
Effects and safety of acupuncture for DFUs:a systematic review and meta-analysis
2016-09-14 07:57LiJuanYiXuTianTingShuaiZiZengLiMaGuoMinSong
Traditional Medicine Research 2016年1期
Li-Juan Yi,Xu Tian,Ting Shuai,Zi Zeng,Li Ma,Guo-Min Song
1Master degree candidate,Graduate College,Tianjin University of Traditional Chinese Medicine,Tianjin 300193,China.2Director of Nursing,Nursing Department of Tianjin Hospital,Tianjin 400020,China.
Introduction
People with diabetes mellitus(DM)often suffer from the intractable diabetic foot ulcers(DFUs)secondary to neuropathy,peripheral vascular disease with ischaemia or both[1].DFUs is the leading contributor to the diabetes-related hospitalization and non-traumatic lower extremity amputation in patients with DM[2,3].It was estimated that 25%of patients with DM would progress foot ulcer throughout their lives[4],and up to 15%would suffer from amputation[5].Therapeutic regimens on DFUs include glycemic control,extensive local wound care and prompt revascularization[6],however,poor healing rate is still a fatal cause leading to low quality of life and overwhelming medical expenditures[7].
Acupuncture,one of the complementary and alternative medicines refers to insert the needless,specific medicinal herb or both(e.g.Moxa,Ginger,Garlic,etc.)into the specific acupoints on body for facilitating recovery,was commonly used to treat the DFUs[8-9].Nowadays a majority of trials evaluated the summary effects of various traditional Chinese medicine TCM interventions,however,these results from different studies are still inconclusive,Although some systematic reviews and meta analyses into the topic published,some weakness can not be avoided and a great deal of randomized controlled trials(RCTs)has failed to complete since then.Therefore,a systematic review and Meta analysis was undertaken by us to critically evaluate the evidence from RCTs regarding acupuncture in DFUs.
Methods
The report of the systematic review and meta analysis is in accordance with the Preferred Items for Systematic Review and Meta Analysis(PRISMA)and Cochrane Handbook for Systematic Reviews of Interventions[10-11].Ethical approval was not necessary,because this study was conducted based on the completed previous trials.
Inclusion and exclusion criteria
RCTs regarding effect and safety of acupuncture for the treatment of DFUs were eligible for the inclusion criteria.Only articles in English and Chinese language were eligible.
Typesof participants
Patients who were definitely diagnosed as DFUs were met the inclusion criteria.Wagner grade of DFUs was not restricted in our meta analysis.However,study involving patients with concurrence of DM and other diseases,such as last-stage of cancer or use the steroid hormonetherapy,would be excluded.
Types of interventions
The experimental group involved patients undergoing acupuncture,a combination of acupuncture and other therapies.The control group involved patients undergoing placebo,drug therapy and no-treatment.
Types of out come measures
Major outcome parameters:total curative effective rate,time to ulcer healing,the hemodynamic parameter,and adverse events.
Exclusion criteria
We excluded these studies that were not RCTs design and the RCTs which tested comprehensive effect of acupuncture plus other interventions.It was ineligible for the study if the data was in-sufficient,lacking or unable to translate into effective sort.
Search strategy
We searched six electronic databases,including PubMed,Web of Science,EMbase,Cochrane library,CBM,and CNKI(from inception to 30 October,2014).The following search terms were used: ‘acupuncture therapy’, ‘acupuncture*,needling’,‘acupoint*’,‘electro acupuncture’,‘moxibustion’,‘diabetic foot’,‘diabetic feet’, ‘DFUs’, ‘diabetic gangrene’, ‘diabetic foot gangrene’.The reference lists of included articles were manually searched to include any eligible studies.
Data extraction and quality assessment
Searches were conducted and data extracted by two independent reviewers(YLJ and TX).Each trial identified in the search was evaluated for design,patient eligibility criteria,and outcome measures.Divergences were resolved by discussion with a third review reviewer(SGM).Duplicate records were excluded based on screening of titles and abstracts.All remaining articles were screened in full text.Quality assessment of included trials was independently performed by each reviewer according to Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0[12].
Statistical analysis
The total curative efficacy,mean time to ulcer healing and the hemodynamic parameters was calculated.We evaluated homogeneity trials included in I2statistic.If I2>50%,the trials were considered to be heterogeneity,a random effects model was conducted.If I2<50%,the studies were deemed to be homogeneity,a fixed effects model was performed.Pooled statistics of the differences in the ratio or mean for the individual study are shown.Pooled differences in ratio or means were calculated and a two-sided P value<0.05 was considered to indicate statistical significance.Subgroup analysis will be performed according to courses of treatment and different comparisons.All analyses were performed using Review Manager (RevMan) 5.3.0 (the Cochrane Collaboration,Copenhagen,Denmark)and Stata software,version 12.0(Stata Corp,College Station,TX).
Results
A total of 336 citations were identified at the initial literature search stage and added no trial to the searched result.After screened title,abstract and full-text,only 8 trials(included 9 RCTs)[8,9,13-18]that included 481 participants according to inclusion and exclusion criteria met quantitative analysis.Among these included articles,Zhang(2008)[8]conducted a three-arm trial,and we divided it into two RCTs.The flow diagram of literature retrieval and study selection was presented(Fig.1).
Characteristics of included trials
A total of 481 participants were included.The Characteristics of 8 trials(included 9 RCTs)were presented in Table1.
Assessment of risk of bias
All included studies described random sequence generation,but only two studies provided adequate information to generate the random sequence.So two studies were judged to be at low risk of bias for this domain.Remaining studies were unclear for risk of bias.
Allocation concealment
No trials mentioned how the randomization sequence were implemented,so they were judged as being at unclear for risk of bias.
Blinding
Blinding for researcher was impossible,but they will appear the operation bias and thus the domain was regarded as “high risk”.One trial was designed to blind the outcomes of assessor.Another study reported the blinding for participants,but details cannot be extracted from studies,the domain of which was rated as “unclear”.Remained studies did not state whether blinding was employed,which led to an unclear for risk of detection bias.
In complete data
For all trials,authors stated that no drop-out,withdrawal and loss to follow-up existed during the research process.Therefore,they were deemed to be at low risk of attrition bias for this domain.
Selective Report
All studies reported outcomes adequately and were deemed to be at low risk of bias.Whereas,conclusion was identified according to methods and participants section of eligible studies due to protocol cannot be provided.
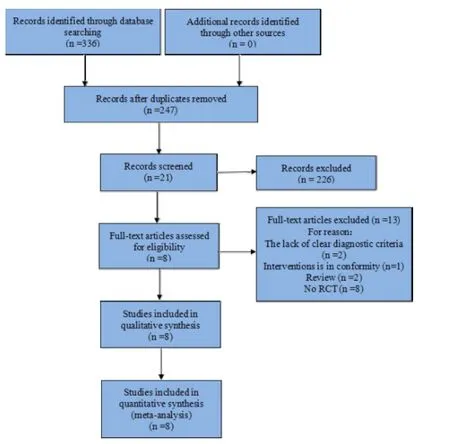
Figure1 PRISMA flow diagram of reteriveal and selection of literature.
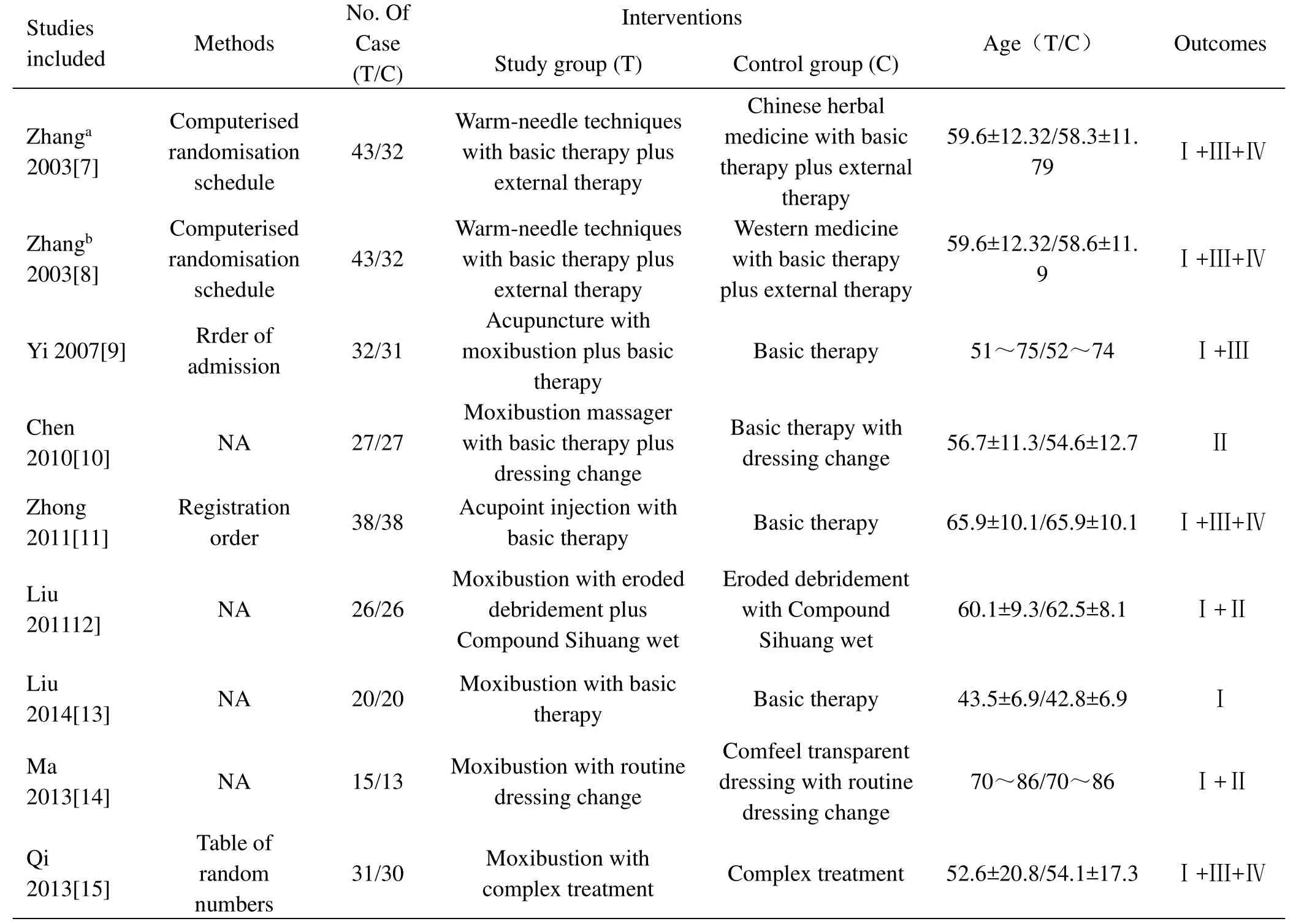
Table1 Characteristics of 9 trials identified in the literature search.
Other potential source of bias
Three studies were funded by non-commercial organizations and the remaining trials did not report funding information.The methodological quality assessment of included trials was revealed(Fig.2 and Fig.3).
Meta-analysis
A total of 8 trials(9 RCTs)investigated the effects of acupuncture and reported the total effective rate of the acupuncture group compared with the control group for the treatment of DFUs.Sub-group analysis was conducted due to the different treatment courses.For courses of less than 6 weeks group,five studies(5 RCTs)were involved with clinical and statistical heterogeneity in the overall treatment time(P=0.12,I2=46%),and thus a fixed effects model of analysis was used.Pooled result revealed the difference between the intervention and the control groups(RR=1.37,95%CI was 1.21 to 1.55.P<0.000)(Fig.4).For courses of 8 weeks group,one study was involved and the result showed that acupuncture effectively improved the total effective rates(RR=1.20,95%CI was 1.00 to 1.44.P=0.05)(Fig.4).In courses of 12 weeks group,two studies were pooled without heterogeneity(P=0.45,I2=0.0%).The meta analysis revealed the intervention groups were significantly better than the control groups(RR=1.29,95%CI was 1.09 to 1.53,P=0.004)(Fig.4).
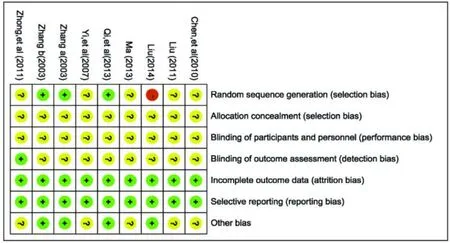
Figure2 Risk of bias summary:authors' judgments about each risk of biasitem for included studies.
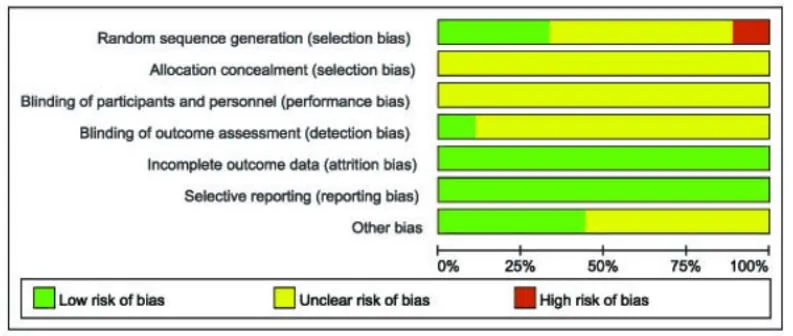
Figure3 Risk of bias graph:authors' judgments about each risk of bias item for included studies.
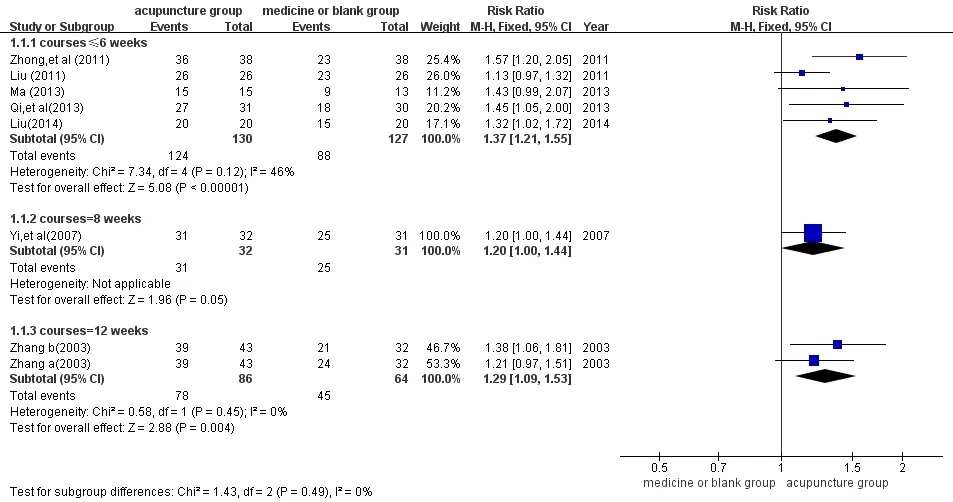
Figure 4 Meta-analysis for total effective rate.
Time to ulcer healing
Three studies employed ulcer healing time as outcomes and were divided into sub-groups according to the diversity of control types.For acupuncture versus blank group,two studies(2 RCTs)were included.A random-effects model of analysis was adopted,as statistical heterogeneity had been detected(P=0.04,I2= 75%).The pooled result suggested that the acupuncture shortened the healing time(SMD=-1.31,95%CI was-2.57 to-0.05.P=0.04).After the pooled analysis,we found the participants’average ages of Chen,et al(2010)were older than the Liu(2011)’s.Therefore,the age’s difference of participants between two trails led to significant clinical heterogeneity existed in these two trials.Moreover,basic interventions were different between them,Liu(2011)did more specialized and meticulous nursing.Hence,methodological heterogeneity existed in the 2 trials and the research team performed a descriptive analysis to interpret the results above:Chen,et al(2010)reported that the observation group could obviously shorten the healing time of diabetic foot ulcers(SMD=-0.72,95%CI was-1.42 to-0.02)and Liu(2011)had the same conclusion(SMD=-2.02,95%CI was-3.07 to-0.96,Fig.4).In acupuncture versus medicine group,only one study was involved.The result indicated differences between the two groups statistically.In the aspect of minimizing the wound healing time,acupuncture group was obviously superior to the control group(SMD=-5.00,95%CI was-7.33 to-2.68,P<0.001,Fig.5).
The hemodynamic parameters
A total of 4 trials(5 RCTs)reported the variation of the relative hemodynamic parameters which were measured by color to Dopple before and after intervention.According to the different hemodynamic parameters,sub-group analysis was generated.With vessel diameter(VD),3 trials(4 RCTs)were involved with clinical and statistical heterogeneity(P<0.001,I2=74%).A sub-analysis was conducted to explore whether the heterogeneity could be partially explained by the different control types.For acupuncture versus blank group,two studies(2 RCTs)were involved.Three studies were pooled without obvious heterogeneity(P=0.88,I2=0.0%).The result revealed a difference between acupuncture group and the control group(SMD=1.01,95%CI was 0.66 to 1.37,P<0.001).For acupuncture versus medicine group,only one study(2 RCTs)was involved.Two RCTs were pooled without heterogeneity(P= 0.85,I2= 0.0%).The result indicated that no better improvements were observed after acupuncture treatment(SMD=0.18,95%CI was-0.14 to 0.51,P=0.27,Fig.6).
Two studies(3RCTs)reported the measure of peak velocity and no heterogeneity was detected across studies(P=0.97,I2=0.0%).The pooled result indicated no difference between acupuncture group and the control group(SMD=0.20,95%CI was-0.07 to 0.48,P=0.14,Fig 7).A total of two trials(3 RCTs)which change data into blood flow volume two groups statistically.In the aspect of minimizing were presented and were incorporated without heterogeneity(P=0.14,I2=48%).The meta analysis showed the acupuncture group was significantly superior to the control group(SMD=0.33,95%CI was 0.07 to 0.60,P=0.01,Fig 8).
Adverse events
Three of the 8 studies evaluated the safety of interventions.Zhang(2003)reported 7%of patients were burnable and bullate after acupuncture.Zhong et al(2011)stated a low incidence of injection site pain(some 5.26%).Qi et al(2013)reflected no occurrence of adverse events after acupuncture.None of the participants withdrew or dropped out due to adverse events.
Publication Bias
The research team performed the analyses of all studies which were involved in the measure of total effective rate,using Begg’s and Egger’s plot to determine publication bias in all the literature.The P value from the Begg and Egger was 0.063 and 0.005,respectively,and the asymmetry of Egger’s plot indicated that publication bias possibly exists(Fig.9).
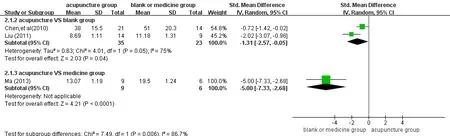
Figure5 Meta-analysis for the ulcer healing time.
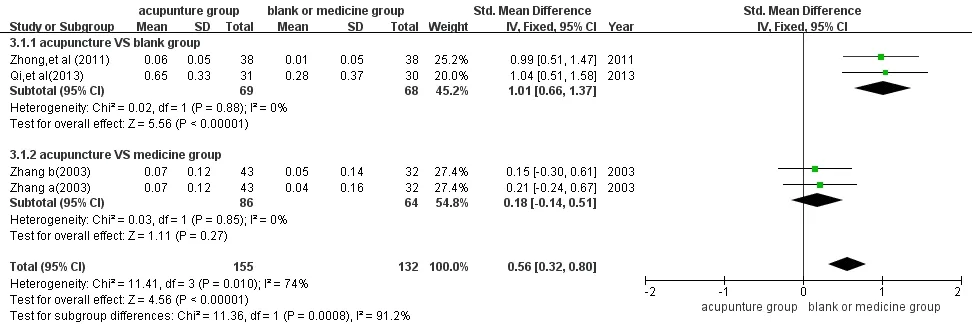
Figure6 Meta-analysis for VD.

Figure7 Meta-analysis for Peak velocity.
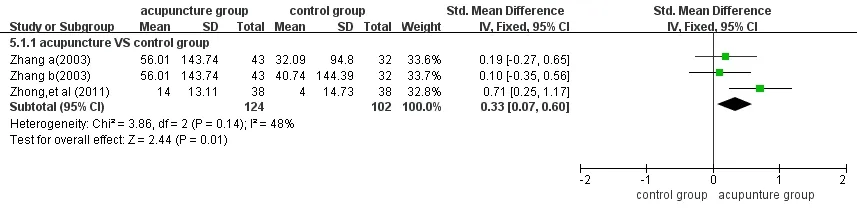
Figure8 Meta-analysis for blood flow volume.
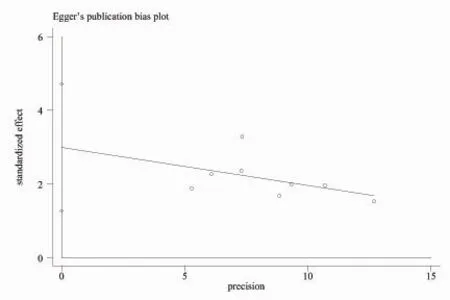
Figure9 Egger’s funnel plot of publication
Discussion
The purpose of this Meta analysis is to critically evaluate the effectiveness of acupuncture in relation to total effective rate,ulcer healing time,the hemodynamic parameters and adverse events.The review emphasized several issues with respect to both clinical practice and future research on each of these outcome areas.
Total effective rate
The findings of meta-analysis suggest that acupuncture therapy has advantages over the control group for the treatment of DFUs in overall efficiency.However,the included trials are mostly of poor quality,so the pooled result is likely to be overestimated.Clinically,the most important question is only what kind of patients with DFUs the acupuncture therapy is appropriate for.But the present evidence is still uncertainty.From the included studies,we found the patients of the target groups were distributed in 0 to 4 Wagner grades,excluding the patients in 5 Wagner grade.So it is useful to considering whether the acupuncture therapy is suitable for those excluded participants and thus increase management of DFUs’cost-effectiveness.These problems need the randomized controlled trials of higher quality with larger sample sizes to explore the potential causes.Furthermore,using purposeful sampling could lead to the distortion of clinical curative effect of acupuncture therapy.Therefore,the acupuncture-treatment populations must be determined at our reasonable discretion and founded on facts.
Another related problem was the way to choose the period of treatment and dose of acupuncture.Up to now,there are no relevant provisions.The optimum treatment cycle and dose of acupuncture are still unknown.Combining the third figure,we find the effectiveness of acupuncture changes over time and tend to be non-linear correlation.So it is important to understand whether we should adjust acupuncture stimulation dose and frequency in the light of the dynamics and tolerance of acupuncture therapy’s time effect,and undertake acupuncture therapy according to its maximum effect size and resistance profile.It is critical to objectively choose the time of treatment and the courses.After all,the incidence of injuries of acupuncture for these patients is relatively high.Studies with a multilateral,larger sample size are needed to explore a series of problems.
Time to ulcer healing
Injured skin as a portal of entry for bacteria can contribute to wound infection[19].Consequently,accelerating wound closure as early as possible is one of the most critical strategies for the treatment of DFUs.A total of 3 studies included the contemporary articles discussed the issue.The descriptive analysis agreed that acupuncture had a therapeutic benefit in shortening the healing time.Immense amounts of research for acupuncture mechanism are more concerned with diabetic peripheral neuropathy(DPN)which contains DFUs,but there is less documentation aimed at DFUs.The findings of meta-analysis suggest that acupuncture therapy has advantages in overall efficiency.There are some explanations why acupuncture therapy may be effective in accelerating healing:a)Improve the local blood circulation and strengthen metabolism to stimulate tissue repair[20],b)Adjust and enhance the body immunity and resistance,and it is likely to minimize the range of risk factors[21],and c)The thermal effect of moxibustion therapy promote the ulcer dry[13].
The hemodynamic parameters
Lower extremity arterial diseases in patients with DFUs are characterized by arterial stenos is and thickened vascular wall[22].These pathological variations often lead to local circulatory deficiency and quickened blood flow velocity,accordingly,aggravate the destruction of vascular wall[22].So it is considered abnormal vessel and flow are one of the core reasons for foot lesions[23].In this study,acupuncture therapy was more effective than the control group in blood flow volume.However,insufficient evidence suggests that acupuncture is in a position to dilate vessel diameter and increase peak velocity.The mechanism of acupuncture should be explored further with more rigorous studies because acupuncture continues being widely used for this condition,which suggests that acupuncture may be an effective intervention for DFUs.
Adverse events
Two of the studies,severally,reported injection pain and burn caused by acupuncture,but none was serious.It is necessary to explore whether we should make a prophylactic use of analgesic for patients with pain and generalize a safer therapy method,such as an application of moxibustion massager.Another related problem is that studies failed to mention the follow-up effect,hence,there is no knowledge of recurrence rate of DFUs in the long term.And it is not conductive to assess the long-term efficacy of acupuncture which can form the basis for consolidation therapy.Future studies must provide some account of this patient-centred outcome as it’s clearly a vital consideration in establishing the use of this therapy.
Limitations of the review
Our review has multiple limitations.The most significant one is clearly the paucity of the primary studies.Both of low methodological quality studies and small sample size seem to be the problems for this meta-analysis,which does not provide strong evidence in favour of acupuncture therapy.
Another potential limitation of the review is that all trials were conducted and published in China and used different treatment sessions and various simulation methods.Consequently,the generalizability of the evidence found in this study may be seriously limited given separate treatment contexts or cultural backgrounds.Moreover,the restriction of languages might lead to a publication bias and affected the validity and reliability of this systematic review.
Finally,a possible critique is that the meta-analyses combined different endpoints and control groups,such as total effective rates and the hemodynamic parameters,measured at different times.
Conclusion
By analyzing the 8 included trials,this systematic review indicates that acupuncture therapy is a safe way for DFUs.It may be most effective in shorten overall treatment time and has advantages in curative effect.It is well known that small,poor-quality studies tend to spuriously inflate the effect of an intervention,hence,well-designed and conducted trials were needed to further definitely substantiate the conclusion.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
1.Mills JL,Conte MS,Armstrong DG,Pomposelli FB,Schanzer A,Sidawy AN,et al.The society for vascular surgery lower extremity threatened limb classification system:risk stratification based on wound,ischemia,and foot infection(WIfI).JVasc Surg 2014;59:220-234.
2.Lipsky BA,Berendt AR,Cornia PB,Pile JC,Peters EJ,Armstrong DG,et al.Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections.Clin Infect Dis 2012;54:132-173.
3.Lipsky BA,Sheehan P,Armstrong DG,Tice AD,Polis AB&Abramson MA.Clinical predictors of treatment failure for diabetic foot infections:data from a prospective trial.Int Wound J 2007;4:30-38.
4.Singh N,Armstrong DG,Lipsky BA.Preventing foot ulcers in patients with diabetes.JAMA 2005;293:217-28.
5.Karthikesalingam A,Hold JE,Moxey P,Jones KG,Thompson MM&Hinchliffe RJ.A systematic review of scoring systems for diabetic foot ulcers.Diabet Med 2010;27:544-549.
6.McIntosh A,Peters J,Young R,Hutchinson A,Chiverton R,Clarkson S,et al.Prevention and management of foot problems in type 2 diabetes:clinical guidelines and evidence.Sheffield:University of Sheffield;2003.
7.Hinchliffe RJ,Andros G,Apelqvist J,Bakker K,Fiedrichs S,Lammer J,et al.A systematic review of the effectiveness of revascularization of the ulcerated foot in patients with diabetes and peripheral arterial disease.Diabetes Metab Res Rev 2012;28:179-217.
8.Zhang XJ.Clinical and Mechanism Study on Treatment of Diabetic Foot with acupuncture and moxibusion.Jinan:Shandong Traditional Chinese Medicine University,2003.
9.Yi JC,Huang LJ,Yi JP.Clinical observation of combination of acupuncture with medicine on diabetic foot.Journal of Liaoning University of TCM 2007,9(3):163-164.
10.Liberaati A,Altman DG,Tetzlaff J,Mulrow C,Gøtzsche P C,Ioannidis JP,et al.The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions:Explanation and elaboration.PLOSMedicine 2009;6:41000100.
11.Higgins JPT,Green S(Eds).Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0[updated March 2011].The Cochrane Collaboration,2011.Available from http://www.cochrane-handbook.org.
12.Higgins JP,Altman DG,Gøtzsche PC,Jüni P,Moher D,Oxman AD,,et al.The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials.British Med J 2011,343:d5928.
13.Chen WH,Huang BY,Wu BJ,Tian XF,Qu HD,Wang L,et al.Clinical observation of moxibustion massager on diabetic foot.Guangdong Medical Journal 2010,31(7):914-915.
14.Zhong ZQ,Cheng KL,Li Q,Huang XJ&Liang HL.Clinical Observation and Nursing of Danhong Injecta Injecting in the Acupoint for 0 Level Diabetic Feet.Clinical Medical Engineering 2011,18(12):1926-1928.
15.15.Liu YC.Efficacy and countermeasures in treating diabetic foot ulcer with four yellow liquid compound plus moxibustion treatment.Clinical Journal of Chinese Medicine 2011,3(8):87-88.
16.Liu AZ.The application of moxibustion-related nursing intervention in diabetic foot.Clinical Medical Engineering 2014,35(8):86-87.
17.Ma CX.The clinical observation of aged diabetic foot ulcer by Moxibustion.Journal of Mongolia TCM 2013:40-41.
18.Qi J,Liu XM,Zheng Qiu yue,et al.The effect of moxibustion by evidence in treating early stage diabetic foot.Med&Pharm JChin PLA 2013,25(6):63-64.
19.Clifford P Shearman, Robin Windhaber. Foot complications in patients with diabetes.Vascular Surgery 2010;28(6):288-292.
20.Xu H,Wang Xu.The related traditional Chinese medicine therapy of diabetic foot.Jilin Journal of Traditional Chinese Medicine 2012,32(12):1216-1217.
21.Cheng JT,Cheng GW.Moxibustion therapy treats all the various illnesses[M].Beijing:People's Military Medical Publisher,2009:5-6.
22.Liao L,Xu DF,Wang ST.CDFI examination and treatment of lower extremity arterial disease in diabetic patients.Chin J Endocrinol Metab 1999,12(3):186-188.
23.Zhang DG,Xie LL,Chao CS.Pedopathy and Local Blood Changes in Diabetic Patients.Chin J Modern Med 2000,10(2):67.
 Traditional Medicine Research2016年1期
Traditional Medicine Research2016年1期
- Traditional Medicine Research的其它文章
- TMR:A new star for the research of traditional medicine
- The effect of acupuncture plus drug versus drug alone on patients with mild cognitive impairment:a systematic review
- Massage for migraine:A meta-analysis
- Similarities and differences of doctor-patient co-operated evidence-based medical record of treating digestive system diseases with integrative medicine compared with traditional medical records
- Complete response of hepatocellular carcinoma treated with traditional herbal medicine:A case report