
慢性胰腺炎患者血液免疫指标的检测和分析
2016-01-11 02:01:47郑兆泓,赵九龙,杜婷婷等
中华胰腺病杂志 2015年2期
·论著·
慢性胰腺炎患者血液免疫指标的检测和分析
郑兆泓赵九龙杜婷婷胡良皞廖专叶博李白容季钧淘王丹林金欢李兆申
【摘要】目的检测慢性胰腺炎(CP)患者各项血液自身免疫指标的阳性率,探讨其临床价值。方法检测上海长海医院消化科就诊的409例CP患者的抗可提取性核抗原抗体(抗ENA抗体)、抗胞浆型中性粒细胞抗体、抗β2-糖蛋白1抗体(anti-β2-GPI)、抗心磷脂抗体(ACA)、抗单链-DNA抗体等25项血清相关自身免疫指标,并与系统检索的Pubmed数据库内相关文献的健康人群阳性率进行比较。结果409例CP患者中仅检出anti-β2-GPI、ACA、抗双链-DNA抗体阳性患者,阳性率分别为11.7%、1.4%、1.9%,其余指标均为阴性。其中anti-β2-GPI阳性率与健康人群相比有显著提高(11.7%比3.4%),ACA阳性率低于健康人群(1.4%比4.1%),差异均有统计学意义(P值均<0.05)。而抗单链-DNA抗体阳性率与健康人群的差异无统计学意义。结论anti-β2-GPI对于CP的诊疗具有潜在价值,ACA的临床意义尚不确定。
【关键词】胰腺炎,慢性;自身免疫疾病;生物学标记;抗β2-糖蛋白1抗体
DOI:10.3760/cma.j.issn.1674-1935.2015.02.006
收稿日期:(2015-01-08)
Detection and analysis of blood immune parameters in patients with chronic pancreatitisZhengZhaohong,ZhaoJiulong,DuTingting,HuLianghao,LiaoZhuang,YeBo,LiBairong,JiJuntao,WangDan,LinJinhuan,LiZhaoshen.DepartmentofGastroenterology,ChanghaiHospital,SecondMilitaryMedicalUniversity,Shanghai200433,China
Correspondingauthor:LiZhaoshen,Email:zhaoshen-li@hotmail.com
Abstract【〗ObjectiveTo explore the positive rate of each autoimmunity parameters in patients with chronic pancreatitis. MethodsFour hundred and nine chronic pancreatitis patients treated in Department of Gastroenterology of Changhai Hospital were selected and the 25 autoimmunity parameters included anti-ENA antibody, anti-neutrophil cytoplasmic antibody, anti-β2-GPI, anticardiolipin antibody (ACA), anti dsDNA antibody were determined, then a literature search was performed to compare the autoimmune positive rate of healthy people in Pubmed database with chronic pancreatitis patients. ResultsAmong 409 patients, the positive rates of anti β2-GPI, ACA, and anti dsDNA antibody were 11.7%, 1.4%, and 1.9%, respectively, whereas other indicators were negatively expressed. The positive rate of anti β2-GPI in CP patients was significantly higher than that of healthy group (11.7%vs3.4%), and the positive rate of ACA was lower than that of healthy group (1.4%vs4.1%), and the difference between the two groups was statistically significant (P<0.05). ConclusionsAnti β2-GPI shows some potential value in the diagnosis and treatment of chronic pancreatitis, but the clinical significance of ACA is uncertain.
【Key words】Pancreatits, chronic;Autoimmune diseases;Biological markers;anti-β2 glycoprotein 1
慢性胰腺炎(chronic pancreatitis,CP)是胰腺的一种进行性炎症性疾病。随着国人生活水平的提高,CP的发病率有增长的趋势,严重地影响了人们的工作和生活。目前关于CP的病因除了摄入酒精较为明确[1]外,其他致病因素尚不明确,影响了疾病的诊断和治疗。自身免疫性胰腺炎(autoimmune pancreatitis, AIP)作为CP的一种亚型,自身免疫指标IgG4对于其诊断的价值已得到明确[2]。对于其他特发性CP患者,自身免疫因素是不是其致病因素,是否需要对CP患者行血液自身免疫指标检测,目前尚无明确的相关研究。本研究检测CP患者(AIP除外)的血液自身免疫指标,以明确CP与自身免疫是否相关。

作者单位:200433上海,第二军医大学长海医院消化内科
通信作者:李兆申,Email: zhaoshen-li@hotmail.com
资料与方法
一、一般资料
选取2008年1月至2013年12月在上海长海医院消化内科就诊并同意接受检测的CP患者(AIP与有免疫性疾病史除外)共409例,其中男性291例,女性118例,平均年龄(34±8)岁。青少年(<18岁)患者55例。
二、检测指标
检测的血指标包括抗可提取性核抗原抗体(抗ENA抗体),抗SS-A,抗SS-B,抗JO-1,抗RNP,抗Scl-70,抗Sm,抗胞浆型中性粒细胞抗体,抗多发性肌炎硬皮病抗体,抗蛋白酶3抗体IgG,抗髓过氧化物酶抗体,抗线粒体M2抗体,抗核糖体抗体,抗肾小球基底膜抗体,抗增殖细胞核抗原抗体,抗β2-糖蛋白1抗体(anti-β2-GPI ),抗核小体抗体,抗组蛋白抗体,抗核周型中性粒细胞抗体,抗双链-DNA抗体,抗单链-DNA抗体,抗核抗体,抗平滑肌抗体,抗线粒体抗体,抗心磷脂抗体(ACA),免疫球蛋白G4亚型(IgG4),共25项自身免疫指标。
三、对照组的设置
因本研究基于大样本的临床检测,未设置相关对照组,且部分抗体在健康人群中阳性率的相关研究较少,并且尚无准确、统一的数值,故系统检索Pubmed,选取库内所有涉及健康人群相关自身免疫阳性率的文献作为对照。例如以anti-β2 glycoprotein I和anti-β2-GPI作为关键词检索Pubmed数据库,选取库内所有涉及健康人群anti-β2-GPI阳性率的相关文献共16篇[3-18],anti-β2-GPI分为IgA、IgG、IgM3型,本次检测为anti-β2-GPI总值,故单独检测anti-β2-GPI 3种分型之一的相关文献未列入统计。
四、统计学处理

结 果
一、CP患者血液自身免疫指标的阳性率
409例CP患者中48例患者的anti-β2-GPI呈阳性,阳性率11.7%。48名阳性患者中anti-β2-GPI的平均值为38.51RU/ml,预测他们的anti-β2-GPI 值分布在33.40~43.63RU/ml(95%CI),明显高于≤20RU/ml的正常参考值[19]。Pubmed数据库内所有涉及健康人群anti-β2-GPI阳性率的相关文献共16篇,纳入2 438名健康者,其中88名阳性,阳性率为3.4%。CP 患者阳性率显著高于文献报道的健康人群,差异有统计学意义(χ2=50.85,P<0.001)。
本组6例患者ACA呈阳性,阳性率1.4%。数据库涉及的健康人群阳性率的相关文献共12篇[20-31],纳入7 269名健康者,其中299例阳性,阳性率为4.1%。CP患者阳性率显著低于文献报道的健康人群,差异有统计学意义(χ2=7.07,P<0.001)
本组8例患者抗双链-DNA抗体阳性,阳性率1.9%。数据库涉及健康人群的阳性率的相关文献共5篇[32-36],纳入368名健康者,其中8名阳性,阳性率为2.1%。CP患者与健康人群的差异无统计学意义(χ2=0.01,P>0.05)。
其余22项自身免疫指标均未发现阳性者。
CP患者血anti-β2-GPI、ACA、抗双链-DNA抗体的阳性率之间有相关性(F=29.33,P<0.001)。
二、anti-β2-GPI阴性与阳性CP患者的比较
anti-β2-GPI阳性CP患者胰腺发育异常(胰腺分裂、胰管汇流异常、环状胰腺等)发生率高于阴性的CP患者,差异有统计学意义(P<0.05),其他指标的差异均无统计学意义(表1)。
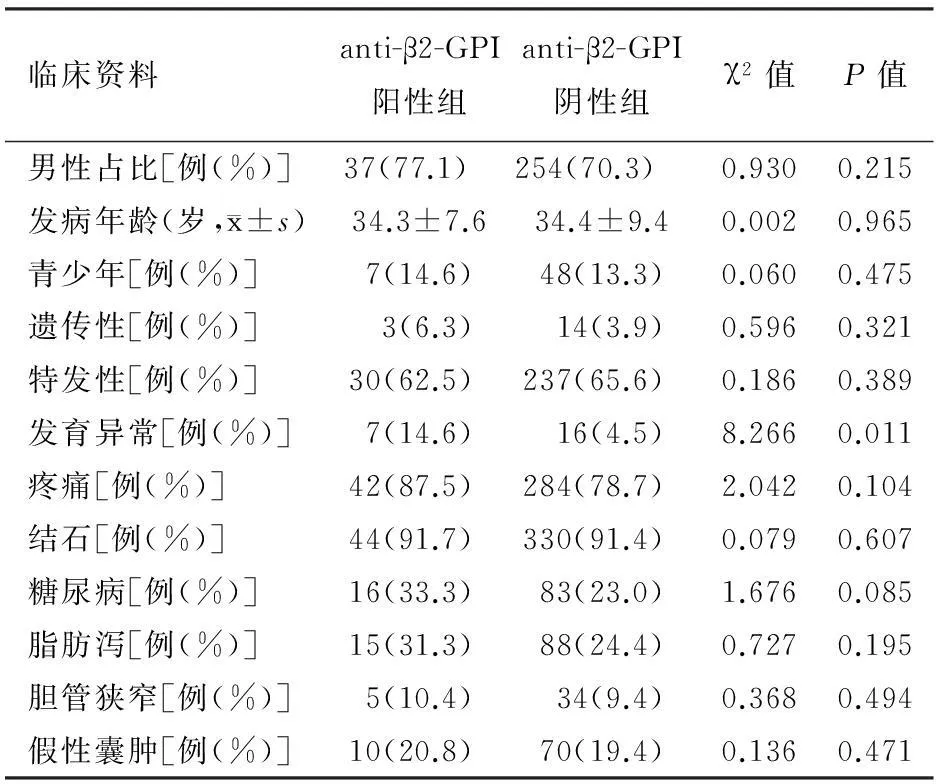
表1 anti-β2-GPI阴性与阳性CP患者的临床资料比较
三、胰腺发育异常者与正常者的比较
23例CP患者存在胰腺发育异常。胰腺发育异常CP患者的男性占比低于胰腺发育正常的CP患者,血清anti-β2-GPI阳性率显著高于胰腺发育正常的CP患者,差异均有统计学意义(P值均<0.05),其他指标的差异均无统计学意义(表2)。
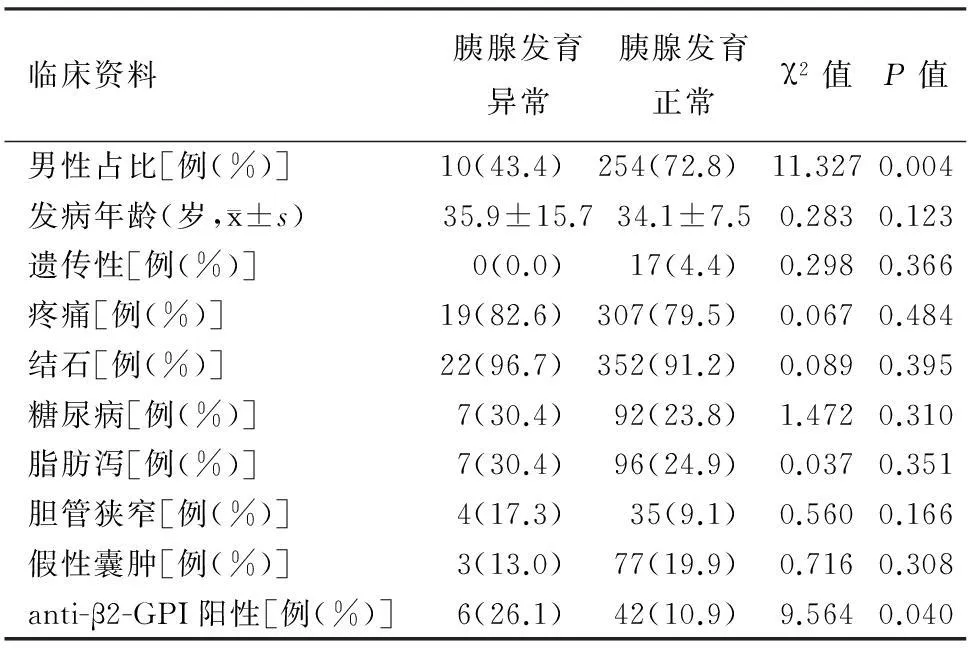
表2 胰腺发育异常与正常的CP患者的临床资料比较
讨 论
本研究检测了CP患者25项血清自身免疫指标,其中anti-β2-GPI、ACA、抗双链-DNA抗体呈现阳性。CP患者的anti-β2-GPI阳性率高于健康人群,提示该指标与CP有相关性。anti-β2-GPI为肝细胞合成并影响甘油三酯和胆固醇的代谢,它还参与凝血过程,促进微血栓形成[37-39]。Wanless等[40]报道,肝微血栓的形成与肝脏纤维化相关。CP作为一种胰腺实质萎缩、纤维化的疾病,anti-β2-GPI引起微血栓形成亦可能与CP的胰腺纤维化相关。但anti-β2-GPI的检测对于CP患者是否具有早期诊断的价值,其数值的变化是否具有评价疾病预后及判断治疗效果的价值都需要进一步研究证实。anti-β2-GPI在胰腺发育异常的患者中也显著升高,提示该指标与胰腺发育异常的相关性。anti-β2-GPI检测目前主要应用于习惯性流产,系统性红斑狼疮,脑卒中等疾病,其中在系统红斑狼疮的阳性率较高,其余疾病的阳性率大部分在10%~20%之间[3-18],与本研究所得阳性率数值相近。抗心磷脂抗体作为一种以血小板和内皮细胞膜上带负电荷的心磷脂作为靶抗原的自身抗体,其阳性率增高常见于系统性红斑狼疮、血栓形成相关疾病、习惯性流产等。本研究该抗体阳性率低于健康人群,其原因尚不明确,有无临床意义有待进一步探讨。基于自身免疫因素并不是CP常见的致病因素,且全面筛查自身免疫指标费用较高,故对CP患者无需全面检查各项免疫指标,仅检测anti-β2-GPI单项指标即可。
参考文献
[1]Strate T, Knoefel WT, Yekebas E, et al. Chronic pancreatitis: etiology, pathogenesis, diagnosis, and treatment[J]. Int J Colorectal Dis, 2003, 18(2): 97-106.
[2]Chari ST, Smyrk TC, Levy MJ. Diagnosis of autoimmune pancreatitis: the Mayo Clinic experience[J]. Clin Gastroenterol Hepatol, 2006, 4(8): 1010-1016.
[3]Chilcott IT, Margara R, Cohen H, et al. Pregnancy outcome is not affected by antiphospholipid antibody status in women referred for in vitro fertilization[J]. Fertil Steril, 2000, 73(3): 526-530.
[4]Lee RM, Emlen W, Scott JR, et al. Anti-beta2-glycoprotein I antibodies in women with recurrent spontaneous abortion, unexplained fetal death, and antiphospholipid syndrome[J]. Am J Obstet Gynecol, 1999, 181(3): 642-648.
[5]Stern C, Chamley L, Hale L, et al. Antibodies to beta2 glycoprotein I are associated with in vitro fertilization implantation failure as well as recurrent miscarriage: results of a prevalence study[J]. Fertil Steril, 1998, 70(5): 938-944.
[6]Koudriavtseva T, D′Agosto G, Mandoj C, et al. High frequency of antiphospholipid antibodies in relapse of multiple sclerosis:a possible indicator of inflammatory-thrombotic processes[J]. Neurol Sci, 2014, 35(11): 1737-1741.
[7]Alkaabi JK, Gravell D, Al-Haddabi H, et al. Haemostatic Parameters in Patients with Behcet′s Disease[J]. Sultan Qaboos Univ Med J, 2014, 14(2): 190-196.
[8]Etemadifar M, Fatemi A, Hashemijazi H, et al. Is it necessary to perform connective tissue disorders laboratory tests when a patient experiences the first demyelinating attack[J]? J Res Med Sci, 2013, 18(7): 617-620.
[9]Sater MS, Finan RR, Abu-Hijleh FM, et al. Anti-phosphatidylserine, anti-cardiolipin, anti-β2 glycoprotein I and anti-prothrombin antibodies in recurrent miscarriage at 8-12 gestational weeks[J]. Eur J Obstet Gynecol Reprod Biol, 2012, 163(2): 170-174.
[10]Spinillo A, Beneventi F, Ramoni V, et al. Prevalence and significance of previously undiagnosed rheumatic diseases in pregnancy[J]. Ann Rheum Dis, 2012, 71(6): 918-923.
[11]Mankaï A, Achour A, Thabet Y, et al. Anti-cardiolipin and anti-beta 2-glycoprotein I antibodies in celiac disease[J]. Pathol Biol(Paris), 2012, 60: 291-295.
[12]Fanopoulos D, Teodorescu MR, Varga J, et al. High frequency of abnormal levels of IgA anti-beta2-glycoprotein I antibodies in patients with systemic lupus erythematosus: relationship with antiphospholipid syndrome[J]. J Rheumatol, 1998, 25(4): 675-680.
[13]Farsi A, Domeneghetti MP, Fedi S, et al. High prevalence of anti-beta2 glycoprotein I antibodies in patients with ischemic heart disease[J]. Autoimmunity, 1999, 30(2): 93-98.
[14]Bruce IN, Clark-Soloninka CA, Spitzer KA, et al. Prevalence of antibodies to beta2-glycoprotein I in systemic lupus erythematosus and their association with antiphospholipid antibody syndrome criteria: a single center study and literature review[J]. J Rheumatol, 2000, 27(12): 2833-2837.
[15]Faden D, Tincani A, anzi P, et al. Anti-beta 2 glycoprotein I antibodies in a general obstetric population: preliminary results on the prevalence and correlation with pregnancy outcome. Anti-beta2 glycoprotein I antibodies are associated with some obstetrical complications, mainly preeclampsia-eclampsia[J]. Eur J Obstet Gynecol Reprod Biol, 1997, 73(1): 37-42.
[16]Koutroubakis IE,Petinaki E, Anagnostopoulou E, et al. Anti-cardiolipin and anti-beta2-glycoprotein I antibodies in patients with inflammatory bowel disease[J]. Dig Dis Sci, 1998, 43(11): 2507-2512.
[17]Helgadottir LB, Skjeldestad FE, Jacobsen AF, et al. The association of antiphospholipid antibodies with intrauterine fetal death: a case-control study[J]. Thromb Res, 2012, 130(1): 32-37.
[18]Roldán V, Marín F, Pineda J, et al. Annexin V levels in survivors of early myocardial infarction[J]. Rev Esp Cardiol, 2002,55(12): 1230-1234.
[19]熊艳,崔天盆,吴建民.SLE患者血清抗心磷脂抗体和抗β2糖蛋白Ⅰ抗体水平及关系[J].临床皮肤科杂志, 2001,30(6):351-352.
[20]Butkiewicz F, Kaszuba M, Brzeziński M, et al. Associations between the incidence of antiphosphatidylserine and antiphosphatidylethanolamine antibodies and clinical manifestations of systemic lupus erythematosus[J]. Pol Arch Med Wewn, 2014,124(11):573-578.
[21]Palomo IG, Mujica VE, Alarcón ML, et al. Prevalence of antiphospholipid antibodies is not different in Chilean diabetic patients and normal individuals[J]. J Diabetes Complications, 2005,19(3):133-137.
[22]Yaseen Al, Khayat ZA, Waheda NE, et al. The prevalence of positive serum anticardiolipin antibodies and asymptomatic bacteriuria in women with recurrent abortions[J]. Eurasian J Med, 2013,45(1):39-42.
[23]Ferrer-Oliveras R, Llurba E, Cabero-Roura L, et al. Prevalence and clinical usefulness of antiphospholipid and anticofactor antibodies in different Spanish preeclampsia subsets[J]. Lupus, 2012,21(3):257-263.
[24]Elefsiniotis IS, Diamantis ID, Dourakis SP, et al. Anticardiolipin antibodies in chronic hepatitis B and chronic hepatitis D infection, and hepatitis B-related hepatocellular carcinoma. Relationship with portal vein thrombosis[J]. Eur J Gastroenterol Hepatol, 2003,15(7):721-726.
[25]Rajewski M, Skrzypczak J. Frequency of antiphospholipid antibodies and antiphospholipid syndrome in women with recurrent miscarriages[J].Ginekol Pol, 2011,82(1):32-38.
[26]Markic′ J, Mestrovic′ M, Valic′ I, et al. Frequency of anticardiolipin, antinuclear and anti-beta2 glycoprotein I antibodies in children with epilepsy[J]. Coll Antropol, 2007,31(3):739-742.
[27]Karoui S, Sellami MK, Laatar AB, et al. Prevalence of anticardiolipin and anti-beta2-glycoprotein I antibodies in celiac disease[J]. Dig Dis Sci, 2007,52(4):1096-1100.
[28]Chen WH, Kao YF, Lan MY, et al. The increase of blood anticardiolipin antibody depends on the underlying etiology in cerebral ischemia[J]. Clin Appl Thromb Hemost, 2006,12(1):69-76.
[29]Wang Z, Fan Y, Wu G. Relation between fetal intrauterine growth retardation and anticardiolipin antibodies[J]. Zhonghua Fu Chan Ke Za Zhi, 1997,32(10):623-625.
[30]Liozon F, Jauberteau-Marchan MO, Boutros-Toni F, et al. Anticardiolipin antibodies and Horton disease[J]. Ann Med Interne (Paris), 1995,146(8):541-547.
[31]Pattison NS, Chamley LW, McKay EJ, et al. Antiphospholipid antibodies in pregnancy: prevalence and clinical associations[J]. Br J Obstet Gynaecol, 1993,100(10):909-913.
[32]Saigal R, Goyal LK, Agrawal A, et al. Anti-nucleosome antibodies in patients with systemic lupus erythematosus: potential utility as a diagnostic tool and disease activity marker and its comparison with anti-dsDNA antibody[J].J Assoc Physicians India, 2013,61(6):372-377.
[33]Kekow M, Barleben M, Drynda S, et al. Long-term persistence and effects of fetal microchimerisms on disease onset and status in a cohort of women with rheumatoid arthritis and systemic lupus erythematosus[J]. BMC Musculoskelet Disord, 2013, 14:325.
[34]Blondin DA, Zhang Z, Shideler KK, et al. Prevalence of non-organ-specific autoantibodies in patients with pemphigus vulgaris[J]. J Cutan Med Surg,2009,13(2):82-87.
[35]Chen HY, Guo JL, Li ZG. Significance of anti-cell membrane-associated DNA (mDNA) antibodies in systemic lupus erythematosus[J]. Clin Rheumatol, 2008,27(2):183-187.
[36]Croquefer S, Renaudineau Y, Jousse S, et al. The ananti-alpha-actinin test completes ananti-DNA determination in systemic lupus erythematosus[J]. Ann N Y Acad Sci, 2005,1050:170-175.
[37]McNally T, Crook M, Mackie IJ, et al. Beta 2 glycoprotein-I antigen is increased in primary hyperlipidaemia[J]. Br J Haematol, 1994, 88(2): 424-426.
[38]Schousboe I, Rasmussen MS. The effect of beta 2-glycoprotein I on the dextran sulfate and sulfatide activation of the contact system (Hageman factor system) in the blood coagulation[J]. Int J Biochem, 1988, 20(8): 787-792.
[39]Balasubramanian K, Killion JJ, Schroit AJ. Estimation of plasma beta-2-glycoprotein levels by competitive ELISA[J]. Thromb Res, 1998, 92(2): 91-97.
[40]Wanless IR, Liu JJ, Butany J. Role of thrombosis in the pathogenesis of congestive hepatic fibrosis (cardiac cirrhosis) [J〗. Hepatology, 1995, 21(5): 1232-1237.
(本文编辑:屠振兴)
猜你喜欢
科普童话·神秘大侦探(2022年11期)2022-05-30 03:21:35
中国医学影像学杂志(2021年6期)2021-08-13 08:43:38
恋爱婚姻家庭(2020年27期)2020-10-09 04:16:18
百花洲(2018年1期)2018-02-07 16:34:52
瞭望东方周刊(2017年45期)2017-12-08 21:37:48
中外医疗(2016年15期)2016-12-01 04:25:39
实用肝脏病杂志(2015年5期)2015-12-03 06:28:03
结核与肺部疾病杂志(2015年1期)2015-07-18 11:09:22
现代电生理学杂志(2015年1期)2015-07-18 11:02:15
肝胆胰外科杂志(2015年4期)2015-02-27 11:12:23
