
The effect of acupuncture plus drug versus drug alone on patients with mild cognitive impairment:a systematic review
2016-09-14 07:57TingShuaiHuiZhangLiJuanYiXuTianZiZengYanWangGuoMinSong
Traditional Medicine Research 2016年1期
Ting Shuai,Hui Zhang,Li-Juan Yi,Xu Tian,Zi Zeng,Yan Wang,Guo-Min Song
1Graduate College,Tianjin University of Traditional Chinese Medicine,Tianjin 300193,China.2School of Nursing,Tianjin University traditional Chinese Medicine,Tianjin,China.3Nursing Department of Tianjin Hospital,Tianjin 400020,China.
Introduction
Mild cognitive impairment(MCI)is a transitional period between normal aging and early Alzheimer’s Disease(AD)[1].It has been referred to as subjective and objective cognitive complaint for age,in which these persons has memory loss and the extent is greater than that of normal aging.However,they don’t have dementia.If these persons are observed for a long time,it can be found that they are very likely to progress to AD[2,3].It is reported that the patient with MCI will have a 10-fold increased risk of progressing to AD as compared to cognitively normal individuals[4].In the United States,AD is the sixth leading cause of mortality and the fifth leading cause for people aged ≥65 years[5].Therefore,it is essential to delay progression of MCI to AD by effective treatment.However,currently,drugs for MCI are mostly acetylcholine-esterase inhibitors,such as Rivastigmine and Donepezil.They cannot have well-established effectiveness in delaying the progression of MCI to AD.The available treatments cannot be obtained to stop or reverse the progression from MCIto AD,neither[6,7].On the contrary,acupuncture that nourishes kidney and the marrow(in PC6,GV20,GB20,etc)can be effective for improving intelligence,stimulating awareness and strengthening memory.
Acupuncture is also considered to be relatively non-toxic[8,9].In China,acupuncture technology was invented 3000 years ago and has been in practice since then.Acupuncture can treat a wide variety of cases containing cardiovascular and psychiatric diseases,pain.Nowadays,it is also increasingly used as an adjunct therapy with drugs in western countries[10].
Recently,after plenty of related literature about the treatment for MCI reviewed,we found there were two systematic reviews and their pooled outcome elucidated acupuncture was effective for MCI[11,12].In addition,there were two published studies showing that acupuncture plus drug was more effective than acupuncture alone by statistical analysis[13,14].Consequently,although the drug don’t have obvious effectiveness,it is important to advocate that drug should not be put aside by patients and their clinicians but rather an integrative approach should be adopted to offer both the relief of symptoms and delay of the progression as much as possible.
In terms of published studies about exploring the effect of acupuncture plus drugs to manage patients with MCI,they have suggested that acupuncture plus drug could significantly improve the delay of the progression of MCI to AD.Nevertheless,published studies conducted involved small sample sizes. Moreover, some of studies had poor methodological quality and then they may overestimate the positive effect.Finally,there is no systematic review to evaluate the effect of acupuncture plus drug.Therefore,in terms of these reasons above,we conducted a systematic review to evaluate the effect of acupuncture plus drug for MCI.
Methods
A computerized search of the databases[Pubmed,EMbase,Web of Science,the Cochrane Library,China National Knowledge Infrastructure(CNKI),China Biology Medicine disc(CBM disc),Wanfang,and Chinese Scientific Journals(VIP)]was performed from inception through February 2015,with full text available and language limited to English or Chinese.Given that only a few related articles about acupuncture for MCI were published every year,medical subject heading(MeSH)and full-text words were combined to search according to Boolean logic operator.The following terms: acupuncture therapy [Mesh](‘acupunctur*’, ‘electro acupuncture’, ‘Ching Lo’, ‘Jing Luo’,‘meridians’, ‘moxabustion’, ‘moxibustion’, ‘acupoint’)and mild cognitive impairment[Mesh](‘mild cognitive impairment’,‘mild cognitive decline’, ‘mild cognitive disorder’)were selected.The lists of references of included original articles and reviews were also manually searched to search for more relevant studies.
Inclusion criteria
We determined the inclusion criteria of published studies according to the criteria of PICOS:P (Population) I(Intervention),C(Comparison),O(Outcomes),S(Study design)[15].And it was defined as:a)population:all the patients which were diagnosed with mild cognitive impairment in terms of specific diagnostic criteria;b)intervention:acupuncture and drug were combined to treat MCI.The form of acupuncture was not limited and electro acupuncture,body acupuncture or scalp acupuncture could be acceptable;c)comparisons:drug alone.The drug therapy must be the same with the intervention group;d)outcomes:mental state and ability of activities(Mini-Mental State Examination scores and Activities of Daily Living scores(ADL)were evaluation tool for mental state and ability of activities in this study);e)study design:published RCTs with appropriate random sequence generation could be included.Additional inclusion criteria:studies must be published in English or Chinese.
Exclusion criteria
The repeated published studies in different time or research department and duplicates were excluded.
Data Extraction
Data extraction was respectively conducted by two investigators(T,S and H,Z).Based on the Standards for Reporting Interventions in Clinical Trials of Acupuncture(STRICTA)guidelines[16],we extracted the materials of the each trial including author,publication year,the number of participants,age of included patients,diagnostic criteria,random method,interventions,comparisons,the duration of treatments and outcome measures.The complete binary and continuous data reported on specific outcomes were needed.If necessary,we would contact the corresponding authors to obtain relevant data.Any divergences in screening,extracting data and assessment of the quality of methodology were resolved through consulting with the third investigator(G.M.,Song).
Quality assessment of the included studies
Quality assessment of trials included in this study was respectively performed by two investigators(T,S and L.J,Yi)according to the Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 [17].These procedures were performed by the seven aspects as follows:randomization sequence generation,allocation concealment,blinding of participants and study personnel,blinding of outcome assessors,incomplete outcome data,selective reporting and other biases.After the materials from eligible trials reviewed,each domain of the seven aspects was rated as “high risk”, “unclear risk”or“low risk”.These domains would be classified as low risk if appropriate methods were used and reported in detail;if not,corresponding domains would be rated as high risk instead.On the other hand,associated domains were rated as unclear risk if the materials reported in the included studies were not sufficient to judge the risk of bias.
Data analysis
All extracted data for the scores of MMSE and ADL were entered into Review manager 5.3(Copen-hagen:The Nordic Cochrane centre,The Cochrane Collaboration,2013)to perform statistical analysis.For continuous outcomes,we selected mean difference(MD)with 95%confidence interval(CI)to estimate the pooled effect size.Because of the different baseline data,we chose the changed data to calculate the pooled results in accordance with the baseline and end-point data.(S2effect size=S2baseline+S2end-point-2*R*Sbaseline*Send-point;
Meffect size=|Mbaseline-Mend-point|;R:0.4 or 0.5)[18].Heterogeneity for the whole extracted data was evaluated by Chi2,corresponding P value and I2index.When clinical heterogeneity was absent and statistical heterogeneity(I2greater than 60%)existed,a random effects model was used and sensitivity analysis was carried out to detect the robustness of the result by sequentially omitting each study.When they were similar enough to be able to pool the effect size among studies,we planned to use fixed-effect model for low to moderate levels of heterogeneity (I2index from 0% to 60%).When heterogeneity was larger than 75%,we gave up to pool studies and only conducted descriptive analysis[19].The funnel plot was performed to determine whether publication bias occurred when more than 10 studies were included.
Results
Study selection and trial characteristics
A total of 399 trials were included in the initial literature search.Then 18 trials which included 1095 participants were selected in accordance with inclusion and exclusion criteria satisfying qualitative analysis.The flow diagram of citation retrieval and selection was presented in Figure 1.The basic characteristics of 18 trials(14 trials met quantitative analysis)were summarized in Table 1 and Table2.

Figure1:Flow diagram of literature retrieval and screening.

Table1:The main characteristics of included studies.
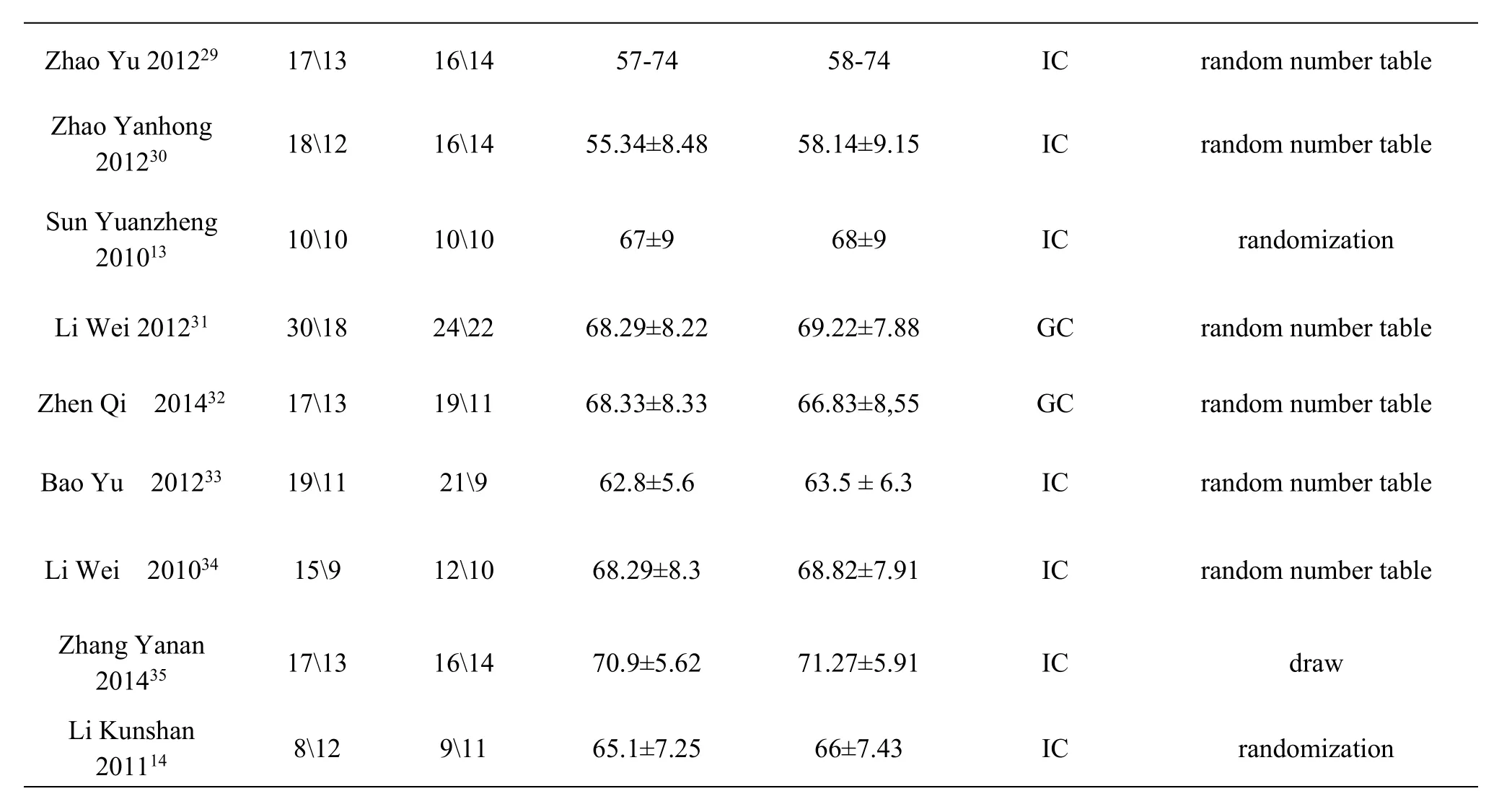
Note:T:treatment group;C:control group.GC:Chinese diagnostic criteria;IC:International diagnostic criteria

Table2 The main intervention of included studies.

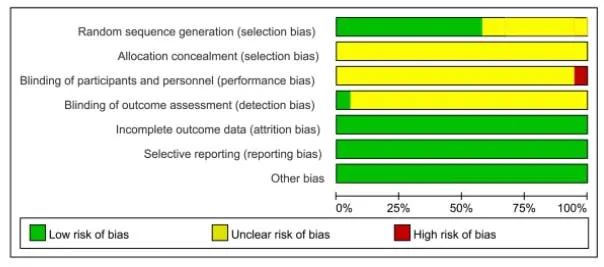
Figure2Assessment of Risk of Bias.
Methodological quality
We used the Cochrane Risk of Bias Tool to assess the risk of bias[17].The results of risk of bias assessment for every study were revealed in Figure 2.
A total of 18 trials involving 1095 participants were included.a)All of the included studies reported the usage of the randomized method,but only 11 of the included trials described the method used to generate the allocation sequence by random number table or draw in detail[20,22,23,26,29-35].b)The whole included studies didn’t mention the method used to conceal the allocation sequence.c)Acupuncture treatment could not be double-blinded in randomized studies,so blinding of participants and personnel couldn’t be performed.Among the included studies,only one trial described the blinding of outcome assessment and the other trials didn’t mention it[20].d)There were 4 trials reporting drop-out and offering the brief reasons and the drop-out rate was lower than 10%[22,26,34].Therefore,the 4 trials were rated as low risk of bias for the domain of incomplete outcome data.
Meta-analysison MMSE
Twelve of all trials involving 704 participants reported the scores of MMSE[13,14,21,22,27,29-35].Heterogeneity was identified across the included studies(P=0.0004,I2=67%).A random-effects model was chosen to summarize mean effect size,because the sources causing heterogeneity were not detected among included trials.This model indicated that the whole participants from included trials were sampled from the different population.Pooled result suggested that acupuncture plus drug could effectively improve the scores of MMSE with statistical significant difference(MD=1.73;95%CI=1.28,2.18;P<0.001)(Figure 3).
Sensitivity analysis on MMSE
Leave-one-out sensitivity analysis was adopted to test the robustness of pooled result on the scores of MMSE.Pooled result of leave-one-out sensitivity analysis was the same and the sensitivity analysis suggested that the summary effect size was robust(Figure4).
Publication biason MMSE

Figure3 Meta-analysis on MMSE.

Figure4 Sensitivity Analysis on MMSE.
We performed a funnel plot of publication bias on MMSE to examine the publication bias,be cause there were twelve of all trials reporting the scores of MMSE.The outcome from the funnel plot analysis was summarized in Figure 5.The funnel plot showed symmetry,which indicated that no publication bias possibly existed in the included trials.

Figure5 Funnel Plot on MMSE.
Meta-analysis on ADL
6 trials which included 404 participants were included in the meta-analysis to calculate the scores of ADL[21,22,31-34].We identified homogeneity in the six studies(P=0.84,I2=0%).Therefore,a fixed-effect model of analysis was performed to calculate mean effect size.This model suggested that all the participants from included trials were sampled from the same population.Pooled result indicated that the scores of ADL could be improved by acupuncture plus drug interventions with statistical difference(MD=5.63;95%CI=4.40,6.87;P<0.001,Figure 6).
Adverse effect
There were 4 studies[25,26,30,33]which reported the adverse effect.Acupuncture-associated bleeding was reported in 3 studies[25,30,33],but they didn’t have impact on the treatment for MCI.In a study[26],diarrhea both occurred in the treatment group and control group.
Discussion
The mechanism of acupuncture

Figure6 Meta-analysis on ADL.
Acupuncture,a treatment of traditional Chinese medicine(TCM),remains promising as an adjunct therapy to treat neurological diseases such as stroke and MCI[36].With the increasing usage of acupuncture all over the world,the underlying mechanisms are explored by more researchers in recent years.Based on existing studies,it can be speculated that acupuncture may have a great effect on patients with MCI through the mechanism of modulating special brain network or brain regional activity[37].Hence,acupuncture plus drug should be considered in order to delay the progression of MCI to AD better.
The evidence of meta-analysis
The systematic review and meta-analysis were implemented in order to systematically evaluate the effect of acupuncture plus pharmacological therapy versus pharmacological therapy alone for the patients with MCI.The results of this study suggested that acupuncture plus pharmacological therapy for MCI could significantly improve the scores of MMSE and the scores of ADL.The sensitivity analysis on the no publication bias.
Limitations and suggestions
The meta-analysis has some potential limitations and for these limitations,we come up with several suggestions in order to further improve the quality of study.They are displayed in the following aspects:
a)Not all the included studies described the randomized method in detail even though they all reported the baseline materials were no statistical significance;Consequently,it should be suggested that study report it in detail in order to ensure the reliability of outcome.
b)The whole included studies didn’t mention the method of concealing the allocation sequence.It should be suggested study must use the method of concealing the allocation sequence to guarantee the implementation of random process and report the process in detail in the study.
c)Most types of placebo acupuncture cannot be blinded for the acupuncturists and patients[38],so double-blinding has been difficult.But outcome assessment can be blinded and the outcome measures can be objective to prevent measure bias.For this systematic review,only one trial[20]mentioned the blinding of outcome assessment.In addition,the outcome measures were almost subjective questionnaire.Therefore,it may result in measurement bias and assessment bias.The proposal should be offered that study use objective outcome measures such as the change of P300,and the blinding of out come assessment must be implemented.
d)Among all the included trials,the work experience of acupuncturists was seldom mentioned and it was unclear whether acupuncturists were trained be fore study according to the unified standard.It may result in performance bias.So it is suggested that acupuncturists should be trained in the light of the unified standard to ensure their skill are nearly equal.
e)It was searched only by English and Chinese database and language was limited with English and Chinese.
Conclusion
With present evidences,acupuncture plus drug is more effective than drug alone for the treatment of MCI.Acupuncture can be an adjunct therapy with drugs for patients with MCI.However,this meta-analysis and the relevant studies have some limitations,such as poor trial methodology. Consequently,further randomized controlled trials with larger number and rigorous methodology and longer follow-up period are required to improve the evidence of results.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
1.Petersen.Mild cognitive impairment as a diagnostic entity.Journal of internal medicine 2004;256:183-94.
2.Petersen,Doody,Kurz,et al.Current concepts in mild cognitive impairment. Archives of neurology 2001;58:1985-92.
3.Albert,DeKosky,Dickson,et al.The diagnosis of mild cognitive impairment due to Alzheimer's disease:recommendations from the National Institute on Aging-Alzheimer's Association work groups on diagnostic guidelines for Alzheimer's disease.Alzheimer's &dementia:the journal of the Alzheimer's Association 2011;7:270-9.
4.Petersen.Clinical practice.Mild cognitive impairment.The New England journal of medicine 2011;364:2227-34.
5.National Center for Health Statistics.[Accessed on March 23,2013.]National Vital Statistics System.Multiple cause-of-death files.Available from:http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm.
6.Cooper,Li,Lyketsos,et al.Treatment for mild cognitive impairment:systematic review.The British journal of psychiatry:the journal of mental science 2013;203:255-64.
7.Zeng,Salvage, Jenner.Effect and mechanism of acupuncture on Alzheimer's disease.International review of neurobiology 2013;111:181-95.
8.Han,Yin,Zhou,et al.Investigation on the changes of dependent signal on the amplitude of low frequency fluctuations at blood oxygen level in brain after acupuncture Neiguan(PC 6).Zhongguo zhen jiu=Chinese acupuncture&moxibustion 2009;29:647-51.
9.Zhu XT.Influences of acupuncture with effects of awakening consciousness and improving intelligence in group acupoints on brain resting state function.J Beijing Univ Tradit Chin Med 2011;34:181-5.
10.Barnes,Bloom,Nahin.Complementary and alternative medicine use among adults and children:United States,2007.National health statistics reports 2008:1-23.
11.Cao,Wang,Chang,et al.Acupuncture for vascular mild cognitive impairment:a systematic review of randomised controlled trials.Acupuncture in medicine:journal of the British Medical Acupuncture Society 2013;31:368-74.
12.Zhou,Zhang,Cao,et al.Treating vascular mild cognitive impairment by acupuncture:a systematic review of randomized controlled trials.Zhongguo Zhong xi yi jie he za zhi Zhongguo Zhongxiyi jiehe zazhi=Chinese journal of integrated traditional and Western medicine/Zhongguo Zhong xi yi jie he xue hui,Zhongguo Zhong yi yan jiu yuan zhu ban 2013;33:1626-30.
13.Sun,Li.Clinical observation on the treatment of mild cognitive impairment by combined acupuncture and medication(in Chinese).Shanghai Journal of acupuncture and moxibustion 2010;29:759-61.
14.Li,Sun.Clinical observation on the treatment of mild cognitive impairment by combined acupuncture and medication(in Chinese). [dissertation]. Heilongjiang:Heilongjiang University of Traditional Chinese medicine 2011.
15.Stone.Popping the(PICO)question in research and evidence-based practice.Applied nursing research:ANR 2002;15:197-8.
16.MacPherson,Altman,Hammerschlag,et al.Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA):extending the CONSORT statement.Acupuncture in medicine:journal of the British Medical Acupuncture Society 2010;28:83-93.
17.Higgins,Green.Cochrane handbook for systematic reviews of interventions version 5.0.0. 2008;London:The Cochrane Collaboration.
18.Brok,Thorlund,Gluud.Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J Clin Epidemiol 2008;61:763-9.
19.Higgins,Deeks.Chapter 7:Selecting studies and collecting data.Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0.The Cochrane Collaboration.2011.
20.Hu,Wang,Liang."Activiting brain and regaining consciousness"acupuncture treats the elder with mild cognitive impairment:70 cases(in Chinese).World Health Digest 2014:279.
21.Zhao,Lu,Jia,et al.The effect of Bushen Yisuiacupuncture plus draganon on the patients with mild cognitive impairment after stroke(in Chinese).Shanxi Journal of Traditional Chinese Medicine 2013;34:1385-6.
22.Li, Yu, Cao, et al. Clinical observation of electroacupuncture with aricept on preventing participants with MCI progressing to AD(in Chinese).Laser Journal 2013;34:75-6.
23.Jiao,Shi,Xu,et al.Clinical observation on the treatment of mild cognitive impairment by combined scalp acupuncture and medication(in Chinese). Journal of Clinical Acupuncture and Moxibustion 2011;27:23-4.
24.Lin,Yin,Shi.The treatment for mild cognitive impairment by combined scalp acupuncture and medication(in Chinese).National medical frontiers of China 2013;8:76.
25.Luo,Zhen,Li,et al.Efficacy of combined treatment of drugs and electric acupunture on cognitive function of patients with mild cognitive impairment(in Chinese).China medical herald 2013;10:118-22.
26.Sun,Zhu,Zhang.The treatment of mild cognitive impairment by Yuan-primary and Luo-connecting needling method plus aricept:30 cases(in Chinese).Chinese Journal of Traditional Medical Science and Technology 2007;14:180.
27.Sun, Sun, Zhang. Effect of Yuan-primary and Luo-connecting needling method plus medication on P300 in patients with mild cognitive disorder(in Chinese).Shanghai JAcu-mox 2012;31:12-4.
28.Wang,Liang,Huang,et al.Study of magnetic resonance spectroscopy on the treatment of mild cognitive impairment after stroke by acupuncture(in Chinese).Journal of Emergency in Traditional Chinese Medicine 2014;23:1928-30.
29.Zhao,Liu,Liu.Clinical observation of the treatment of mild cognitive impairment by combined acupuncture and nimodipine(in Chinese).Journal of Military Surgeon in Southwest China 2012;14:36-8.
30.Zhao.Clinical observation of the treatment of mild cognitive impairment by combined acupuncture and nimodipine(in Chinese).Clinical Rational Drug Use 2012;5:16-7.
31.Li,Cheng,Yu.Observation on therapeutic effect of acupuncture combined with medicine on mild cognitive disorders in patients with post-stroke(in Chinese).Chinese acupuncture and moxibustion 2012;32:3-7.
32.Zhen.Clinical study on treatment on mild cognitive impairment after stroke by Yishen Tiaodu acupuncture(in Chinese). [dissertation]. Heilongjiang: Heilongjiang University of Traditional Chinese medicine 2014.
33.Bao.Clinical study on mild cognitive impairment after stroke treated with cord-supplement and brain-strengthening acupuncture(in Chinese).[dissertation].Heilongjiang:Heilongjiang University of Traditional Chinese medicine 2012.
34.Li.Clinical observation of the effect of acupuncture on mild cognitive impairment after stroke(in Chinese).[dissertation].Beijing:Beijing University of Chinese medicine 2010.
35.Zhang.Observation of mild cognitive dysfunction after stroke's treatment by the combinition with acupuncture andmedicine(in Chinese).[dissertation].Nanjing:Nanjing University of Chinese medicine 2014.
36.Li,Yang.An fMRI study of acupuncture-induced brain activation of aphasia stroke patients.Complement Ther Med 2011;19:49-59.
37.Wang,Nie,Li,et al.Effect of acupuncture in mild cognitive impairemnt and Alzheimer Disease:a functional MRI study.PLoSOne 2012;7.
38.Lene V,Baram S,Takakura N,et al.Can acupuncture treatment ba double-blinded? An evaluation of double-blinded acupuncture treatment postoperative pain.PLoSOne 2015;10.
 Traditional Medicine Research2016年1期
Traditional Medicine Research2016年1期
- Traditional Medicine Research的其它文章
- TMR:A new star for the research of traditional medicine
- Effects and safety of acupuncture for DFUs:a systematic review and meta-analysis
- Massage for migraine:A meta-analysis
- Similarities and differences of doctor-patient co-operated evidence-based medical record of treating digestive system diseases with integrative medicine compared with traditional medical records
- Complete response of hepatocellular carcinoma treated with traditional herbal medicine:A case report