超声对类风湿关节炎的诊断价值
2016-10-19 11:13白超赵娜李霞张文焕蒋雪梅
中国中西医结合影像学杂志 2016年4期
白超,赵娜,李霞,张文焕,蒋雪梅
(1.山东中医药大学第一临床学院,山东济南250014;2.山东中医药大学附属医院超声科,山东济南250014)
超声对类风湿关节炎的诊断价值
白超1,赵娜1,李霞1,张文焕2,蒋雪梅2
(1.山东中医药大学第一临床学院,山东济南250014;2.山东中医药大学附属医院超声科,山东济南250014)
目的:观察类风湿关节炎(rheumatoid arthritis,RA)患者各关节的多普勒超声改变,评估多普勒超声对关节炎的诊断价值。方法:回顾性分析54例疑似RA患者,采用高频超声扫查双膝关节、双腕关节、双手掌指关节、双手近端指间关节、双踝关节,评估各关节滑膜厚度、关节积液、血流信号及骨侵蚀程度。结果:54例超声共扫查关节1 188个,统计病变关节,双手第2~5掌指关节占20%(87/432),双手第2~5近端指间关节占17.6%(76/432),双腕关节占56.5%(61/108),双踝关节50/108(46.3%),双膝关节66/108(61.1%)。超声提示RA 37例,非RA 17例,另有4例超声未见明显的RA征象,但临床诊断为RA。临床诊断39例RA,非RA 15例,超声诊断RA的灵敏度为89.7%(35/39),特异度为73.3%(11/15),阳性预测值94.6%(35/37),阴性预测值76.5%(13/17)。超声诊断RA与临床诊断结果进行对照分析,K=0.734(0.7<K≤0.8),Z=5.415,P=0.000<0.05,即2种方法一致性较高。结论:超声对早期RA炎症活动具有较强的敏感性,且可靠、便捷、安全,与临床评估结果具有高度相似性,其与临床评估相结合,可提高诊断准确性。
关节炎,类风湿;超声检查
[Abstract]Objective:To observe the changes of Doppler ultrasound in patients with rheumatoid arthritis(RA),and to evaluate the predictive value of Doppler ultrasound parameters in the joint inflammation.Methods:We performed a retrospective analysis of 54 cases of suspected patients with RA,using high frequency ultrasound scanning metacarpophalangeal joints,wrists joints,proximal interphalangeal joint,double ankle,knee joints,evaluated the synovial thickness,joint effusion,blood flow signals and the degree of bone erosion.Results:1188 joints of 54 cases were scaned.Statistics of the joints of the lesions:MCP 87/432(20%),PIP 76/432(17.6%),wrists joints 61/108(56%),double ankle 50/108(46%),double knee joints 66/108(61%).US examination showed 37 cases of RA,17 cases of non-RA.There were 4 cases of US examination showed no obvious RA signs,but the clinical diagnosis was RA.The clinical diagnosis was 39 cases of RA,15 cases of non-RA.The sensitivity of RA was 89.7%(35/39),specificity was 73.3% (11/15),RA forecast value 94.5% (35/37),non-RA forecast value 76.5% (13/17).The comparative analysis of US diagnosis and clinical diagnosis showed:Kappa=0.734(0.7<k≤0.8),z=5.415,P=0.000<0.05,which means that two methods(US diagnosis and clinical diagnosis)had high consistency.Conclusion:①Ultrasound has a strong sensitivity to early RA inflammatory activity,and its method is reliable,convenient and safe.The results of the assessment are of predictive value in the diagnosis of disease activity and imaging findings.②The results of ultrasound assessment are highly similar with the clinical evaluation results.③In the identification of patients with RA,Doppler ultrasound combined with clinical assessment can more accurately reflect the disease activity of inflammation.
[Key words]Arthritis,rheumatoid;Ultrasonography
类风湿关节炎(rheumatoid arthritis,RA)是一种以关节炎症为主的异质性、系统性、自身免疫性疾病。主要侵犯全身各处关节,可导致永久性结构损伤。其病理特点为侵蚀关节滑膜、炎性细胞浸润、血管形成、破坏关节软骨、肌腱受到侵烛,最终导致关节软骨、骨质及关节囊被破坏。主要临床表现为关节肿痛、僵直、畸形、功能障碍,也可引起腕管/跗管综合征、腘窝囊肿、类风湿血管炎等,甚至累及肾脏、神经系统、心脏、呼吸系统等[1]。因此,准确评估关节炎症疾病的程度对RA早诊断、早治疗至关重要。多普勒超声不仅可检测滑膜炎,并可评估结构损伤,是诊断早期RA的重要检查方法。
1 资料与方法
1.1一般资料收集山东中医药大学附属医院2015年3—10月风湿免疫门诊疑诊为RA患者54例,其中男11例,女43例;年龄10~79岁,平均45.68岁,男女比例4∶1;正在服用抗风湿药物早期RA患者15例。
1.2诊断标准
1.2.1超声诊断标准采用Szkudlarek等[2]提出的半定量分级系统。①滑膜分级:0级,无滑膜增生;Ⅰ级,可见滑膜填充于关节周围骨之间,但不超过骨面最高点连线;Ⅱ级,滑膜明显增厚且超过骨面最高点连线,但不超过骨干;Ⅲ级,滑膜组织增厚,超过骨面最高点连线与一侧骨干。②滑膜内血流信号分级:0级,滑膜内未见血流信号;Ⅰ级,滑膜增生并见点状血流信号;Ⅱ级,增生滑膜内见条状血流信号,其充盈面积低于滑膜面积的一半;Ⅲ级,增生滑膜内见面积大于滑膜面积一半及以上的条状丰富血流信号,甚至血流信号充填于增生滑膜。③骨侵蚀分级:0级,骨皮质光滑且无骨质破坏;Ⅰ级,骨皮质毛糙、不平整,骨质尚连续,无明显中断或缺失,骨质轻度破坏;Ⅱ级,骨皮质表面连续性明显中断或缺失,可见骨质破坏;Ⅲ级,骨表面不平整,骨质严重破坏。④积液分级:0级,未见积液;Ⅰ级,可见少量积液;Ⅱ级,可见明显积液,关节囊无肿胀;Ⅲ级,大量积液并关节囊肿胀。
1.2.2临床诊断标准研究表明[3],RA分类标准1987 ACR和2010 ACR/EULAR存在不一致,本研究采用1987 ACR[4]作为研究标准。
1.3仪器与方法采用GE Logiq S8彩色超声诊断仪,探头频率6~15 MHz,Siemens 2 000,探头选择频率5~12 MHz。患者取舒适体位,充分暴露受检部位,采用适量耦合剂(厚约2 mm),探头轻触关节(尤其在显示滑膜血流时,不可加压)。扫查双手第2~5掌指关节(metacarpophalangeal joints,MCP)背侧和掌侧;第2~5近端指间关节(proximal interphalangeal joints,PIP)(不包括远端指骨间关节)的背侧、指掌侧、桡、尺侧方面;双膝关节髌上囊、双腕关节背侧、指掌侧、桡、尺侧方面;双踝关节内踝、外踝。评估每个关节,统计病变关节,确定数量和半定量分级,评估各关节滑膜肥厚度、关节积液、血流信号及骨侵蚀程度。通过半定量分级系统判定,并与临床诊断结果进行对比。
1.4统计学方法采用SPSS 17.0软件进行数据分析。对超声检查结果与临床诊断结果行Kappa一致性检验、独立性检验、关联程度及优势性检验。标准:K值范围在(-1,1),若观察一致率大于机遇一致率,则K值范围在(0,1),K值为0,结果为机遇造成;K值为-1则完全不一致,K值越接近1,一致性越好,K值=1则完全一致;0<K≤0.4为一致性低,0.4<K≤0.5为一致性一般,0.5<K≤0.7为一致性良好,0.7<K≤0.8为一致性较高,0.8以上为一致性高。独立性P<0.05,2种方法相互独立。关联系数rp范围(0,1),0<rp≤0.4为关联程度低,0.4<rp≤0.5为关联程度一般,0.5<rp≤0.7为关联程度良好,0.7<rp≤0.8为关联程度较高,0.8以上为关联程度高。优势性检验以P<0.05为差异有统计学意义。
2 结果
超声提示RA 37例,其中男9例,女28例;非RA 17例,其中男3例,女14例。临床诊断RA 39例,男9例,女30例;非RA 15例,男3例,女12例。
54例共扫查关节1 188个,统计其中病变关节:双手MCP检出率20.1%(87/432),双手PIP检出率17.6%(76/432),双腕检出率56.5%(61/108),双踝检出率46.3%(50/108),双膝检出率61.1%(66/108)。半定量分级系统统计结果见表1。
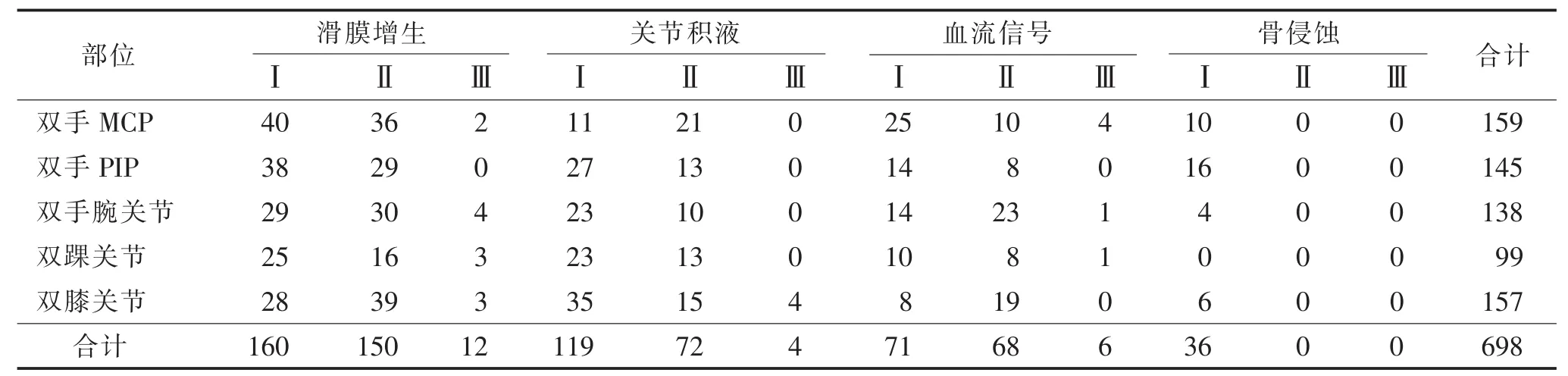
表1 半定量分级系统统计结果
双手MCP各项指标占22.8%(159/698),双手PIP各指标占20.8%(145/698),双手腕关节各指标占19.8%(138/698),双踝关节各指标占14.2%(99/698),双膝关节各指标占22.5%(157/698)。
所有部位滑膜增生Ⅰ级占22.9%(160/698),Ⅱ级占21.5%(150/698),Ⅲ级占1.8%(12/698);关节积液级Ⅰ级占17.0%(119/698),Ⅱ级占10.3%(72/698),Ⅲ级占0.6%(4/698);血流信号Ⅰ级占10.2%(71/698),Ⅱ级占9.7%(68/698),Ⅲ级0.9%(6/698);骨侵蚀Ⅰ级占5.2%(36/698),无Ⅱ级和Ⅲ级。
超声与临床诊断RA的对照见表2。超声诊断RA的灵敏度为89.7%(35/39),特异度为73.3%(11/15),阳性预测值94.6%(35/37),阴性预测值76.5%(13/17)。超声诊断RA与临床诊断分析对比,结果显示:①K=0.734(0.7<K≤0.8),Z=5.415,P=0.000,即超声与临床诊断2种方法一致性较高。②Pearsonχ2=29.323,v=1,P=0.000,2种方法相互独立。③列联系数rp= 0.593,P=0.000,0.5<rp≤0.7为关联程度良好,超声与临床诊断2种方法关联程度良好。④优势性检验:P=0.687,2种方法在RA检测中,互有优势,差异无统计学意义。
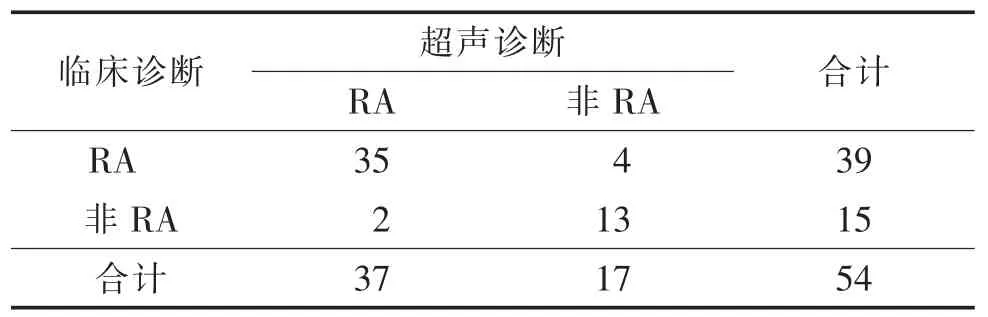
表2 超声与临床诊断RA结果的对照例
3 讨论
RA被称为不死的癌症,其主要治疗目标是缓解症状,随着生物疗法的应用,临床缓解率明显提高[5]。RA对患者心理困扰也较严重,因此,除药物治疗缓解症状外,还需定期监测患者的心理[6]。此外,炎性风湿性疾病的早期鉴别诊断也非常重要,Sorensen等[7]分析了RA、银屑病关节炎(psoriatic arthritis,PSA)和强直性脊柱炎(ankylosing spondylitis,AS)的初始症状和诊断,阐释了早期诊断的重要性。也有学者[8]利用超声对PSA进行了评分,这对RA和PSA的鉴别起到了一定作用。约80%的RA患者血液中有类风湿因子(rheumatoid factors,RF)、IgM、IgG、IgA及抗环状瓜氨酸(CCP)抗体等,20%的患者有类风湿结节[9]。但仍有部分患者依据临床及实验室检查无法明确诊断。在过去的几年中,肌肉骨骼超声(musculoskeletal ultrasound,MSU)已被证明不仅能检测关节和关节周围炎(滑膜炎、腱鞘炎及滑囊炎),而且在评价结构损伤、检测关节肿胀程度方面比临床评估更敏感[10],有助于RA的早期诊断;在检测骨质侵蚀的程度方面MSU比常规X线摄影更敏感,还可监测治疗效果,也是指导注射治疗的重要工具。
X线摄影曾经在早期RA的影像学检查中广泛使用,但对RA不是很敏感[11-12]。MRI检测炎症和关节损伤虽较敏感[13],但成本高,检查时间长,因此,超声越来越多地用来评价RA。
我们尽量最小化这项研究的一些不足之处,如vander Heijde[14]指出RA足部关节的侵蚀早于手部关节;男性类风湿性关节炎患者比例较低,以及治疗与非治疗患者无区别扫描,但以上细微的差异在RA严重程度的评估中,不足以影响其研究的结果。相关研究[15]表明,大关节经常参与风湿性疾病(本研究中双膝关节病变占61.1%)。
本研究中超声能够精确评估滑膜肥厚度、血流信号、骨侵蚀程度。各项指标Ⅰ级在本指标中所占的比例最高,滑膜增生Ⅰ级占22.9%、积液Ⅰ级占17.0%、血流信号Ⅰ级占10.2%、骨侵蚀Ⅰ级占5.2%。各部位损伤中最高为MCP(22.8%)及膝关节(22.5%),最低为踝关节(14.2%),由于未检测跖趾关节,因此难以确定RA病变在上下肢的分布。多普勒超声对RA的诊断与临床诊断具有高度一致性,有助于治疗方案制订及疗效评估。我们将进一步细化检查,开展超声DAS28评分[16],为临床提供更加客观的诊断依据。总之,超声具有可重复性、高分辨力、价廉的优势,在一定程度上还会起到治疗作用,对肩关节疼痛、骨性关节炎及RA等疼痛性疾病具有确切的效果[17]。

图1 女,47岁,左侧腕关节滑膜增生Ⅱ级,积液Ⅰ级,血流信号Ⅱ级,骨侵蚀Ⅰ级图2女,61岁,左膝关节滑膜增生Ⅱ级,积液Ⅰ级,血流信号Ⅱ级,软骨变薄图3男,42岁,左侧外踝关节滑膜增生Ⅱ级,积液Ⅱ级,血流信号Ⅲ级
[1]Bridges SL.National Institute of Arthritis and Musculoskeletal and Skin Diseases[J].中华内科杂志,2010,49(12):1014.
[2]Szkudlarek M,Court-Payen M,Jacobsen S,et al.Interobserver agreement in ultrasonography of the finger and toe joints in rheumatoid arthritis[J].Arthritis Rheum,2003,48:955-962.
[3]Kasturi S,Goldstein BL,Malspeis S,et al.Comparison of the 1987 American College of Rheumatology and the 2010 American College of Rheumatology/European League against Rheumatism criteria for classification of rheumatoid arthritis in the Nurses' Health Study cohorts[J].Rheumatol Int,2014,34:407-411.
[4]Arnett FC,Edworthy SM,Bloch DA,et al.The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis[J].Arthritis Rheum,1988,31:315-324.
[5]Gul HL,Ferreir JF,Emery P.Remission in rheumatoid arthritis:is it all the same[J].Expert Rev Clin Pharmacol,2015,8:575-586.
[6]Bode C,Taal E,Wright JD.Rheumatoid arthritis:psychosocial aspects[J].International Encyclopedia of the Social&Behavioral Sciences,2015,69:655-659.
[7]Sorensen J,Hetland ML.Diagnostic delay in patients with rheumatoid arthritis,psoriatic arthritis and ankylosing spondylitis:results from the Danish nationwide DANBIO registry[J].Ann Rheum Dis,2015,74:e12
[8]Ficjan A,Husic R,Gretler J,et al.Ultrasound composite scores for the assessment of inflammatory and structural pathologies in Psoriatic Arthritis(PsASon-Score)[J].Arthritis Res Ther,2014,16:476.
[9]Brasington RD.85-Clinical features of rheumatoid arthritis[M]// Hochberg MC.Rheumatology.6th ed.Philadelphia:Elsevier Ltd. 2015:704-711.
[10]Szkudlarek M,Klarlund M,Narvestad E,et al.Ultrasonography of the metacarpophalangeal and proximal interphalangeal joints in rheumatoid arthritis:a comparison with magnetic resonance imaging,conventional radiography and clinical examination[J]. Arthritis Res The,2006,8:R52.
[11]McGonagle D,Conaghan PG,Wakefield R,et al.Imaging the joints in early rheumatoid arthritis[J].Best Pract Res Clin Rheumatol,2001,15:91-104.
[12]Naváez García JAN.Evaluation through imaging of early rheumatoid arthritis[J].Reumatol Clin,2010,6:111-114.
[13]фstergaard M,Axelsen MB,Boesen M.Magnetic resonance imaging in rheumatoid arthritis[M]//Atlas of Rheumatoid Arthritis. Springer Healthcare Ltd.,2015:125-140.
[14]van der Heijde DM.Joint erosions and patients with early rheumatoid arthritis[J].Br J Rheumatol,1995,34(suppl 2):74-78.
[15]Scirè CA,Iagnocco A,Meenagh G,et al.Ultrasound imaging for the rheumatologist.XXVIII.Impact of sonographic knee joint involvement in recent-onset inflammatory polyarthritis[J]. Clin Exp Rheumatol,2010,28:449-453.
[16]Glasnovic,Bosnjak I,Vcev A,et al.Anti-citrullinated antibodies,radiological joint damages and their correlations with disease activity score(DAS28)[J].Coll Antropol,2007,31:345-348.
[17]Sengul I,Akcay-Yalbuzdag S,Ince B,et al.Comparison of the DAS28-CRP and DAS28-ESR in patients with rheumatoid arthritis[J].Int J Rheum Dis,2015,18:640-645.
Prediction and diagnostic value of ultrasound in the diagnosis of rheumatoid arthritis
BAI Chao,ZHAO Na,LI Xia,ZHANG Wenhuan,JIANG Xuemei.The First Clinical Medical College,Shandong University of Traditional Chinese Medicine,Jinan,250014,China.
2016-01-10)
10.3969/j.issn.1672-0512.2016.04.012
中国中医科学院计划项目(2013BA102B06)。
蒋雪梅,E-mail:jxm6612@163.com。
猜你喜欢
舰船科学技术(2022年10期)2022-06-17
中国典型病例大全(2022年11期)2022-05-13
建材发展导向(2021年14期)2021-08-23
护理实践与研究(2021年15期)2021-08-06
中国生殖健康(2019年3期)2019-02-01
中成药(2018年12期)2018-12-29
大众健康(2016年6期)2016-08-03
中国民族民间医药·下半月(2014年2期)2014-09-26
中医研究(2014年11期)2014-03-11
中医研究(2014年5期)2014-03-11