
A newly developed open-end intracranial hematoma drainage tube
2016-11-16 12:31:36ChaoHeNongnaphatWanussakulDongYangTianyaWuMingZhao
Chao He(✉), Nongnaphat Wanussakul, Dong Yang, Tianya Wu, Ming Zhao
1The People's Hospital of Zhuji, Zhuji 311800, China
2The Second Affiliated Hospital of Zhejiang, Hangzhou 310000, China
A newly developed open-end intracranial hematoma drainage tube
Chao He1(✉), Nongnaphat Wanussakul2, Dong Yang1, Tianya Wu1, Ming Zhao1
1The People's Hospital of Zhuji, Zhuji 311800, China
2The Second Affiliated Hospital of Zhejiang, Hangzhou 310000, China
ARTICLE INFO
Received: 20 May 2016
Revised: 27 May 2016
Accepted: 28 May 2016
© The authors 2016. This article
is published with open access
at www.TNCjournal.com
open-end;
drainage tube;
bullet shape;
barrel;
plunger;
stereotaxic;
drainage matching holes on each side
Objective: To design a new open-end intracranial hematoma drainage tube for clinical application.
Methods: The newly developed device consists of two parts: the plunger and barrel. On one side, the barrel is bullet shaped with an opening tip. The plunger is located in the middle cavity of the tube barrel and extended out at the open-end. It was designed for strengtheningthe tube barrel and for convenience in performing the drainage procedure. It can be used by inserting the drainage tube into the lesion and pulling out the plunger, whereby blood will forcefully rise up inside the barrel, providing a satisfactory outcome. It is made for effusion drainage purposes. During the procedure, the drainage tip is placed at the deepest part of the intracranial hematoma to completely drain the blood. Moreover, the plunger fits tightlyin the tube, preventing leakage during the operation. With the use of the device, brain can be separated. In addition, the device can help reduce the risk of cerebral damage because of the small operating area. The barrel sidewall has matching opening holes bilaterally and equally for exchanging substances between the inner and outer parts. The overlapping ratio in each horizontal pair is around 1/3-1/2. Each pair on the opposite side will form a different pressure. Thus, the opening holes will not easily get blocked with blood clot.
Results: Blood and accumulated liquid from the deepest part of the intracranial hematoma can be directly drawn through the drainage tube withoutdamaging a large area. The tube does not get blocked easily and allows for complete removal of the hematoma.
Conclusions: The device is asuitable instrument for clinical application.
1 Introduction
Hematoma drainage surgery is generally performed in elderly patients with hypertensive or traumatic intracerebral hemorrhage,even in chronic subdural hematoma[1-4]. The original device was widely used in the hematoma drainage surgery treatment technique. However, it has some limitations in usage, which can be classified as follows: (1) the sealing problem of the open-end caused by an occasional but significant blood clot and the inability of the tube to completely draw fluid from the deepest site; (2) improper overlappingof the holes because of the porous design of the device, which can occasionally lead to unfavorable blood clot; (3) the random location of holes in the barrel, which hinders the prediction of the direction of the drawing of blood; and (4) the holes that are easily blocked by blood clot. To avoid the occasional clotting, stereotaxic drainage should be performed at the deepest part of the lesion.
2 Methods
To solve hematoma drainage problems, we designed a new intracranial hematoma drainage tube with an open-end. It is made of the commonly used high- polymer medical material as component. The drainage tube is composed of a plunger and barrel. The front of the bullet-shaped plunger has a cover. Small holes were made at the sidewall of the barrel to allow for exchange of fluid between the inner and outer cavities. The front of the barrel has a small channel that functions as a link between the inner and outer cavities. The plunger is extended from the rear into the middle cavity of the barrel, and part of it is further extended out from the open-end. The sidewall of the barrel will have function of exchanging substance between the opening holes (Figures 1a-c and 2a-c).
The drainage tube is inserted at the site of the hemorrhage, and the plunger is slightly pulled out. After the channels are opened, the negative pressure will draw out all the fluid from the area. If blood clots block the channels, the barrel is removed and inserted again.
Each pair of holes in the barrel will be placed over lapping each other on the horizontal line. The ratio of the overlap is around 1/3-1/2. By placing each hole in this position, the direction of the bloodstream is controlled. Only in the right position will different pressure form, which leads to smooth flow of blood, without the hole being blocked easily (Figure 3a-e).
The rear of the plunger has a rod. In this way, the plunger does not have to be too long and extend out of the barrel. The plunger rod plays a role in fixation by moving in and out of the plunger. Moreover, it can be used for holding, which makes the operation more convenient and stable.
A scale was placed along the sidewall of the barrel. Each unit is marked 1 cmap art, and a longer scale is marked with dots labeled 5, 10, and 15 cm in order to easily identify the depth while using the instrument, for better accuracy and safety (Figure 4a-c).

Figure 1 Vertical view of the drainage tube. a. Bullet-like tip of the drainage tube. b. Tube wall. c. Opening hole. Figure 2 Vertical view of the plunger. a. Bullet-like head of the plunger. b. Plunger body. c. Plunger rod. Figure 3 The plunger inside the barrel in longitudinal section view. a. Head of the plunger. b. Plunger body. c. Barrel wall. d. Opening hole. e. Plunger rod. Figure 4 Parts of the barrel of the drainage tube. a. Long line and dot marker indicating 5cm. b. Barrel wall. c. Scale of 1 cm marked with a short line.
3 Results
The drainage tubes are currently commonly used in clinical approaches. Their advantages include the following: (1) The plunger tip is extended out of the barrel and inserted in the cavity. Owing to the plunger fitted in the opening of the channel of the barrel, the barrel can be closed tightly. Insertion of the device in the barrel has reduced the medical effects and the risks of nerve injuries, as the brain tissue can be separated with in the small operation area. (2) The drainage tube has an open-end tip, which directly draws fluid from the deepest part of the lesion into the stereotaxic drainage. This method can completely drain fluid with high efficacy. (3) The holes on the sidewall of the barrel that overlap each other allow fluid to flow smoothly without being blocked easily. (4) The plunger rod is located at the rear of the plunger, making it easy to perform the drainage procedure (Figures 5a-e and 6a-d).
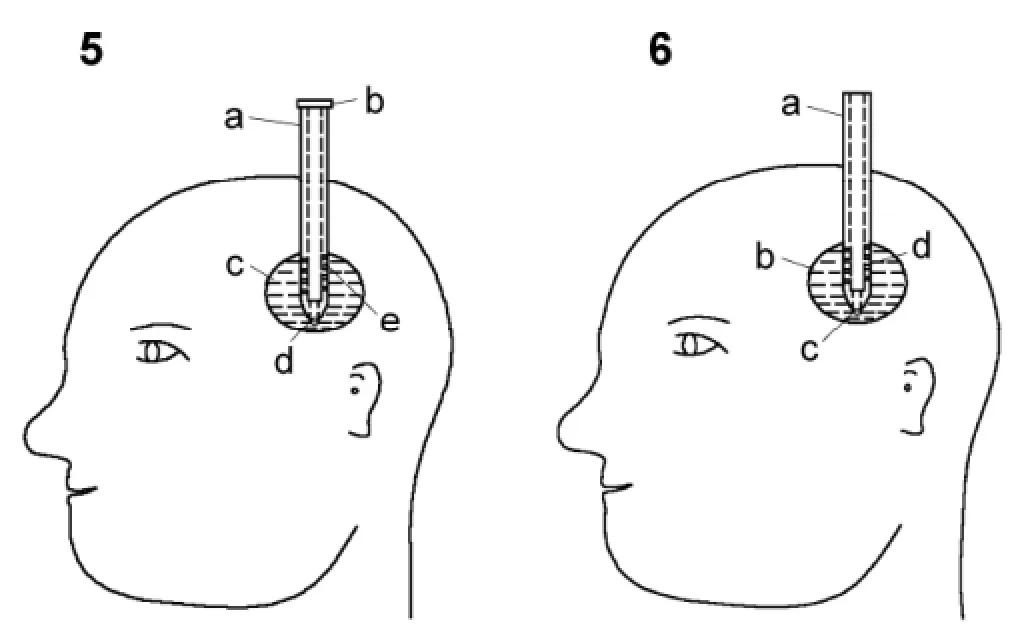
Figure 5 Placement of the drainage tube along with the plunger inside the hemorrhage area. a. Barrel of the drainage tube. b. Plunger rod at the back of the plunger. c. Hematoma cavity. d. Plunger head. e. Opening hole. Figure 6 The drainage tube after removal of the plunger from the hemorrhage area. a. Barrel. b. Hematoma cavity. c. Barrel head. d. Opening hole.
4 Discussion
Intracranial hematoma puncture drainage could not immediately remove the entire hematoma[5, 6].
In order to increase the rate of success of removing the hematoma, improving the clearance rate becomes an important key in achieving the operation goal[7, 8]. Thus, we redesigned the device for a higher clearance rate of removing hematomas. The steps are as follows: Stereotaxic drainage is performed from the open-end, at the deepest part of lesion, to remove fluid smoothly and more efficiently. The overlapping of each hole on the sidewall of the barrel prevents blood clots from blocking the barrel. The aforementioned steps can also be combined with the following steps, at the same time: (1) As the device is heavy, it should be passed through the middle cavity of the hematoma and placed far from the bottom, at around 1 cm. The tube will be used to remove the fluid at the lowest part first and the higher part last. In this way, the hematoma can be removed as much as possible in the shortest time possible. (2) When the condition is suitable, a single hematoma cavity can be injected with urokinase for anticoagulation[9].
In summary, our design of the open-end drainage tube for intracranial hematoma can be used for removing hemorrhage in the cerebral cavity. The elimination rate is high and the risk and complication during operation is low. It is favorable for nerve and tissue remodeling and repair because it is easy to manipulate even if the operation area is small. It is low-cost and suitable for use in general hospitals[10].
Conflict of interests
The authors have no financial interests to disclose regarding the article.
[1] Kalani MYS, Filippidis A, Martirosyan NL, Theodore N. Cerebral herniation as a complication of chest tube drainage of cerebrospinal fluid after injury to the spine. World Neurosurg 2013, 79(5-6): 798.e17-798.e19.
[2] Wang X, Dong Y, Qi XQ, Li YM, Huang CG, Hou LJ.Clinical review: Efficacy of antimicrobial-impregnated catheters in external ventricular drainage—A systematic review and meta-analysis. Crit Care 2013, 17: 234.
[3] Cinibulak Z, Aschoff A, Apedjinou A, Kaminsky J, Trost HA, Krauss JK. Current practice of external ventricular drainage: Asurvey among neurosurgical departments in Germany. Acta Neurochir 2016, 158(5): 847-853.
[4] Feng Y, He JQ, Liu B, Yang LK, Wang YH. Endoscope- assisted keyhole technique for hypertensive cerebral hemorrhage in elderly patients: A randomized controlled study in 184 patients. Turk Neurosurg 2016, 26(1): 84-89.
[5] Jamjoom AAB, Kolias AG, Zaben M, Chari A, Kitchen J, Joannides A, Brennan PM, Kandasamy J, Gatscher S, Gray WP, et al. External ventricular drainage: Is it time to look at national practice? Br J Neurosurg 2015, 29: 9-10.
[6] Fisher CM. Hypertensive cerebral hemorrhage. Demonstration of the source of bleeding. J Neuropathol Exp Neurol 2003, 62(1): 104-107.
[7] Tahir MZ, Sobani ZA, Murtaza M, Enam SA. Long-tunneled versus short-tunneled external ventricular drainage: Prospective experience from a developing country. Asian J Neurosurg 2016, 11(2): 114-117.
[8] Aurangzeb A, Khan SA, Ahmed E, Mehmood S, Ali A, Zadran KK, Hussain S. Predisposing factors, clinical presentation and outcome of repeated aspiration in cerebral abscess through a drainage tube in situ. J Ayub Med Coll Abbottabad 2011, 23(4): 58-60.
[9] Wang K, Du HG, Yin LC, He M, Hao BL, Chen L.Which side of lateral ventricles to choose during external ventricular drainage in patients with intraventricular hemorrhage: Ipsilateral or contralateral? J Surg Res 2013, 183(2): 720-725.
[10] Kirmani A, Sarmast A, Bhat A. Role of external ventricular drainage in the management of intraventricular hemorrhage; its complications and management. Surg Neurol Int 2015, 6(1): 188.
He C, Wanussakul N, Yang D, Wu TY, Zhao M. A newly developed open-end intracranial hematoma drainage tube. Transl. Neurosci. Clin. 2016, 2(2): 150-152.
✉ Corresponding author: Chao He, E-mail: zj.hechao@163.com
Supported by the Zhejiang Province General Medical Health Research Program (No. 2016KYB315).
 Translational Neuroscience and Clinics2016年2期
Translational Neuroscience and Clinics2016年2期
- Translational Neuroscience and Clinics的其它文章
- New frontiers in biomaterials research for tissue repair and regeneration
- Transplantation of neural progenitor cells differentiated from adipose tissue-derived stem cells for treatment of sciatic nerve injury
- A study of the effects of 3,5-diiodo-L-thyronine in the tail suspension and forced swim models of depression
- Behavioral features of mice fed with a cholesterol-enriched diet: Deficient novelty exploration and unaltered aggressive behavior
- Preliminary analysis of cellular sociology of co-cultured glioma initiating cells and macrophages in vitro
- Antiparkinsonian treatment for depression in Parkinson's disease: Are selective serotonin reuptake inhibitors recommended?