
三维适形放疗和放疗联合化疗对中晚期食管癌患者预后影响的比较
2016-03-07 09:31李晓宁王澜李润霄韩春
中国肿瘤临床 2016年3期
李晓宁 王澜 李润霄 韩春
三维适形放疗和放疗联合化疗对中晚期食管癌患者预后影响的比较
李晓宁王澜李润霄韩春
摘要目的:探讨三维适形放疗和放疗联合化疗中晚期食管癌患者预后影响。方法:回顾性分析2007年6月至2010年6月在河北医科大学第四医院就诊的中晚期食管癌患者245例,根据患者接受的治疗方式不同将患者分为单纯放疗组和放化疗联合治疗组,其中单纯放疗组173例接受三维适形放疗,放化疗联合治疗组72例接受三维适形放疗联合治疗,干预后1个月评价两组患者的疗效、不良反应、生存率。结果:联合治疗组的女性、年龄<62岁、淋巴结出现转移、照射剂量≥63 Gy的比例均显著高于单纯放疗组,且差异具有统计学意义(P<0.05);两组患者的肿瘤发生部位以及Karnofasky评分的差异无统计学意义(P>0.05);联合治疗组患者的有效率显著高于单纯放疗组,且差异具有统计学意义(P<0.05);联合治疗组患者发生食管炎、区域性复发、白细胞及血小板下降发生率显著高于单纯放疗组,且差异具有统计学意义(P<0.05);两组患者的骨髓移植、肺炎、放射肺纤维化、恶心、呕吐、食欲下降的发生率差异无统计学意义(P>0.05);联合治疗组患者5年的生存率均显著高于单纯放疗组,且差异具有统计学意义(P<0.05)。结论:对于中晚期食管癌患者,放化疗联合治疗与单纯放疗相比可以提高治疗有效率与患者生存率,引发的不良反应均在耐受范围内,值得临床推广。
关键词三维适形放疗放疗联合化疗食管癌预后
作者单位:河北医科大学第四医院放疗科(石家庄市050017)
目前,我国食管癌的发生率呈上升趋势,死亡率亦逐年上升,居恶性肿瘤第5位[1-3]。我国是食管癌的高发国家,且确诊患者70%以上为中晚期,该类患者缺乏手术治疗的指征,放疗是主要的治疗手段,但单纯放疗的5年生存率低于10%[4-6]。在西方国家以及日本,同期放化疗被认为是标准治疗方案。目前,随着设备的不断更新以及技术的逐渐提升,三维适形放疗由于其精确性可以显著降低周围组织的照射以及伤害,已经成为主要的放疗手段[7-8]。本研究回顾性分析单纯的三维适形放疗与放化疗联合治疗对中晚期食管癌患者的预后影响,为临床治疗提供科学依据。
1 材料与方法
1.1一般资料
本研究回顾性分析2007年6月至2010年6月在河北医科大学第四医院就诊的中晚期食管癌患者245例,其中男性188例,女性57例,平均年龄为(65.26±8.69)岁,淋巴结转移的患者为42例,肿瘤部位分布情况为颈胸上端112例,胸中下段123例,多发患者为10例,Karnofsky平均评分为(85.37±6.72)分。
1.1.1纳入标准本研究纳入所有患者的Karnofsky评分均≥70分;均经病理组织学诊断确诊为食管癌;均经过会诊确定无法进行外科手术治疗;除少数发生淋巴结转移外无合并远处脏器的转移;除罹患食管癌外无其他重大器官的病变;临床资料齐全。
1.1.2排除标准排除临床诊断非食管癌的患者;接受食管癌手术治疗的患者;发生远处转移的患者;心脏、肝脏、脾脏、肾脏、肺等器官发生病变的患者;临床资料不齐全。
1.2方法
1.2.1分组方法根据食管癌患者接受的治疗方式不同将患者分为单纯放疗组和放化疗联合治疗组,其中单纯放疗组接受三维适形放疗,放化疗联合治疗组接受三维适形放疗联合治疗,其中单纯放疗组患者173例,联合治疗组72例,两组患者的临床资料对比情况见表1。
1.2.2单纯放疗组患者的治疗本组患者接受三维适形放疗,所有患者取仰卧位行热塑膜固定,三维治疗计划系统为Pinnacle 9.2计划系统。肿瘤靶区主要包括CT扫描可见的食管癌变的病灶以及转移的淋巴结,临床靶区指肿瘤靶区外扩宽度(前后左右)6~8 mm左右,食管纵轴外延30 mm左右,计划靶区由临床靶区外延6~8 mm组成,并同时勾画出临近的组织以及器官,其中包括肺脏、气管、脊髓。采用6MV直线,1.80~2.15 Gy/次,1次/天,每周进行5天,总剂量为50~70 Gy,平均剂量为(62.72±4.83)Gy。
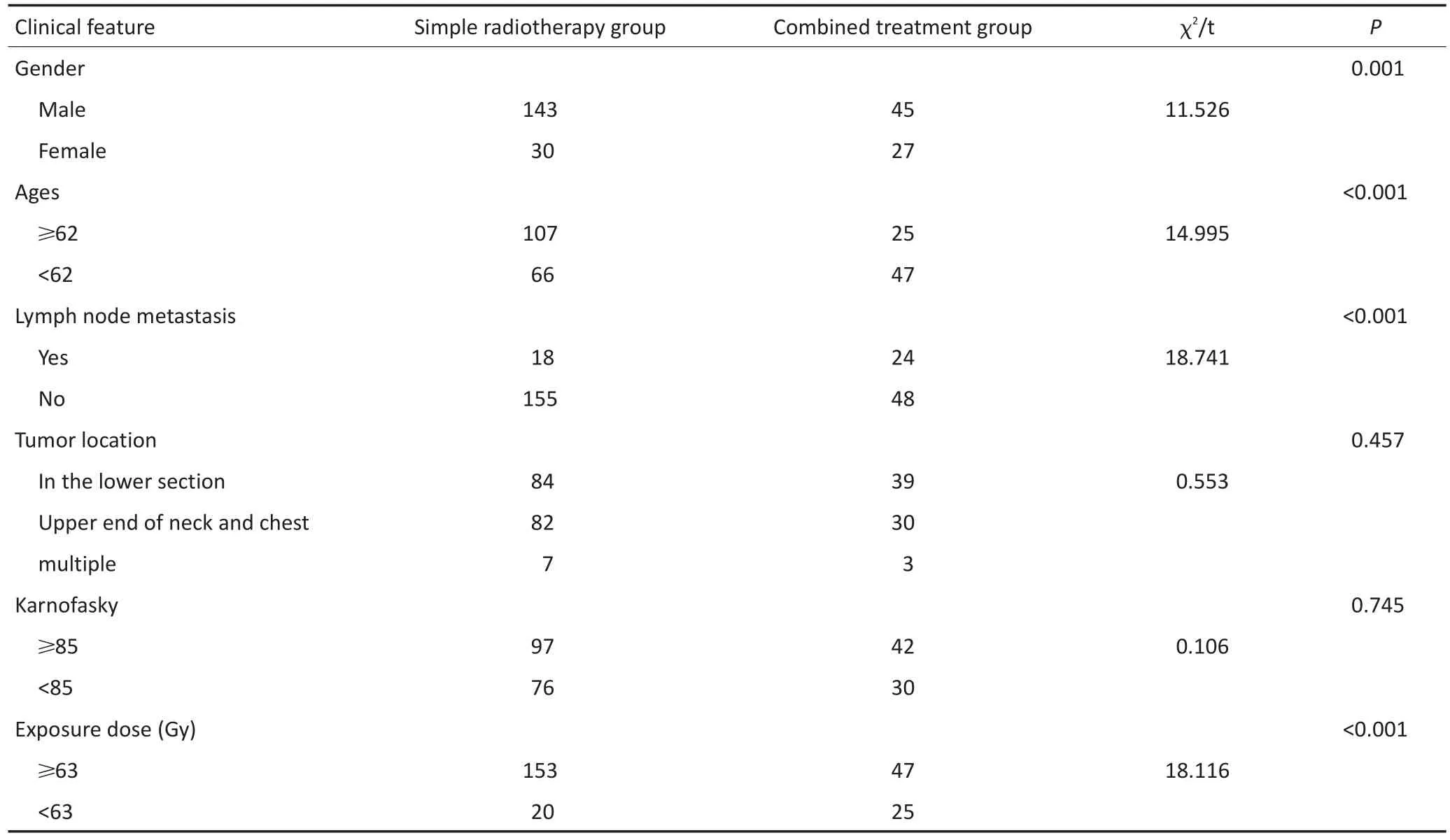
表1 两组患者临床资料的比较Table 1 Comparison of clinical data between the two groups
1.2.3联合治疗组患者的治疗本组患者的放疗与单纯放疗组患者的放疗相同,平均剂量为(61.97± 4.62)Gy,两组患者的照射量差异无统计学意义。在放疗的基础上给予化疗,化疗采用DF化疗方案。其中顺铂(DDP)75 mg/m2(第1天静脉注射),氟尿嘧啶(5-FU)500 mg/m2(第1~4天静脉注射)为1个疗程,其中治疗的第1天和第29天各给予1个疗程。
1.2.4观察指标干预后1个月评价两组患者的疗效、不良反应、5年生存率。其中疗效的评价根据体检以及影像学资料进行综合评定,分为完全缓解(CR)、部分缓解(PR)、病情稳定(SD)以及病情恶化(PD)。不良反应主要包括食管炎症、骨髓抑制、肺炎、放射肺纤维化、区域性复发、远处转移、白细胞下降、红细胞下降以及血小板下降。将照射野内与照射野外复发的患者均统计为区域性复发患者。所有数据均根据随访获得,随访时间最长为60个月。总有效率=(完全缓解例数+部分缓解例数)/总例数×100%
1.3统计学方法
本研究数据均采用SPSS 19.0统计软件进行处理。定量数据均采用平均值±标准差(±s)进行表示,计量资料采用t检验,计数资料均采用χ2检验,两组患者的生存率采用Kaplan-Meier法进行分析。P<0.05为差异具有统计学意义。
2 结果
2.1两组患者临床资料的比较
联合治疗组的女性、年龄<62岁、淋巴结出现转移、照射剂量≥63 Gy的患者比例均显著高于单纯放疗组,且差异具有统计学意义(P<0.05);两组患者的肿瘤发生部位以及Karnofasky评分的差异无统计学意义(表1)。
2.2两组患者疗效的比较
联合治疗组患者的有效率显著高于单纯放疗组,且差异具有统计学意义(表2)。
2.3两组患者不良反应的比较
联合治疗组患者发生食管炎、区域性复发、白细胞下降以及血小板下降发生率显著高于单纯放疗组,且差异具有统计学意义,两组患者的骨髓抑制、肺炎、放射肺纤维化、食欲下降、恶心、呕吐的发生率差异无统计学意义(表3)。
2.4两组患者生存率的比较
Kaplan-Meier分析显示联合治疗组患者的3~5年生存率均显著高于单纯放疗组(表4,图1)。

表2 两组患者疗效的比较Table 2 Comparison of curative effect between the two groups

表3 两组患者不良反应的比较Table 3 Comparison of adverse reactions between the two groups

表4 两组患者生存例数统计Table 4 Statistics of survival of patients in the two groups

图1 两种治疗方式的生存曲线图Figure 1 Survival curves of two treatment modalities
3 讨论
食管癌为我国常见恶性肿瘤之一,发生率和死亡率均较高,且有上升趋势。国外前瞻性研究报道,无法外科手术治疗的食管癌患者采用放化疗联合治疗比单纯放疗的生存率要高,而且许多的研究也证实该项临床研究的意义[9-10],但是也有许多研究指出食管癌患者采用放化疗联合治疗不会有效提高生存率,得出不同的结论[10-11]。本研究行回顾性分析比较三维适形放疗和放疗联合化疗对中晚期食管癌患者预后的影响,结果显示放化疗联合治疗可有效改善无法外科治疗食管癌患者的预后。
联合治疗组的女性、年龄<62岁、淋巴结出现转移、照射剂量≥63 Gy的患者比例均显著高于单纯放疗组,且差异具有统计学意义(P<0.05);两组患者的肿瘤发生部位以及Karnofasky评分的差异无统计学意义(P>0.05)。罹患食管癌的女性患者、年龄较为年轻的患者、淋巴结发生转移的患者更易接受放化疗联合治疗。在治疗过程中要对此引起足够的重视,此类患者采用放化疗联合治疗的效果较好。
联合治疗组患者的有效率显著高于单纯放疗组,且差异具有统计学意义。联合治疗组患者2、3、4、5年的生存率均显著高于单纯放疗组,且差异具有统计学意义。联合治疗组患者发生食管炎、区域性复发、白细胞及血小板下降发生率显著高于单纯放疗组,且差异具有统计学意义。两组患者的骨髓抑制、肺炎、放射肺纤维化、远处转移、红细胞下降的发生率的差异无统计学意义。放化疗联合治疗会在短期引发多种并发症,但可提高患者的有效治愈率。2010年王玉祥等[12]研究指出,三维适形放疗组的4年生存率显著高于常规放疗组,有研究指出三维适形放疗联合化疗后疗效显著高于单纯放疗组,且3年的生存率显著高于单纯放疗组[13]。原因为单纯的放疗虽然可以杀灭和损伤肿瘤细胞,但是可能会导致肿瘤细胞处于亚致死状态,放射治疗结束后将重新复活,而且肿瘤细胞还具有很强的损伤修复能力。化疗药物可以有效抑制肿瘤细胞的M期有丝分裂,并有效杀死肿瘤细胞,再通过诱导凋亡促进厌氧细胞的氧化,组织中肿瘤细胞的增殖最终起到抑制肿瘤血管生成的作用,并可消除微小的病灶[14-15]。DDP以及5-FU的主要作用为通过抑制肿瘤细胞的DNA合成途径,而对其产生杀伤和抑制作用,还可以通过改变肿瘤细胞的增殖动力学,最终增强敏感性。因此,放疗联合化疗还可有效抑制放疗后细胞的亚致死性以及肿瘤细胞的损伤修复作用,而且在化疗的过程中会降低癌细胞的生长速度并缩小病灶面积,减少肿瘤的营养供应,最终增强放疗的敏感性。综合以上放化疗联合治疗的优势,有效率显著高于单纯放疗组[16-17]。由于药物毒副作用以及对正常细胞的抑制,患者白细胞受到抑制导致免疫力降低,短期并发症会相应地增多,但均在患者的耐受范围内。
综上所述,对于中晚期食管癌患者,放化疗联合治疗与单纯放疗相比不仅可提高治疗有效率,而且可以有效地提高生存率,虽引发不良反应但均在耐受范围内,值得临床推广。
参考文献
[1] Han C, Wang L, Zhu SC, et al. Evaluation of prognosis of clinical staging for esophageal carcinoma treated with non-surgical methods-addition with analysis of 225 patients[J]. Chinese Journal of Radiation Oncology, 2011, 20(2):109-112.[韩春,王澜,祝淑钗,等.非手术治疗食管癌临床分期标准对225例放疗患者的预后评价[J].中华放射肿瘤学杂志,2011,20(2):109-112.]
[2] Zhao WY, Zhang LZ, Wang JR, et al. Three-dimensional conformal radiotherapy combined with different chemotherapy in the treatment of advanced esophageal cancer[J]. Journal of Modern Oncology, 2012, 20(5):956-958.[赵维勇,张丽珍,王继荣,等.三维适形放疗联合不同化疗方案治疗中晚期食管癌的临床研究[J].现代肿瘤医学,2012,20(5):956-958.]
[3] Welsh J, Settle SH, Amini A, et al. Failure patterns in patients with esophageal cancer treated with definitive chemoradiation[J]. Cancer, 2012, 118(10):2632-2640.
[4] Shen WB, Gao HM, Zhu SC, et al. Efficacy of three-dimensional radiotherapy±chemotherapy in 95 esophageal cancer patients with tracheoesophageal groove lymph nodemetastasis[J]. Chinese Journal of Radiation Oncology, 2015, 24(1):36-40.[沈文斌,高红梅,祝淑钗,等.95例伴气管食管沟淋巴结转移食管癌三维放疗±化疗疗效分析[J].中华放射肿瘤学杂志,2015,24(1):36-40.]
[5] Kole TP, Aghayere O, Kwah J, et al. Comparison of heart and coronary artery doses associated with intensity-modulated radiotherapy versus three- dimensional conformal radiotherapy for distal esophageal cancer[J]. Int J Radiat Oncology Biol phys, 2012, 83(5): 1580-1586.
[6] Zhang B, Qiao TK, Gao CX, et al. Three dimensional conformal radiotherapy combined with chemotherapy for mediate and advanced stage esophageal cancer and analysis of prognostic factors [J]. China Oncology, 2011, 21(10):803-806.[张彬,乔田奎,高彩霞, 等.同期适形放疗联合化疗治疗中晚期食管癌的临床研究[J].中国癌症杂志,2011,21(10):803-806.]
[7] Kong J, Li XN, Han C, et al. Treatment outcomes of 792 cases of esophageal carcinoma patients treated with three-dimensional radiotherapy[J]. Chinese Journal of Radiation Oncology, 2012, 21(5): 421-424.[孔洁,李晓宁,韩春,等.792例食管癌三维技术放疗的疗效分析[J].中华放射肿瘤学杂志,2012,21(5):421-424.]
[8] Li X, Zhang WC, Zhao LJ, et al. Prognostic analysis of radical 3DRT± chemotherapy in patients with esophageal cancer aged 70 years or older[J]. Chinese Journal of Radiation Oncology, 2015, 24(2):111-115.[李雪,章文成,赵路军,等.≥70岁食管癌根治性3DRT±化疗预后分析[J].中华放射肿瘤学杂志,2015,24(2):111-115.]
[9] Lin LX, Xu ZY. Analysis of long-term effect of platinum alone chemotherapy combined with radiotherapy for esophageal carcinoma without operation[J]. Cancer Research and Clinic, 2014, 26(5):339-341.[林连兴,徐志渊.铂类单药化疗联合同期放疗治疗非手术食管癌的远期效果分析[J].肿瘤研究与临床,2014,26(5):339-341.]
[10] Aggarwal A, Harrison M, Glynne-Jones R, et al. Combination external beam radiotherapy and intraluminal brachytherapy for non-radical treatment of oesophageal carcinoma in patients not suitable for surgery or chemoradiation[J]. Clinical Oncology, 2015, 27(1):56-64.
[11] Tan LJ, Xiao ZF, Zhang HX, et al. Survival comparison of three-dimensional radiotherapy alone with concurrent chemoradiotherapy for non-surgical esophageal carcinoma[J]. Chinese Journal of Radiation Oncology. 2015, 24(2):106-110.[谭立君,肖泽芬,张红星,等.不能手术食管癌三维放疗与同期放化疗生存比较[J].中华放射肿瘤学杂志,2015,24(2):106-110.]
[12] Wang YX, Wang J, Wang Y, et al. Prognosis comparison of three-dimensional conformal radiotherapy/intensity modulated radiation therapy for esophageal carcinoma with localregionallymphnodemetastasis[J].Chinese Journal of Radiation Oncology,2011,20(6):489-493.[王玉祥,王军,王祎,等.食管癌伴区域淋巴结转移三维适形与调强放疗疗效初步比较[J].中华放射肿瘤学杂志,2011,20(6):489-493.]
[13] Pan DL, Li JC, Yang Y, et al. Analysis of prognostic factors in 210 patients with advanced esophageal carcinoma after chemoradiotherapy[J]. Chinese Clinical Oncology, 2015,(2):140-144.[潘丁龙,李建成,杨燕,等.210例中晚期食管癌放化疗的预后因素分析[J].临床肿瘤学杂志,2015,(2):140-144.]
[14] Li XR, Feng JJ. The effect of radiotherapy combined with chemotherapy on the prognosis of esophageal cancer patients[J]. Shanxi Medical Journal, 2012, 41(7):688-689.[李喜茹,冯建军.放疗联合化疗对食管癌患者疗效及预后的影响[J].山西医药杂志,2012,41(7):688-689.]
[15] Fang XD. Clinical analysis of radiation therapy combined with PF regimen for esophageal cancer in 145 cases[J].Chongqing Medicine, 2012, 41(19):1936-1937,1939.[方向东.放疗同期PF方案化疗治疗145例局部晚期食管癌临床分析[J].重庆医学,2012,41(19):1936-1937.]
[16] Xia YY, Wang L, Song DA, et al. PhaseⅡclinical trial of raltitrexed plus oxaliplatin combined with concurrent radiotherapy for advanced esophageal carcinoma[J]. Chinese Journal of Clinical Oncology, 2014, (11):716-719.[夏铀铀,王磊,宋大安,等.放疗联合雷替曲塞奥沙利铂同步治疗中晚期食管癌的Ⅱ期临床研究[J].中国肿瘤临床,2014,(11):716-719.]
[17] Wang YX, Zhu SC, Su JW, et al. Analysis of three-dimensional conformal radiotherapy(3D-CRT) for esophageal carcinoma with or without nodal metastasis[J]. Chinese Journal of Clinical Oncology, 2011, 38(1):36-41.[王玉祥,祝淑钗,苏景伟,等.淋巴结转移对食管癌三维适形放疗疗效的影响[J].中国肿瘤临床,2011,38(1):36-41.]
(2015-09-01收稿)
(2016-01-10修回)

李晓宁专业方向为肿瘤放疗治疗。E-mail:51749826@qq.com
Comparison of influence of dimensional conformal radiotherapy and radiotherapy combined chemotherapy on the prognosis of patients with esophageal cancer without surgical treatment
Xiaoning LI, Lan WANG, Runxiao LI, Chun HAN
Correspondence to: Chun HAN; E-mail: 438092281@QQ.com
Department of Radiotherapy, the 4th Hospital of Hebei Medical University, Shijiazhuang 050017, China
AbstractObjective: To compare the influence of three-dimensional conformal radiotherapy and radiotherapy combined chemotherapy on the prognosis of patients with advanced esophageal cancer. Methods: A retrospective analysis from June 2007 to June 2010 in our hospital was conducted on 245 patients. Depending on the treatment, patients were classified into simple radiotherapy group and chemoradiothearapy group ,both of which received three-dimensional conformal radiotherapy. A total of 173 patients were in the radiation and chemotherapy combined treatment group, while 72 cases were in the simple radiothearapy group. One month after intervention, efficacy, adverse reactions, and survival rates of the two groups of patients were compared. Results: The proportion of women in the combination therapy group, aged <62 years, the proportion of lymph node metastasis occurrence and dose≥63Gy ratio were significantly higher than those in the radiotherapy group, respectively. The difference was statistically significant (P<0.05). However, the tumor location and Karnofasky scores of two groups of patients indicated a difference that was not statistically significant (P> 0.05). The combined treatment group results were significantly higher than the efficiency of the radiotherapy group. The difference was statistically significant (P<0.05). In the combined treatment group, significant differences were observed in the incidence of esophageal inflammation, regional recurrence, white blood cell, and platelet decrease. The difference was statistically significant (P<0.05). However, the difference in the incidence of bone marrow transplantation, pneumonia, radiation pulmonary fibrosis, nausea, vomiting, and loss of appetite was not statistically significant (P>0.05). The five-year survival rate of combination group were significantly higher than that of the radiotherapy group, and the difference was statistically significant (P<0.05). Conclusion: For advanced esophageal carcinoma patients, radiotherapy and chemotherapy combined with radiotherapy improved efficiency of treatment and effectively improved survival rate. Although the proposed treatment could lead to adverse reactions, these effects are within the range of tolerance, which makes the said treatment worthy of clinical promotion.
Keywords:three-dimensional conformal radiotherapy, radiotherapy combined with chemotherapy, esophageal cancer, prognosis
作者简介
通信作者:韩春438092281@QQ.com
doi:10.3969/j.issn.1000-8179.2016.03.878
猜你喜欢
祝您健康·文摘版(2020年7期)2020-07-13
中国生殖健康(2019年2期)2019-08-23
天津医科大学学报(2019年3期)2019-08-13
世界知识(2018年19期)2018-11-21
老年教育(老年大学)(2018年12期)2018-01-28
腹腔镜外科杂志(2016年9期)2016-06-01
中国卫生标准管理(2015年5期)2016-01-14
肿瘤预防与治疗(2014年2期)2014-11-24
中医研究(2014年9期)2014-03-11
中医研究(2014年2期)2014-03-11
