探讨甲状腺影像报告和数据系统分级在超声诊断甲状腺癌中的应用价值
2016-11-10 08:18:20顾士荣
肿瘤影像学 2016年3期
顾士荣
上海市松江区方塔中医医院超声科,上海 201699
探讨甲状腺影像报告和数据系统分级在超声诊断甲状腺癌中的应用价值
顾士荣
上海市松江区方塔中医医院超声科,上海 201699
目的:探讨甲状腺影像报告和数据系统(Thyroid Imaging Reporting and Data System,TI-RADS)分级对诊断甲状腺癌中的应用价值。方法:选择甲状腺结节患者75例并进行外科手术或细针穿刺活检(fine needle aspiration,FNA),应用高频彩色多普勒超声对双侧甲状腺进行扫查。根据TI-RADS对甲状腺结节分级,选择TI-RADS 3~5级的患者63例(81个病灶),将甲状腺 TI-RADS 分级情况与病理切片结果进行比较和分析,评估 TI-RADS 分级对鉴别甲状腺癌的效能。结果:在63例患者(81个病灶)中,病理学活检结果显示,28个TI-RADS 3级病灶中,良性23个(82.14%)、恶性5个(17.86%);32个TI-RADS 4级病灶中,良性5个(15.63%)、恶性27个(84.37%);21个TI-RADS 5级病灶中,良性0个(0)、恶性21个(100%)。TI-RADS分级诊断甲状腺癌的灵敏度和特异度分别为88.67%和82.14%。TI-RADS 3~5级病灶的纵横比边缘、边界、钙化、血管充盈、血流阻力指数(resistance index,RI)值差异均有统计学意义(P<0.01)。结论:TI-RADS分级诊断甲状腺癌的灵敏度和特异度较高。在高频超声检查甲状腺中,应用TI-RADS分级对诊断甲状腺癌具有重要临床意义。
甲状腺结节;超声;甲状腺影像报告和数据系统
近年来甲状腺结节的发现率越来越高,过去10年中甲状腺恶性结节发病率和检出率的上升幅度居所有癌症之首[1-2]。随着甲状腺癌患病的年轻化,其早期诊断和及时手术治疗成为研究的热点。超声检查已成为诊断和治疗甲状腺结节的重要影像学手段[3-4]。甲状腺癌的淋巴转移或其他远处转移途径将引起病情恶化,降低患者手术后生存率,因此其早期明确诊断对预后显得尤为重要。据文献报道,应用高频彩色多普勒超声,参照甲状腺影像报告和数据系统(Thyroid Imaging Reporting and Data System,TI-RADS)分级诊断标准,可降低超声科医师判断的主观性,显著提高甲状腺癌的诊断率[5]。本研究应用高频彩色多普勒超声分析63例甲状腺癌患者,旨在探讨其鉴别甲状腺肿瘤良恶性的应用价值。
1 资料和方法
1.1临床资料
选择2012年10月—2014年6月患有甲状腺结节并接受外科手术或细针穿刺活检的患者75例,年龄18~73岁,平均(43±12.14)岁,其中18~33 岁21例、34~45岁31例、46~60岁15例、61~73岁8例。手术前对所有研究对象的双侧甲状腺进行高频彩色多普勒超声检查,共发现92个病灶,同时采用超声TI-RADS进行分级和评价,选取TI-RADS 3~5级的63例患者(81个病灶)进行分析。
1.2仪器和方法
采用ESAOTE Mylab90、PHILIPS iU22彩色超声诊断仪,线阵探头频率7.5~13.0 MHz。患者静息状态下,仰卧位暴露颈部。探头轻触甲状腺表面,二维超声观察甲状腺质地,注意甲状腺结节的数量、分布、边缘、边界、内部回声、后方回声有无衰减、内部有无钙化等。选取结节最大长轴切面图像最清楚时测量大小,然后用彩色多普勒观察结节内部及周边血流分布,并记录结节内部血管血流的阻力指数(resistance index,RI)。
1.3TI-RADS分级诊断标准[5]
甲状腺TI-RADS诊断标准分为5级。0级:无结节,正常甲状腺或弥漫性增生性甲状腺;1级:高度提示良性,以囊性为主,有声晕;2级:可能良性,边缘界限清楚,以实性为主,回声不均匀,等回声或高回声,蛋壳样钙化或粗钙化;3级:不确定,回声均匀,低回声,边缘光整,实性,纵横比>1,无其他提示恶性的超声图像;4级:可能恶性,l~2项提示恶性的超声表现,如极低回声、微钙化、边缘不光整、淋巴结异常;5级:高度提示恶性,超过3项提示恶性的超声表现,如极低回声、微钙化、边缘不光整、边界不清、淋巴结异常等。以1~3级评判为良性,4~5级评判为恶性。
1.4统计学处理
应用SPSS 18.0软件进行统计学分析,对TI-RADS 3~5级病灶特征的计数资料行χ2检验,P<0.05为差异有统计学意义。
2 结 果
2.1按TI-RADS分级诊断标准的超声表现
根据TI-RADS分级诊断标准,对81个甲状腺病灶的边缘、边界、回声、周围组织、钙化、血管分布、血流RI值(RI≥0.7作为诊断甲状腺癌的界值)进行评估,TI-RADS 3级病灶有28个、4级32个、5级21个。结果显示,TI-RADS 3~5级甲状腺病灶的纵横比、边缘、边界、钙化、血管充盈、血流RI值差异均有统计学意义(P<0.01),但形状和回声性质差异无统计学意义(P>0.05)(表1)。
2.2甲状腺病灶TI-RADS 3~5分级与病理结果比较
经术后病理检查证实共81个病灶,其中良性28个、恶性53个(表2)。良性肿瘤包括甲状腺囊腺瘤11个、炎性病变7个、甲状腺腺瘤样增生4个,其余6个病灶为增生性病变;恶性肿瘤包括乳头状癌33个、滤泡状癌12个、髓样癌5个、未分化癌2个、鳞状细胞癌1个。63例甲状腺疾病患者的81个甲状腺病灶中,病理学活检结果显示28个TI-RADS 3级病灶,其中良性23个(82.14%)(图1、2)、恶性5个(17.86%);病理学活检结果显示32个TI-RADS 4级病灶,其中良性5个(15.63%)、恶性27个(84.37%)(图3、4);病理学活检结果显示21个TI-RADS 5级病灶,其中良性0个(0)、恶性21个(100%)。TI-RADS分级诊断标准判断甲状腺癌的阳性预测值为90.51%,灵敏度为88.67%,特异度为82.14%。
3 讨 论
在各种影像学检查手段中,超声对甲状腺结节的灵敏度较高[6],对早期甲状腺癌的检出具有重要意义。在以往常规超声诊断中,甲状腺结节是根据形态学特征来进行良恶性鉴别[7],在一定程度上依赖超声科医师的工作经验和操作熟练度,因此结果主观性较强。临床医师很难依据含糊的超声报告确定肿瘤性质和决定治疗方案,可能严重延误疾病的治疗。有研究[5,8]借鉴美国放射学会制定的乳腺影像学报告及数据系统(Breast Imaging Reporting and Data System,BI-RADS),对甲状腺结节进行标准化的分级评估,制定了TI-RADS以提高诊断符合率及准确率。依据超声TI-RADS分级,采用高频彩色多普勒超声对甲状腺疾病进行检查,不仅可减低良性肿瘤穿刺活检,还可为早期诊断和治疗争取更多的时间,从而提高患者的生存率。
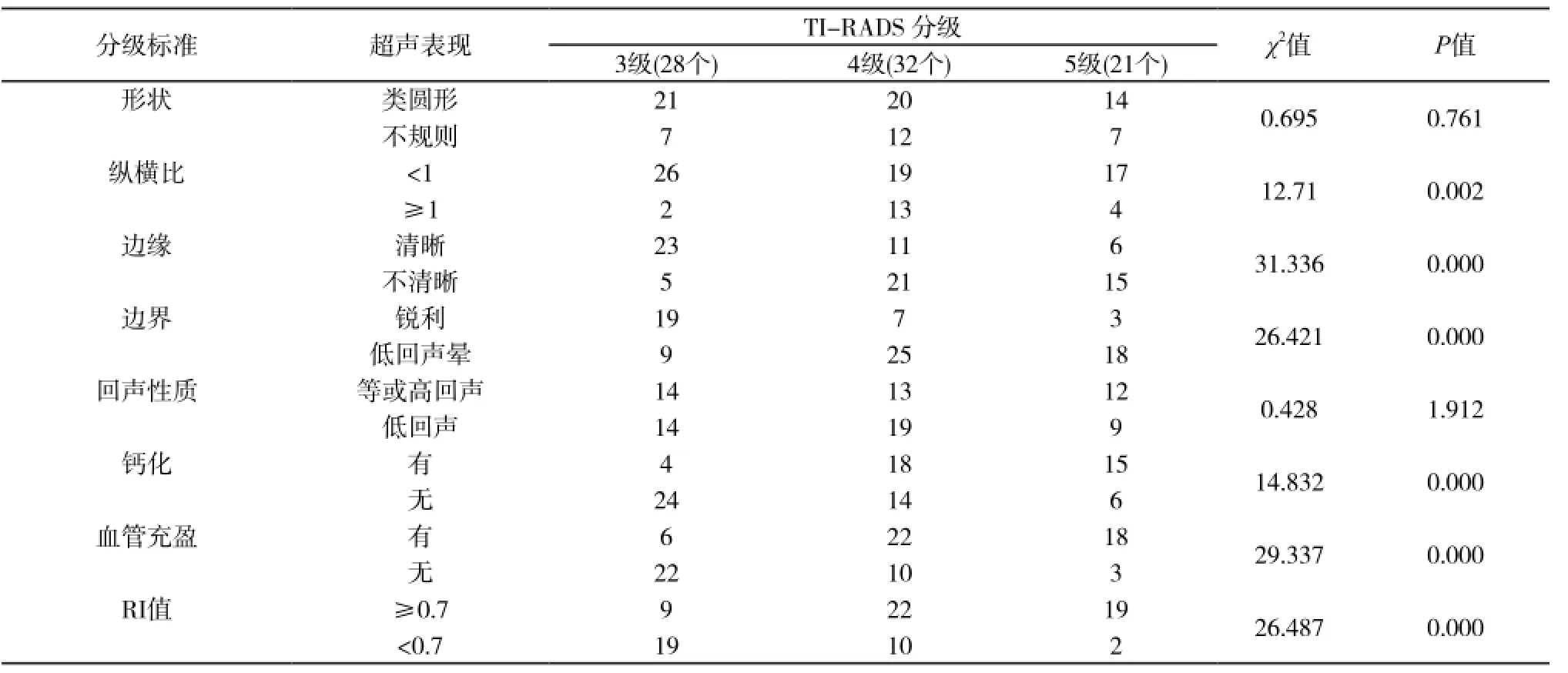
表1 TI-RADS 3~5级诊断标准的超声表现

表2 TI-RADS 3~5级与病理结果比较
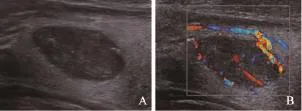
图1 TI-RADS 3级腺瘤性甲状腺肿超声及CDFI表现
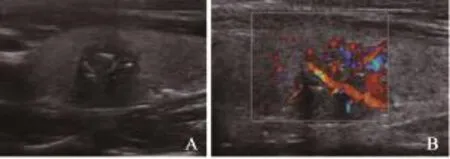
图2 良性结节性甲状腺肿病理表现(HE,×200)
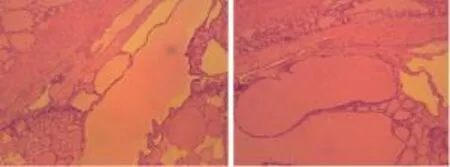
图3 TI-RADS 4级甲状腺癌超声及CDFI表现
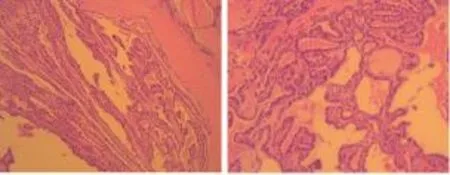
图4 恶性甲状腺癌(乳头状癌)病理表现(HE,×200)
有研究[9]表明,TI-RADS评分3、4和5级甲状腺结节中恶性者分别占33.3%、86.8%和100%。本研究81个结节中,TI-RADS评分3、4和5级的甲状腺结节恶性率分别为17.86%、84.37%、100%,与报道基本一致。本研究结果显示,TI-RADS 3~5级病灶的纵横比、边缘、边界、钙化、血管充盈、血流RI值差异均有统计学意义,表明超声表现可指导 TI-RADS对甲状腺病灶的具体分级,从而减少主观判断,增加客观判断依据,有助于提高甲状腺癌的诊断率。然而,病灶的形状和回声性质差异无统计学意义,表明这些超声表现不是区分TI-RADS 3~5级的必要依据。在63例患者(81个病灶)中,病理学活检结果表明,28个TI-RADS 3级病灶中,良性23个(82.14%)、恶性5个(17.86%);32个TI-RADS 4级病灶中,良性5个(15.63%)、恶性27个(84.37%);21个TI-RADS 5级病灶中,良性0个(0)、恶性25个(100%)。TI-RADS分级诊断甲状腺癌的灵敏度和特异度分别为88.67%和82.14%,表明在高频超声检查甲状腺时,应用TI-RADS分级标准确实可降低医师的主观性,将超声报告统一标准化和准确化,且该分级诊断方法对鉴别诊断甲状腺疾病的良恶性具有较好的判断效能,为临床提供准确可靠的依据。
综上所述,TI-RADS分级标准使高频彩色多普勒超声检查对甲状腺疾病的定性更趋客观,并为甲状腺癌早期发现和诊断、早期手术治疗提供了可靠依据。超声科医师可根据 TIRADS分级诊断标准制订评估分界线,以降低主观干扰,提高甲状腺恶性结节普查的诊断率,以期早期手术治疗而提高患者的生存率。
[1] 郭民英. Polo样激酶和Ki-67在甲状腺癌中的表达及其病理意义研究 [J]. 中国全科医学, 2011, 14 (3): 975.
[2] GRUBBS E G, RICH T A, LI G, et al. Recent advances in thyroid cancer [J]. Curr Probl Surg, 2008,45(3): 156-250.
[3] JIANG Y X, ZHANG B. Ultrasonic diagnosis and treatment of thyroid nodule [J]. Med J Pek Union Med Coll Hosp, 2010, 1(1): 34-39.
[4] FAN Z P, QIAO Z, WU J D. Analysis on diagnosis and relapse factors of thyroid gland cancer [J]. Chin J Bases Clin General Surg, 2010, 17(1): 68-72.
[5] PARK J Y, LEE H J, JANG H W, et al. A proposal for a thyroid imaging reporting and data system for ultrasound features of thyroid carcinoma [J]. Thyroid, 2009, 19(11): 1258-1264.
[6] ZHAO L J, ZHOU Y Y, ZHANG R F, et al. High frequency color Doppler in the diagnosis of benign and malignant thyroid nodules [J]. J Zhengzhou Univ (Med Sci), 2009, 44(6): 1284.
[7] ZHANG B, JIANG Y X, DAI Q, et al. Logistic regression analysis of the features of thyroid nodules on gray scale and color Doppler ultrasound [J]. Chin J Ultrasonogr, 2008,17(12): 106l-1065.
[8] HORVATH E, MAJLIS S, ROSSI R, et al. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management [J]. J Clin Endocrinol Metab, 2009, 94(5): 1748-1751.
[9] MA B Y, SUNDAR P S, PENG Y L, et al. The value of sonography in thyroid imaging reporting and data system for thyroid nodule [J]. Chin J Bases Clin General Surg,2011, 18(8): 898-901.
Role of Thyroid Imaging Reporting and Data System category in ultrasonic diagnosis of thyroid cancer
GUShirong (Department of Ultrasound, Fangta Hospital of Traditional Chinese Medicine of Songjiang District, Shanghai 201699, China)
Correspondence to: GU Shirong E-mail: gsr196825@sina.com
Objective: To study the role of Thyroid Imaging Reporting and Data System (TI-RADS) category in ultrasonic diagnosis of thyroid cancer. Methods: A total of 75 patients with thyroid diseases who underwent surgery or fine needle aspiration(FNA) were selected. All the patients underwent thyroid examination with high-frequency color Doppler ultrasonography. According to TI-RADS category, 63 patients (81 thyroid lesions) with TI-RADS grade 3-5 were recruited. The characteristics of highfrequency color Doppler ultrasonography in diagnosis of thyroid lesions with different TI-RADS grades were compared with the histopathological results. Then the efficacy of TI-RADS category in the identification of thyroid cancer was assessed. Results: In all 63 patients (81 thyroid lesions) confirmed by histopathology, 28 lesions were TI-RADS grade 3, in which 23 (82.14%) were benign,5 (17.86%) were malignant; 32 lesions were TI-RADS grade 4, and histopathology confirmed 5 (15.63%) were benign, 27 (84.37%)were malignant; 21 lesions were TI-RADS grade 5, and all the lesions were malignant confirmed by histopathology (100%). The sensitivity and specificity were 88.67% and 82.14% respectively in the diagnosis of thyroid cancer by TI-RADS category. Statistical differences were found among thyroid lesions with TI-RADS grades 3, 4, 5 in A/T, margin, boundary, calcification, vascularity and blood flow and resistance index (RI). Conclusion: The sensitivity and specificity of TI-RADS category are high in diagnosing thyroid cancer by high-frequency color Doppler ultrasound.
Thyroid nodule; Ultrasonography; Thyroid Imaging Reporting and Data System
R445.1
A
1008-617X(2016)03-0279-04
顾士荣 E-mail:gsr196825@sina.com
(2016-02-16
2016-05-17)
猜你喜欢
中老年保健(2022年6期)2022-08-19 01:41:22
内蒙古林业(2021年6期)2021-06-26 10:42:32
国际放射医学核医学杂志(2021年10期)2021-02-28 08:43:46
国际放射医学核医学杂志(2021年10期)2021-02-28 08:43:24
中国交通信息化(2019年2期)2019-03-25 03:20:12
中国设备工程(2019年8期)2019-01-17 11:16:42
自动化学报(2017年5期)2017-05-14 06:20:51
中国卫生(2016年9期)2016-11-12 13:28:08
中国卫生标准管理(2015年2期)2016-01-15 00:31:34
中国继续医学教育(2015年1期)2016-01-06 01:36:04