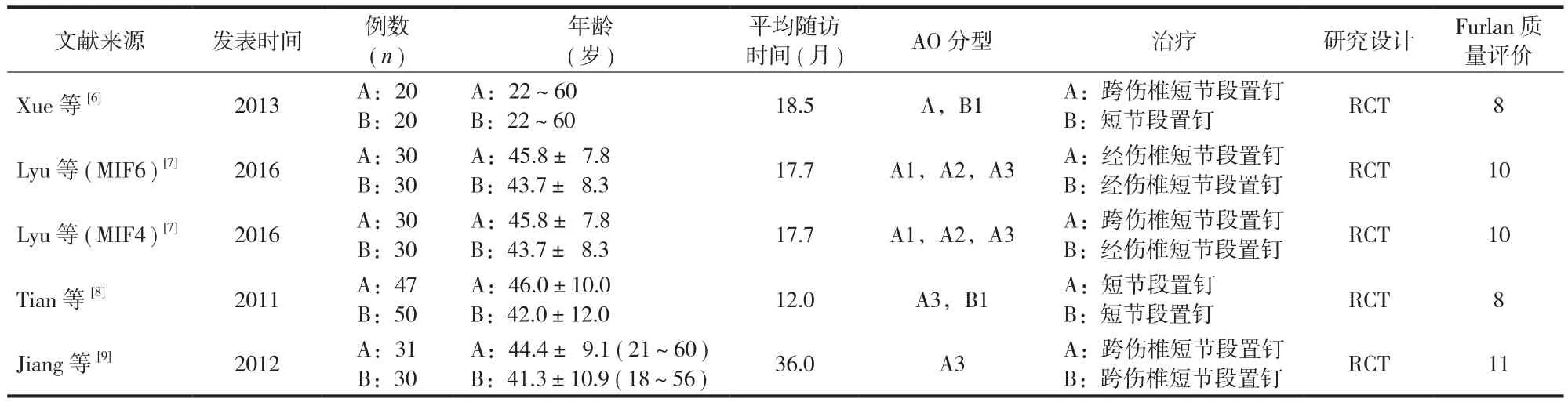
表1 纳入的比较经皮椎弓根螺钉内固定术与后路开放椎弓根螺钉内固定术的 5 项研究Tab.1 The 5 trials meeting the inclusion criteria in the comparison between percutaneous pedicle screw fixation and posterior open pedicle screw fixation for thoracolumbar fractures
二、Meta 分析结果
1. 手术时间:5 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的手术时间比较[6-9],共纳入 318 例,经皮椎弓根螺钉内固定组 158 例,后路开放椎弓根螺钉内固定组 160 例。各研究组间有统计学异质性 ( P=0.0004,I2=80% ),采用随机效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的手术时间少于后路开放椎弓根螺钉内固定组,差异有统计学意义 [ WMD=-0.67,95% CI ( -1.20,-0.14 ),P=0.01 ] ( 图 1 )。
2. 术中出血量:5 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的术中出血量比较[6-9],共纳入 318 例,经皮椎弓根螺钉内固定组 158 例,后路开放椎弓根螺钉内固定组160 例。各研究间有统计学异质性 ( P<0.00001,I2=95% ),采用随机效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的术中出血量少于后路开放椎弓根螺钉内固定组,差异有统计学意义 [ WMD=-2.83,95% CI ( -4.15,-1.51 ),P<0.0001 ] ( 图 2 )。
3. 术后 VAS 评分:5 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的术后 VAS 评分比较[6-9],共纳入 318 例,经皮椎弓根螺钉内固定组 158 例,后路开放椎弓根螺钉内固定组 160 例。总体各项研究间有统计学异质性 ( P<0.00001,I2=91% ),采用随机效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的术后 VAS 评分小于后路开放椎弓根螺钉内固定组,差异有统计学意义[ WMD=-2.79,95% CI ( -3.80,-1.77 ),P<0.0001 ] ( 图 3 )。亚组分析显示,术后 1 周内 VAS 评分亚组I2=97%,经皮椎弓根螺钉内固定组的术后 VAS 评分与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ WMD=-4.02,95% CI ( -8.98,0.94 ),P=0.11 ],术后 3 个月 VAS 评分亚组 I2=74%,经皮椎弓根螺钉内固定组的术后 VAS 评分小于后路开放椎弓根螺钉内固定组,差异有统计学意义 [ WMD=-2.33,95% CI ( -3.08,-1.58 ),P<0.00001 ]。

图 1 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组手术时间的比较Fig.1 Comparison of the duration of surgery between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group
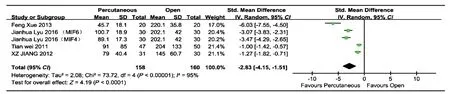
图 2 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组术中出血量的比较Fig.2 Comparison of the intraoperative blood loss between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group
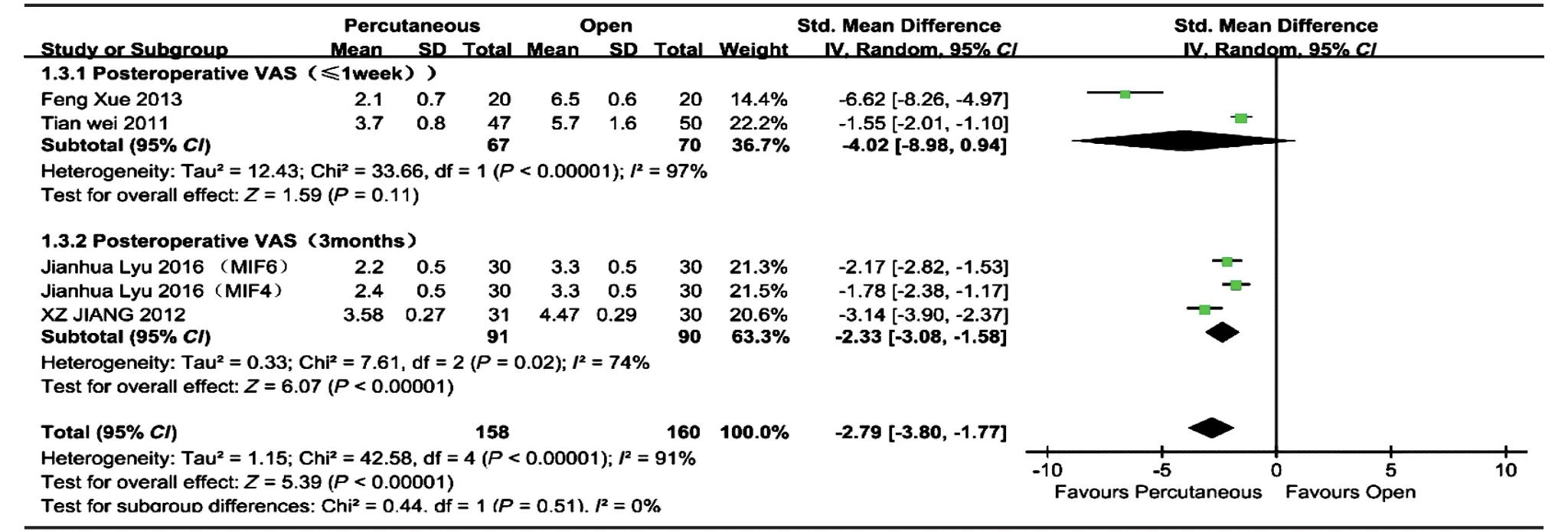
图 3 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组术后 VAS 评分的比较Fig.3 Comparison of the postoperative VAS score between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group
4. 住院时间:4 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根钉内固定组的住院时间比较[6-7,9],共纳入 221 例,经皮椎弓根螺钉内固定组 111 例,后路开放椎弓根螺钉内固定组 110 例。各项研究间有统计学异质性 ( P=0.004,I2=78% ),采用随机效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的住院时间少于后路开放椎弓根螺钉内固定组,差异有统计学意义 [ WMD=-1.79,95% CI ( -2.48,-1.11 ),P<0.00001 ] ( 图 4 )。
5. 术后手术节段 Cobb’s 角改变:2 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的术后手术节段 Cobb’s 角大小的比较[8-9],共纳入 158 例,经皮椎弓根螺钉内固定组 78 例,后路开放椎弓根螺钉内固定组 80 例。各研究间有统计学异质性 ( P<0.00001,I2=95% ),采用随机效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的住院时间与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ WMD=-0.72,95% CI ( -2.32,0.89 ),P=0.38 ]。4 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的术后手术节段Cobb’s 角大小的比较[7-9],共纳入 278 例,经皮椎弓根螺钉内固定组的术后手术节段 138 例,后路开放椎弓根螺钉内固定组 140 例。各研究间有统计学异质性 ( P=0.09,I2=53% ),采用随机效应模型进行Meta 分析。经皮椎弓根螺钉内固定组的术后手术节段 Cobb’s 角矫正度丢失与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ WMD=-0.05,95% CI ( -0.40,0.31 ),P=0.80 ] ( 图 5 )。
6. 手术并发症:4 项研究进行了经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组的手术并发症发生率的比较[8-9]。共纳入 316 例,经皮椎弓根螺钉内固定组 156 例,后路开放椎弓根螺钉内固定组160 例。总体各项研究间无统计学异质性 ( P=0.71, I2=0% ),采用固定效应模型进行 Meta 分析。经皮椎弓根螺钉内固定组的并发症发生率与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ RR=0.57,95% CI ( 0.19,1.67 ),P=0.30 ]。亚组分析显示,椎弓根螺钉位置异常亚组 I2=9%,经皮椎弓根螺钉内固定组的椎弓根螺钉位置异常发生率与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ RR=0.69,95% CI ( 0.20,2.37 ),P=0.55 ],术后感染亚组 I2=0%,经皮椎弓根螺钉内固定组的术后感染发生率与后路开放椎弓根螺钉内固定组比较,差异无统计学意义 [ RR=0.34,95% CI ( 0.04,3.18 ),P=0.34 ] ( 图 6 )。

图 4 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组住院时间的比较Fig.4 Comparison of the hospital length of stay between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group
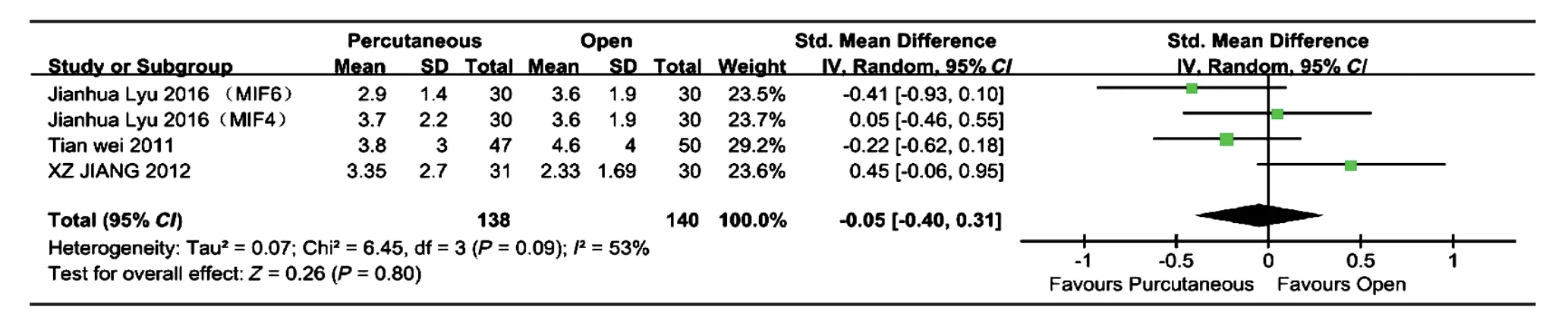
图 5 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组术后 Cobb’s 角矫正度丢失的比较Fig.5 Comparison of the postoperative Cobb’s angle correction loss between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group

图 6 经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组手术并发症发生率的比较Fig.6 Comparison of the complication rate between percutaneous pedicle screw fixation group and posterior open pedicle screw fixation group
讨 论
胸腰段脊柱骨折手术治疗的目的主要有两点:首先,为骨折损伤节段提供即刻稳定性;其次,保证骨折椎体的愈合或运动节段融合的发生[10]。手术的指征通常为后凸>30°,节段性后凸伴有后方骨性结构或韧带损伤,椎体塌陷超过 50%,累及三柱的骨折,椎管占位<40% 并且不伴神经系统严重损伤;手术治疗方式需要视具体情况而定,有相关研究表明,后路开放椎弓根螺钉内固定能获得很好的临床疗效和影像学改变[11-12]。然而,后路开放椎弓根螺钉内固定需要对椎旁肌以及筋膜等组织进行剥离,这将引起对脊柱中线结构的医源性损伤,并会导致脊柱不稳定以及慢性疼痛;并且其置钉引发的上位关节突关节的损伤发生率高达 24%,从而成为邻近节段退变的高危因素[13]。有研究指出,后路开放手术有感染可能,进行后路开放手术患者中约3.1% 出现了术后感染[14]。后路开放手术出血量较多,Verlaan 等[14]指出后路开放手术或前后路联合手术平均出血量会达到 1 L。考虑到后路开放手术治疗胸腰段脊柱骨折的不足,Assaker[15]首先将经皮椎弓根螺钉内固定技术应用于胸腰段脊柱骨折的治疗。相比之下,很多文献指出经皮椎弓根螺钉内固定术能有效降低手术出血量,缩短手术时间,降低对已经受损的软组织的损害[9,16-18]。然而,经皮椎弓根螺钉内固定术对手术技术要求较高,学习曲线较长,限制其广泛应用。
本次系统评价共纳入 5 项临床研究,共计 318例,其中经皮椎弓根螺钉内固定术 158 例,后路开放椎弓根螺钉内固定术 160 例。本研究结果提示,与后路开放椎弓根螺钉内固定术相比,经皮椎弓根螺钉内固定术手术时间短,出血量少,住院时间短,提示在上述方面,经皮椎弓根螺钉内固定有优势[19-20]。
恢复脊柱序列是手术治疗胸腰段脊柱骨折的目标之一。既往的研究结果显示,随访中接受经皮椎弓根螺钉内固定术治疗的患者会出现矫正度的丢失,这可能与微创手术中往往使用万向椎弓根螺钉有关。万向椎弓根螺钉的钉头和钉尾之间会产生微动,这可能对术后矫正度的丢失产生影响[21]。并且有文献指出,微创手术有复位困难和维持前凸能力较差的缺点[22]。然而,本研究中经皮椎弓根螺钉内固定术与开放后路椎弓根螺钉内固定术,在术后Cobb’s 角大小以及矫正度的丢失方面无明显差异,其原因可能为万向椎弓根螺钉对连接棒产生的弯曲力与剪切力的共同作用下,有效阻碍了连接棒与钉头之间的滑动[23];并且本研究纳入的临床研究均为单个椎体的骨折,骨折程度不重,复位相对容易,平均随访时间较短,也可能影响研究结果。
术后疼痛的降低能够使患者早期下床活动,缩短康复所需的时间,缩短住院时间并且降低住院费用[24]。本研究对相关 5 项研究的术后 VAS 评分进行了比较,并发现总体经皮椎弓根螺钉内固定组术后VAS 评分低于后路开放椎弓根螺钉内固定组,差异有统计学意义。然而,在术后 1 周内 VAS 评分亚组中,经皮椎弓根螺钉内固定组的术后 VAS 评分与后路开放椎弓根螺钉内固定组差异无统计学意义;经皮椎弓根螺钉内固定组的术后 VAS 评分小于后路开放椎弓根螺钉内固定组,差异有统计学意义。据此推测VAS 评分可能与随访的时间有关,后路开放椎弓根螺钉内固定手术操作会对操作区域内的肌肉组织以及神经组织等重要结构造成更大的伤害,这可能是造成慢性疼痛的原因,因此 1 周之内经皮组与后路开放组之间 VAS 评分无差异,随访 3 个月出现经皮椎弓根钉内固定组 VAS 评分比后路开放组低[25]。
术后感染及椎弓根螺钉位置异常是脊柱手术常见的并发症,其中术后感染以切口感染最为常见;通常将椎弓根螺钉位置不良定义为螺钉穿透椎弓、椎体前壁或上下终板[26]。本研究中经皮椎弓根螺钉内固定组与后路开放椎弓根螺钉内固定组在手术并发症发生率方面无统计学差异,并且在术后感染及椎弓根螺钉位置异常方面也无统计学差异。此研究结果表明,虽然有文献报道开放手术有较高的切口感染风险[27],但是在严格无菌操作及抗生素的使用条件下,感染的发生率在两者之间无统计学差异。本研究结果也表明,在微创手术操作中,影像设备的使用以及导航技术的应用能明显减小椎弓根螺钉位置异常的发生率,明显提高微创手术的安全性[8]。
本次系统评价目前存在以下局限性:( 1 ) 本研究纳入虽然都为随机对照试验 ( randomized controlled trail,RCT ),但是纳入文章数量较少,可能影响其可靠性;( 2 ) 纳入文章的研究例数较少,因此结果的可靠性需要进一步考量;( 3 ) 文章未纳入全部的术后疗效指标 ( 如术后椎体高度、ODI 评分等 ),导致数据分析不全面;( 4 ) 各研究随访时间的差异可能影响结果的可靠性;( 5 ) 各项研究之间的异质性较大,采用随机效应模型,可能影响结果的可靠性。
中等数据支持,经皮椎弓根螺钉内固定术与后路开放椎弓根螺钉内固定术相比,手术时间短,出血量少,住院时间短,术后 3 个月时 VAS 评分较低,但是两者术后 1 周内 VAS 评分无统计学差异,术后 Cobb’s 角矫正情况无统计学差异。低等数据支持,经椎弓根内固定术与后路开放椎弓根钉内固定术相比,手术并发症的发生率无统计学差异。
[1] Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine, 1996, 21(4):492-499.
[2] Diaz JJ Jr, Cullinane DC, Altman DT, et al. Practice management guidelines for the screening of thoracolumbar spine fracture. J Trauma, 2007, 63(3):709-718.
[3] Hsieh PC, Koski TR, Sciubba DM, et al. Maximizing the potential of minimally invasive spine surgery in complex spinal disorders. Neurosurg Focus, 2008, 25(2):E19.
[4] Smith JS, Ogden AT, Fessler RG. Minimally invasive posterior thoracic fusion. Neurosurg Focus, 2008, 25(2):E9.
[5] Furlan AD, Pennick V, Bombardier C, et al. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine, 2009, 34(18):1929-1941.
[6] Xue F, Fu ZG, Zhang DY, et al. Minimal invasive internal fixation with U-shaped break-off pedicle screws for treatent of thoracolumbar fractures. Beijing Da Xue Xue Bao, 2013, 45(5):728-731.
[7] Lyu J, Chen K, Tang Z, et al. A comparison of three different surgical procedures in the treatment of type A thoracolumbar fractures: a randomized controlled trial. Int Orthop, 2016, 40(6):1233-1238.
[8] Tian W, Han X, He D, et al. The comparison of computer assisted minimally invasive spine surgery and traditional open treatment for thoracolumbar fractures. Zhonghua Wai Ke Za Zhi, 2011, 49(12):1061-1066.
[9] Jiang XZ, Tian W, Liu B, et al. Comparison of a paraspinal approach with a percutaneous approach in the treatment of thoracolumbar burst fractures with posterior ligamentous complex injury: a prospective randomized controlled trial. J Int Med Res, 2012, 40(4):1343-1356.
[10] Vanek P, Bradac O, Konopkova R, et al. Treatment of thoracolumbar trauma by short-segment percutaneous transpedicular screw instrumentation: prospective comparative study with a minimum 2-year follow-up. J Neurosurg Spine, 2014, 20(2):150-156.
[11] Avilés C, Flores S, Molina M. Conservative versus operative treatment for thoracolumbar burst fractures without neurologic deficit. Medwave, 2016, 16(Suppl 1):e6383.
[12] Esses SI, Botsford DJ, Kostuik JP. Evaluation of surgical treatment for burst fractures. Spine, 1990, 15(7):667-673.
[13] Moshirfar A, Jenis LG, Spector LR, et al. Computed tomography evaluation of superior-segment facet-joint violation after pedicle instrumentation of the lumbar spine with a midline surgical approach. Spine, 2006, 31(22):2624-2629.
[14] Verlaan JJ, Diekerhof CH, Buskens E, et al. Surgical treatment of traumatic fractures of the thoracic and lumbar spine: a systematic review of the literature on techniques, complications, and outcome. Spine, 2004, 29(7):803-814.
[15] Assaker R. Minimal access spinal technologies: state-of-theart, indications, and techniques. Joint Bone Spine, 2004, 71(6): 459-469.
[16] Fitschen-Oestern S, Scheuerlein F, Weuster M, et al. Reduction and retention of thoracolumbar fractures by minimally invasive stabilisation versus open posterior instrumentation. Injury, 2015, 46(Suppl 4):S63-70.
[17] Ma YQ, Li XL, Dong J, et al. Comparison of percutaneous versus open monosegment instrumentation in the treatment of incomplete thoracolumbar burst fracture. Zhonghua Yi Xue Za Zhi, 2012, 92(13):904-908.
[18] Lyu J, Chen K, Tang Z, et al. A comparison of three different surgical procedures in the treatment of type A thoracolumbar fractures: a randomized controlled trial. Int Orthop, 2016, 40(6):1233-1238.
[19] Rahamimov N, Mulla H, Shani A, et al. Percutaneous augmented instrumentation of unstable thoracolumbar burst fractures. Eur Spine J, 2012, 21(5):850-854.
[20] Rampersaud YR, Annand N, Dekutoski MB. Use of minimally invasive surgical techniques in the management of thoracolumbar trauma: current concepts. Spine, 2006, 31(11 Suppl): S96-102.
[21] De Iure F, Cappuccio M, Paderni S, et al. Minimal invasive percutaneous fixation of thoracic and lumbar spine fractures. Minim Invasive Surg, 2012, 2012:141032.
[22] Wardlaw D, Cummings SR, Van Meirhaeghe J, et al. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet, 2009, 373(9668):1016-1024.
[23] Briem D, Lehmann W, Ruecker AH, et al. Factors influencing the quality of life after burst fractures of the thoracolumbar transition. Arch Orthop Trauma Surg, 2004, 124(7):461-468.
[24] Wang H, Zhou Y, Li C, et al. Comparison of open versus percutaneous pedicle screw fixation using the sextant system in the treatment of traumatic thoracolumbar fractures. Clin Spine Surg, 2016.
[25] Fitschen-Oestern S, Scheuerlein F, Weuster M, et al. Reduction and retention of thoracolumbar fractures by minimally invasive stabilisation versus open posterior instrumentation. Injury, 2015, 46(Suppl 4):S63-70.
[26] Li H, Yang L, Xie H, et al. Surgical outcomes of miniopen Wiltse approach and conventional open approach in patients with single-segment thoracolumbar fractures without neurologic injury. J Biomed Res, 2015, 29(1):76-82.
[27] Vanek P, Bradac O, Konopkova R, et al. Treatment of thoracolumbar trauma by short-segment percutaneous transpedicular screw instrumentation: prospective comparative study with a minimum 2-year follow-up. J Neurosurg Spine, 2014, 20(2):150-156.
( 本文编辑:王萌 )
Meta-analysis of percutaneous pedicle screw fixation and posterior open pedicle screw fixation in the treatment of thoracolumbar fractures
SUN Xiang-yao, ZHANG Xi-nuo, HAI Yong. Department of Orthopedics, Beijing Chao-
yang Hospital, Capital Medical University, Beijing, 100020, PRC Corresponding author: HAI Yong, Email: spinesurgeon@163.com
Objective To systematically review the clinical results of percutaneous pedicle screw fixation and posterior open pedicle screw fixation for thoracolumbar fractures, and to collect better scientific evidence in the treatment of thoracolumbar fractures. Methods The randomized controlled trials ( RCTs ) were performed to analyze the clinical results of percutaneous pedicle screw fixation and posterior open pedicle screw fixation in the treatment of thoracolumbar fractures. The computer retrieval of Pubmed ( from 1966 to March 2016 ), Cochrane Central Register of Controlled Trails ( CENTRAL ) ( No.3 2016 ) and Embase ( from 1966 to March 2016 ) was performed. The related journals ( from 1990 to March 2016 ) such as the Journal of Bone and Joint Surgery, Spine and European Spine Journal, were manually searched. According to the inclusion and exclusion criteria, the literature was selected independently by 2 professional spinal surgeons. The meta-analysis of all the data was carried out using the Cochrane Collaboration’s RevMan5.3 software. Results Through systematic retrieval and screening, 5 RCTs were identified, with 318 casesin all. There were 158 cases of percutaneous pedicle screw fixation and 160 cases of posterior open pedicle screw fixation. The meta-analysis results showed that shorter surgery time [ WMD = -0.67, 95% CI ( -1.20, -0.14 ), P = 0.01 ], less intraoperative blood loss [ WMD = -2.83, 95% CI ( -4.15, -1.51 ), P < 0.0001 ], lower overall postoperative VAS score [ WMD = -2.79, 95% CI ( -3.80, -1.77 ), P < 0.0001 ], lower VAS score at 3 months after the operation [ WMD = -2.33, 95% CI ( -3.08, -1.58 ), P < 0.00001 ] and shorter hospital length of stay [ WMD = -1.79, 95% CI ( -2.48, -1.11 ), P < 0.00001 ] in the percutaneous pedicle screw fixation group, compared with the posterior open pedicle screw fixation group. No statistically significant differences were found between the 2 groups with regard to VAS score at 1 week after the operation [ WMD = -4.02, 95% CI ( -8.98, 0.94 ), P = 0.11 ], postoperative Cobb’s angle [ WMD = -0.72, 95% CI ( -2.32, 0.89 ), P = 0.38 ], postoperative Cobb’s angle correction loss [ WMD = -0.05, 95% CI ( -0.40, 0.31 ), P = 0.80 ], complication rate [ RR = 0.57, 95% CI ( 0.19, 1.67 ), P = 0.30 ], pedicle screw misplacement rate [ RR = 0.69, 95% CI ( 0.20, 2.37 ), P = 0.55 ] and postoperative infection rate [ RR = 0.34, 95% CI ( 0.04, 3.18 ), P = 0.34 ]. Conclusions Shorter surgery time, less intraoperative blood loss, shorter hospital length of stay and lower VAS score at 3 months after the operation are noticed in percutaneous pedicle screw fixation when compared with posterior open pedicle screw fixation. However, no statistically significant differences are found between the 2 groups with regard to VAS score at 1 week after the operation, postoperative Cobb’s angle, postoperative Cobb’s angle correction loss and complication rate.
Spinal fractures; Thoracic vertebrae; Lumbar vertebrae; Minimally invasive surgical procedures; Meta-analysis
10.3969/j.issn.2095-252X.2016.11.007
R683.2, R687.3
100020 北京,首都医科大学附属北京朝阳医院骨科
海涌,Email: spinesurgeon@163.com
2016-04-15 )
猜你喜欢
中华骨与关节外科杂志(2022年9期)2022-12-22 07:05:14
儿童故事画报(2017年7期)2017-07-19 08:44:02
中国生物医学工程学报(2017年6期)2017-02-10 05:11:53
中华骨与关节外科杂志(2016年6期)2016-05-17 06:11:04
中华骨与关节外科杂志(2016年5期)2016-05-17 06:10:52
中国卫生标准管理(2015年18期)2016-01-20 09:27:00
中国卫生标准管理(2015年5期)2016-01-14 05:17:00
中国继续医学教育(2015年2期)2016-01-06 01:36:20
实用中医药杂志(2015年2期)2015-12-01 07:06:11
四川党的建设(2014年10期)2015-01-26 00:01:16