
多种中药制剂联合应用治疗儿童手足口病临床研究
2016-09-24 01:38朱艳辉宋宏玲
中国妇幼健康研究 2016年2期
朱艳辉,宋宏玲
(首都医科大学附属北京儿童医院急诊科,北京 100045)
多种中药制剂联合应用治疗儿童手足口病临床研究
朱艳辉,宋宏玲
(首都医科大学附属北京儿童医院急诊科,北京 100045)
目的观察痰热清联合喜炎平及康复新液治疗普通型儿童手足口病的临床疗效。方法选取首都医科大学附属北京儿童医院2012年1月至2012年12月符合标准的60例普通型手足口病患儿随机分成治疗组和对照组,两组均采用退热、补液、支持和加强护理等综合治疗。治疗组每日静点痰热清注射液及喜炎平注射液,并给予康复新液口腔含服并外擦手、足、臀部皮疹;对照组每日静点病毒唑针剂,并给予阿昔洛韦乳膏涂擦皮疹,两组治疗7天为一个疗程,观察两组患儿体温下降及口腔疱疹、皮疹消退的情况。结果治疗组治疗7天后总有效率为100.00%;对照组治疗7天后总有效率为80.00%,两组差异有统计学意义(χ2=6.67,P<0.01)。治疗组患儿热退时间、口腔疱疹及皮疹消退时间、可进食时间分别为2.0±0.8天、3.1±1.1天、2.0±0.8天,对照组患儿热退时间、口腔疱疹及皮疹消退时间、可进食时间分别为4.1±1.3天、5.0±0.8天、4.0±0.6天,两组比较差异具有统计学意义(t值分别为-13.736、-13.983、-20.192,均P<0.01)。结论痰热清联合喜炎平及康复新液治疗普通型儿童手足口病临床效果明显,值得推广使用。
儿童;普通型;手足口病;痰热清注射液;喜炎平注射液;康复新液
[Abstract]Objective To observe the clinical effects of Tanreqing injection combined with Xiyanping injection and Kangfuxin solution in the treatment of children with common type of hand, foot and mouth disease (HFMD). Methods Sixty cases of children with HFMD selected from Beijing Children’s Hospital of Capital Medical University from January to December in 2012 were randomly divided into treatment group and control group. All those children met with the standards of this research. Children in both groups received comprehensive treatments, including reducing fever, fluid infusion, adopt antifebrile, rehydration, supporting treatment and enhancing healthcare. In addition, children in treatment group received a daily intravenous drip of Tanreqing injection and Xiyanping injection. Moreover, as for children in treatment group, they also received a sub-lingual administration of Kangfuxin solution. Besides, Kangfuxin solution was applied externally for rashes at the hand, feet and hip. However, children in control group received a combined treatment of daily intravenous drip of virazole and Aciclovir ointment for eternal use. Children in both groups went through a seven-day course of treatment. Children’s conditions, including reduction of body temperature and vanishing of oral herpes and rashes were observed. Results After a seven-day course of treatment, the total effective rate reached 100% in treatment group and 80.00% in the control group. The difference between two groups was of statistical significance (χ2=6.67,P<0.01). As for children in treatment group, their fever reduced in 2.0±0.8 days and their oral herpes and rashes vanished in 3.1±1.1 days. Besides, after 2.0±0.8 days of treatment, they were able to eat. However, as for children in control group, their fever reduced in 4.1±1.3 days and their oral herpes and rashes vanished in 5.0±0.8 days. In addition, they were able to eat after 4.0±0.6 days of treatment. The differences between two groups were of statistical significance (tvalue was -13.736, -13.983, -20.192, respectively, allP<0.01).Conclusion Clinical effects of Tanreqing injection combined with Xiyanping injection and Kangfuxin solution in the treatment of children with common type of HFMD are significant. Therefore, the combined therapy is worthy of being promoted and popularized.
[Key words]children; common type; hand, foot and mouth disease (HFMD); Tanreqing injection; Xiyanping injection; Kangfuxin solution
儿童手足口病(hand,foot and mouth disease,HFMD)是一种肠道病毒(柯萨奇16组,肠病毒71罕见)引起的急性传染病,在学龄前儿童的发展,尤其是在3岁以下年龄组发病率最高[1]。患者和隐性感染者均为传染源,主要通过消化道、呼吸道和密切接触等途径传播。主要症状为手、足、口腔等部位的斑丘疹、疱疹。少数重症病例可出现脑膜炎、脑炎、脑脊髓炎、肺水肿、循环障碍等,多由EV71感染引起,病情凶险,病死率高,致死原因主要为脑干脑炎及神经源性肺水肿,因此,早期、及时、有效的对症治疗尤为重要。本资料选取30例普通型手足口病住院患儿,采用痰热清、喜炎平、康复新液联合治疗的方法,取得显著疗效,现介绍如下:
1资料与方法
1.1一般资料
选取首都医科大学附属北京儿童医院2012年1月至2012年12月共60例符合普通型手足口病诊断标准的患儿,随机分为治疗组和对照组。治疗组:男孩18例,女孩12例,年龄1.5~6岁,平均4.5±0.6岁;对照组:男孩16例,女孩14例,年龄1.6~6.5岁,平均4.0±0.8岁。两组患儿在性别、年龄、病程、病情等方面差异均无统计学意义(均P>0.05),具有可比性。
1.2诊断标准
参考《手足口病诊疗指南(2013版)》标准,普通型病例:急性起病,发热,口腔粘膜出现散在疱疹,手、足和臀部出现斑丘疹、疱疹,疱疹周围可有炎性红晕,疱内液体较少;可伴有咳嗽、流涕、食欲不振等症状;部分病例仅表现为皮疹或疱疹性咽峡炎;多在1周内痊愈,预后良好;部分病例皮疹表现不典型,如:单一部位或仅表现为斑丘疹。
1.3纳入、排除标准
纳入标准:符合手足口病普通型病例的诊断标准;且年龄<7岁。排除标准:①排除手足口病危重病例(参考《手足口病诊疗指南(2012版)》[2]标准:患儿病情进展迅速,在发病1~5天左右出现脑膜炎、脑炎、脑脊髓炎、肺水肿、循环障碍等,极少数病例病情危重,可致死亡,存活病例可留有后遗症);②排除药疹、麻疹、水痘、风疹、荨麻疹、幼儿急疹等病例;③排除临床资料不全者。
1.4治疗方法
两组均采用退热、补液、支持和加强护理等综合治疗。对照组:每日1次给予病毒唑(注射用利巴韦林,0.1g/支)10~15mg/kg,加入到5%葡葡萄糖注射液100mL中静滴,连用5天,同时给予阿昔洛韦乳膏(10g/支)涂擦皮疹,每日4~6次,连用7天;治疗组:每日1次给予痰热清注射液(10mL/支)0.3~0.5mL/kg,加入到5%葡葡萄糖注射液100mL中静滴,连用5天,并给予每日1次喜炎平注射液(5mL/支)0.2~0.4mL/kg,加入到5%葡葡萄糖注射液100mL中静滴,连用5天,再给予康复新液(100mL/支)每日3~4次口腔含服,并外擦手、足、臀部皮疹,连用7天。
1.5观察指标
①两组患儿体温下降情况;②口腔疱疹、皮疹消退的情况及患儿可进食时间;③是否出现其他系统并发症。
1.6疗效评价
痊愈:体温恢复正常,口腔疱疹、皮疹消退,无新发疱疹及皮疹出现,未出现其他系统并发症;显效:2天内体温降至正常,口腔疱疹、皮疹明显减少并颜色变暗,可进食,未出现其他系统并发症;好转:3~4天内体温降至正常,一般状况好转,5~6天内不流涎,未出现其他系统并发症;无效:体温控制不满意,反复发热,口腔疱疹或皮疹消退不明显或退而复现,或出现其他系统并发症。总有效率=痊愈率+显效率+好转率。
1.7统计学方法
本组数据采用SPSS 17.0统计学软件进行统计处理,计量资料以均数±标准差表示,组间比较采用t检验,计数资料比较采用χ2检验,均以P<0.05为有显著性差异,P<0.01为有极显著性差异。
2结果
2.1两组临床疗效比较
治疗组治疗7天后总有效率为100.00%;对照组治疗7天后总有效率为80.00%。两组患儿治疗7天后总有效率比较具有极显著性差异(P<0.01)。见表1。
表1两组患儿治疗7天后临床疗效的观察和比较[n(%)]
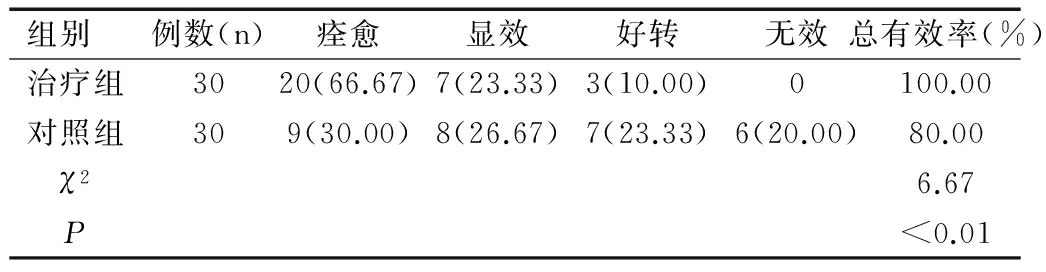
Table 1 Observation and comparison of clinacal effect between two gruops after 7-day treatment[n(%)]
2.2两组患儿热退时间、口腔疱疹及皮疹消退时间、可进食时间比较
两组患儿热退时间、口腔疱疹及皮疹消退时间、可进食时间比较均有极显著性差异(均P<0.01),见表2。


Table 2 Comparison of two gruops in feve educe,oral herpes and rashes vanishing and eating ±S)
2.3不良反应
两组患儿均未出现其他系统并发症及明显不良反应。
3讨论
3.1概述
手足口病是全球性的传染病,在我国发病率为113.88/10万~565.79/10万。该病在我国属于丙类传染病,占2010年第1批上榜的39种我国法定传染病报告病例死亡的前5位[2]。手足口病目前尚无特效药物治疗,因此,早期发现、及时有效的对症治疗成为治疗的主要手段。研究发现,多种中药治疗手足口病有非常好的疗效[3]。
3.2痰热清的药理作用
痰热清注射液是由熊胆粉、金银花、山羊角三味药再加上黄芩、连翘两味中药组合而成,现代中药理论实验证明熊胆能起到解毒、抑制病菌及解痉等疗效;金银花、连翘、黄芪、山羊角合用能起到抗菌解毒、缓解发热及免疫调节的作用。董崇林等[4]研究发现痰热清联合其他药物应用于治疗手足口病,能快速缓解患儿的发热症状,促进疱疹消退及溃疡愈合,减轻患儿痛苦,缩短病程。痰热清注射液改变了传统的中药口服的方式,通过静脉点滴的给药途径,显效更快,能更好的帮助患儿降低发热体温,消退皮疹及口腔疱疹,改善临床症状。
3.3喜炎平的药理作用
喜炎平注射液是一种新型纯中药制剂,主要成分是水溶性穿心莲内酯总酯的磺化物,其性苦寒,具有清热解毒、燥湿的功效。现代药理研究表明,喜炎平注射液具有明显抗病毒、解热、抗菌的作用。其抗病毒作用机制为:通过占据病毒复制时DNA与蛋白质的结合位,阻止蛋白质对DNA或RNA片段的包裹,阻断DNA或RNA的复制,从而抑制或杀灭病毒[5]。该药能抑制早期毛细血管通透性增高与炎性渗出与水肿,同时具有明显的促肾上腺皮质功能,提高白细胞、中性粒细胞及巨噬细胞对细菌、病毒的吞噬能力,增强机体的免疫力。
3.4康复新的药理作用
康复新液为美洲大蠊干燥虫体的乙醇提取物,主要功效为通利血脉,养阴生肌,可以显著促进肉芽组织的生长即血管的新生,同时可以加速坏死组织的脱落,进而可以快速地修复各类溃疡及创伤创面,另外,具有抗炎、消除炎性水肿的功能,通过提高巨噬细胞的吞噬能力及血清溶菌酶的活性,发挥调节机体生理平衡的作用[6]。除此之外,康复新液还具有抗过敏、抗感染、糖皮质激素样作用,而且还具有免疫调节的作用,诱导T淋巴细胞活化,促进γ-干扰素的合成与释放,进一步活化NK细胞,发挥抗病毒的作用。
本研究结果表明,采用痰热清联合喜炎平及康复新液治疗普通型儿童手足口病有较好的临床疗效,缩短了病程,减轻了患儿及家长的痛苦,同时减少了继发感染的机会,值得推广使用。
[1]Fan X L, Jiang J, Liu Y J,etal. Detection of human enterovirus 71 and Coxsackievirus A16 in an outbreak of hand, foot, and mouth disease in Henan Province, China in 2009[J].Virus Genes,2013,46(1):1-9.
[2]中华人民共和国卫生部.手足口病诊疗指南(2012版)[M].北京:中华人民共和国卫生部,2012.
[3]Cao H, Liu Z, Steinmann P,etal. Chinese herbal medicines for treatment of hand, foot and mouth disease: a systematic review of randomized clinical trials[J]. European Journal of Integrative Medicine,2012,4(1):e85-e111.
[4]董崇林,孙铭晓,连成成.痰热清注射液联合利巴韦林治疗手足口病160例疗效观察[J].中国综合临床,2011,27(4):442-443.
[5]唐娟.喜炎平联合利巴韦林治疗手足口病162例疗效观察[J].中国医药指南,2013,11(2):23-24.
[6]王章洪,任文东,唐燕.康复新液治疗手足口病208例临床观察[J].中外医学研究,2012,10(10):63-64.
[专业责任编辑:潘凯丽]
Clinical research on combined therapy of TCM preparations in the treatment of children with hand-foot-and-mouth disease
ZHU Yan-hui, SONG Hong-ling
(Emergency Department’Beijing Children’s Hospital, Capital Medical University, Beijing 100045, China)
2015-09-11
朱艳辉(1977-),女,主治医师,主要从事儿童急救工作。
宋宏玲,副主任医师。
10.3969/j.issn.1673-5293.2016.02.020
R
A
1673-5293(2016)02-0205-02
猜你喜欢
现代仪器与医疗(2021年4期)2021-11-05
煤气与热力(2021年5期)2021-07-22
透析与人工器官(2020年1期)2020-11-16
中成药(2018年3期)2018-05-07
中成药(2017年3期)2017-05-17
中国卫生标准管理(2015年18期)2016-01-20
转化医学电子杂志(2015年4期)2015-12-27
中国卫生标准管理(2015年14期)2015-01-27
中国药业(2014年12期)2014-06-06
中国药业(2014年24期)2014-05-26
