
The transdiagnostic dimension of psychosis: implications for psychiatric nosology and research
2015-12-09 05:19JimVANOS
上海精神医学 2015年2期
Jim VAN OS
•Commentary•
The transdiagnostic dimension of psychosis: implications for psychiatric nosology and research
Jim VAN OS
psychosis; diagnosis; nosology; epidemiology; schizophrenia; transdiagnostic
1. Introduction
Paul Bebbington’s Special Article in this issue[1]provides a fascinating perspective on the literature linking psychosis to the social world and how this relationship is impacted by emotional regulation and reasoning biases. In the last decade, this research has contributed to novel psychological treatments with exciting new results, such as the recent trial showing that a brief psychological intervention to reduce worry impacts paranoia outcomes.[2]The work discussed by Bebbington has important conceptual implications for psychiatry,as it views psychosis as a transdiagnostic dimension,the expression of which is governed by complicated underlying dynamics involving emotional and cognitive mechanisms.
Given the recent focus on transdiagnostic dimensional expression of psychopathology, during the development of DSM-5 serious consideration was given to the possible inclusion of a system of transdiagnostic dimensions, including psychosis. The introduction of transdiagnostic dimensions would have allowed for a diagnostic system combining a nomothetic groupspecific categorical diagnosis (such as schizoaffective disorder) with an idiographic person-specific set of dimensional scores – for example, scores on anxiety,depression, psychosis, mania, motivational alterations,cognition and suicidality. The advantage of such a system is that it focuses attention on the dynamic interaction of symptoms in a network of psychopathology,[3]and on how this psychopathological network is affected bythe social world.[4]Unfortunately, setting up a system of transdiagnostic dimensions proved too complicated and was not introduced in DSM-5. Nevertheless, in the transition from DSM-IV to DSM-5, psychosis became a transdiagnostic feature of several diagnostic groups,such as the psychotic variants of obsessive-compulsive disorder and body dysmorphic disorder. These shifts re flect increasing awareness that psychotic experiences are frequent not only in psychotic disorders, but also in non-psychotic disorders.
2. What is the transdiagnostic dimension of psychosis?
What have we learned about the transdiagnostic dimension of psychosis? A particularly fascinating perspective is offered by epidemiology. Conceptually and historically, psychosis has a strong association with the diagnosis of schizophrenia. As a result, psychosis has been studied predominantly in the context of a diagnosis of schizophrenia, while other disorders in the psychosis spectrum have been largely ignored. For example, a search of PUBMED on 5 April 2015 identi fied 49 979 articles with ‘schizophrenia’ in the title versus only 681 with ‘schizoaffective disorder’, 170 with‘delusional disorder’, 17 with ‘brief psychotic disorder’,and 5 with ‘psychotic disorder not otherwise speci fied(NOS)’. Thus schizophrenia is considered the dominant context for the study of psychosis. However, recent data have cast doubt on the validity of this strategy.
Methodologically comprehensive work from Finland(illustrated in Figure 1) has shown that the spectrum of psychotic disorders (including schizophrenia,schizoaffective disorder, schizophreniform disorder,delusional disorder, psychotic disorder NOS, brief psychotic disorder, psychotic depression, psychotic bipolar disorder, substance-induced psychotic disorder,psychotic disorder due to a medical condition), whilst largely ignored in research, is much broader than the diagnosis of schizophrenia alone. The total lifetime prevalence of the full spectrum of psychotic disorders is 3.5%; schizophrenia only accounts for 1% (less than one-third) of this overall prevalence. There is substantial evidence that the various disorders that make up the psychotic disorder spectrum represent different manifestations of the same underlying syndrome, sharing etiology, psychopathology, treatment approaches, and prognosis; moreover, this view is further supported by the lack of clear and consistent‘points of rarity’ between the various conditions.[5]Given the requirement of relative chronicity in the DSMIV criteria for schizophrenia (i.e., a duration of at least 6 months), the 30% fraction of the psychotic disorder spectrum meeting the criteria for schizophrenia can be considered the ‘poor outcome fraction’ of the spectrum.
3. Possible bias in psychosis research: schizophrenia
If the diagnosis of schizophrenia represents the poor outcome fraction of a much broader psychotic disorder spectrum, the interpretation of research findings about schizophrenia is not straightforward. For example, a case-control comparison between schizophrenia and healthy controls showing differences in cognition could be interpreted either as showing that (a) cognition is associated with the onset of schizophrenia, or (b)cognition predicts poor outcome within the psychotic disorder spectrum. The latter interpretation is a plausible hypothesis, given the association between cognition and universal predictors of poor outcomes in health care such as poverty[6]and education.[7]Similarly,recent research indicates strong associations between the diagnosis of schizophrenia and low social class,[8]another universal predictor of poor outcome in health care. The fact that schizophrenia research may be biased by chronicity poses a problem, as novel treatments are developed in the understanding that research findings reflect fundamental mechanisms underlying the disorder, not the mechanisms that determine the outcome of the disorder.
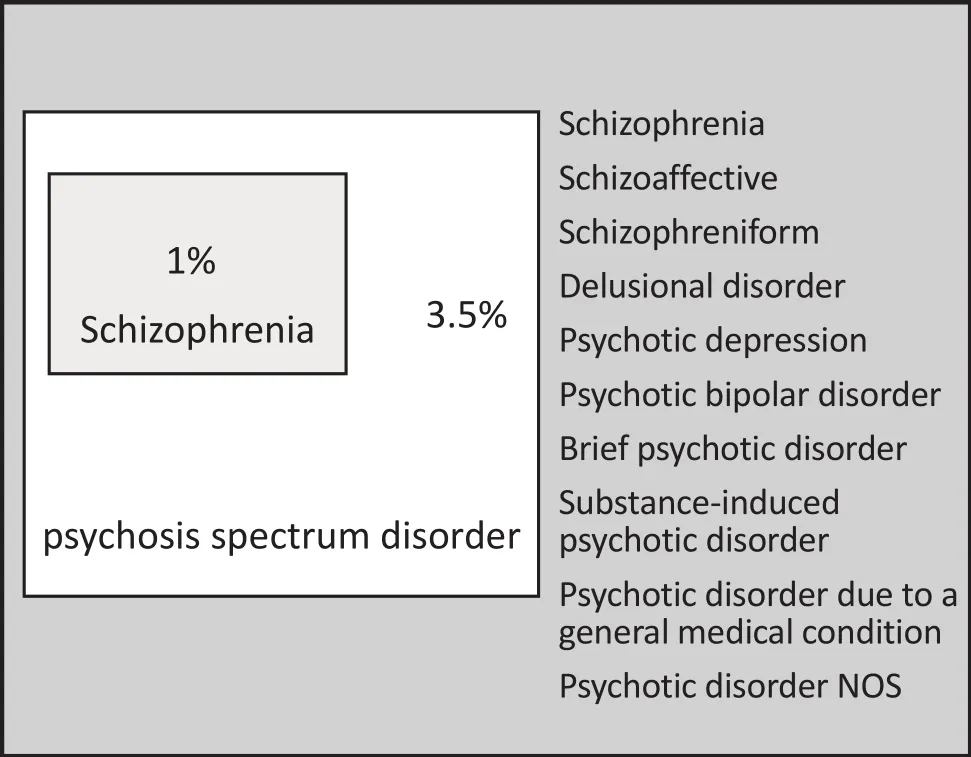
Figure 1. Schizophrenia represents only a fraction of the total psychotic disorder spectrum
3.1. Possible bias in psychosis research: non-psychotic disorders
As the study of psychosis as a transdiagnostic dimension has progressed, fascinating findings have emerged about psychotic experiences outside the psychotic disorder spectrum, that is, in the traditionally ‘non-psychotic’disorders of anxiety and depression. As illustrated in Figure 2, research has shown that around 30% of individuals with a diagnosis of anxiety or depression(the so-called ‘common mental disorders’) present with subtle sub-threshold psychotic experiences[9-11]and that 7% of the general population report psychoticlike experiences.[12]Importantly, the concurrent presence of subthreshold psychotic experiences in individuals with common mental disorders is related to the clinical severity of the mental disorder[9-11]and is a marker of poor response to pharmacological and psychotherapeutic treatments.[13,14]These findings indicate that current diagnostic criteria for non-psychotic disorders neglect an important psychopathological element that has a major influence on clinical severity and treatment response, an omission that may distort scienti fic findings about these conditions.
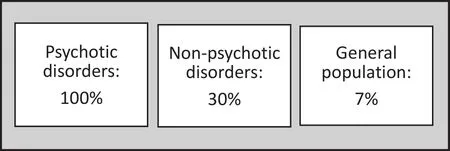
Figure 2. Transdiagnostic prevalence of psychotic symptoms and psychotic experiences
4. Towards an agnostic network model of diagnosis in psychiatry
The work presented by Bebbington is compatible with the proposition that mental disorders are reducible to sets of symptoms that are connected through systems of causal relationships[15]and that are sensitive to the social world.[16]Evidence from general population studies suggests that this conceptualization of mental disorders is particularly relevant to the earliest stages of psychopathology. One indirect indicator of the existence of this proposed network model is that the transition from a given subthreshold state to a given mental disorder is not symptom-specific; for example,subthreshold psychosis predicts both psychotic and(albeit more weakly) non-psychotic outcomes.[17]A more direct indicator of the model is that the earliest expressions of psychopathology dynamically interact with each other. For example, there is evidence that transition from subthreshold psychosis to psychotic disorder is contingent on the earlier presence of subtle indices of motivational impairment (early negative symptoms);[18]the transition from subthreshold mania to bipolar disorder is contingent on the presence of earlier subthreshold psychosis;[19]and the relationship between insomnia and paranoia may be mediated by affective dysregulation.[20]Interaction may also occur between symptoms within the same domain; for example, studies have shown that early hallucinatory states are more likely to result in transition to a clinical disorder when there is concurrent delusional ideation.[21]Similarly,subthreshold psychosis is associated with subthreshold depression and subthreshold mania in a dose-response fashion (suggesting a causal link); the stronger the association between the two domains, the greater the risk of transition to a clinical disorder.[22]Finally, many individuals with subthreshold psychosis present to clinical services with anxiety disorders or depressive disorders; in individuals with these common mental disorders the concurrent presence of subthreshold psychosis has a negative impact on the course and outcome of the disorder.[13,14]Clearly, the paradigm of subthreshold psychosis which considers these symptoms as specific predictors of psychotic disorder needs to be reconsidered; subthreshold psychosis may also be a predictor of the course and outcome of nonpsychotic disorders.[23]
5. Conclusion
The work presented by Bebbington suggests that the challenge in the years to come is to understand how the earliest expressions of psychopathology form part of a dynamic circuit of symptoms that interact with each other and gradually differentiate into more speci fic, but still largely overlapping, clinical syndromes.There is evidence that the manner in which the early stages of different psychopathological systems interact with each other over time is influenced by genetic and environmental factors.[24]Similarly, it is attractive to speculate that symptom circuits in the earliest stages of psychopathology reflect the dynamics of the neural circuits that regulate affect, assignment of salience, motivational processes, and social cognition.Of particular interest is how progressive changes in the dynamics of early psychopathology contribute to changes in functioning and personal attributions of ill-health, resulting in help-seeking behavior.Finally, assessment of the early dynamic interaction of symptoms over time facilitates person-specific diagnostic formulations, and the development of individualized treatments that target the most dominant links in the dynamic circuit of early psychopathology.[25]
Con flict of interest
The author reports no con flict of interest related to this manuscript
Funding
The preparation of this manuscript was funded by the European Community’s Seventh Framework Program under grant agreement No. HEALTH-F2-2009-241909(Project EU-GEI).
1. Bebbingtion P. Unravelling psychosis: psychosocial epidemiology, mechanism, and meaning.Shanghai Arch Psychiatry.2015; 27(2): 70-81. Epub 2015 Apr 2. doi: http://dx.doi.org/10.11919/j.issn.1002-0829.215027
2. Freeman D, Dunn G, Startup H, Startup H, Pugh K, Cordwell J, et al. In:An explanatory randomised controlled trial testing the effects of targeting worry in patients with persistent persecutory delusions: the Worry Intervention Trial (WIT).Southampton (UK); 2015
3. van Os J. The dynamics of subthreshold psychopathology:implications for diagnosis and treatment.Am J Psychiatry.2013; 170: 695-698. doi: http://dx.doi.org/10.1176/appi.ajp.2013.13040474
4. van Os J, Lataster T, Delespaul P, et al. Evidence that a psychopathology interactome has diagnostic value,predicting clinical needs: an experience sampling study.PLoS One. 2014; 9: e86652. doi: http://dx.doi.org/10.1371/journal.pone.0086652
5. van Os J, Kapur S. Schizophrenia.The Lancet. 2009; 374: 635-645. doi: http://dx.doi.org/10.1016/S0140-6736(09)60995-8
6. Mani A, Mullainathan S, Shafir E, Zhao J. Poverty impedes cognitive function.Science. 2013; 341: 976-980. doi: http://dx.doi.org/10.1126/science.1238041
7. Nisbett RE, Aronson J, Blair C, Dickens W, Flynn J, Halpern DF.Intelligence: new findings and theoretical developments.Am Psychol.2012; 67: 130-159. doi: http://dx.doi.org/10.1037/a0026699
8. Agerbo E, Sullivan PF, Vilhjálmsson BJ,Pedersen CB,Mors O,Børglum AD, et al. Polygenic risk score, parental socioeconomic status, family history of psychiatric disorders,and the risk for schizophrenia: a Danish population-based study and meta-analysis.JAMA Psychiatry. 2015; PMID:25830477
9. Kelleher I, Keeley H, Corcoran P, Lynch F, Fitzpatrick C, Devlin N, et al. Clinicopathological significance of psychotic experiences in non-psychotic young people: evidence from four population-based studies.Br J Psychiatry. 2012; 201:26-32.
10. Wigman JT, van Nierop M, Vollebergh WA, et al. Evidence that psychotic symptoms are prevalent in disorders of anxiety and depression, impacting on illness onset, risk,and severity--implications for diagnosis and ultra-high risk research.Schizophr Bull. 2012; 38: 247-57
11. Jeppesen P, Clemmensen L, Munkholm A, Rimvall MK, Rask CU, Jørgensen T, et al. Psychotic experiences co-occur with sleep problems, negative affect and mental disorders in preadolescence.J Child Psychol Psychiatry. 2015; 56(5): 558-565. doi: http://dx.doi.org/10.1111/jcpp.12319
12. Linscott RJ, van Os J. An updated and conservative systematic review and meta-analysis of epidemiological evidence on psychotic experiences in children and adults: on the pathway from proneness to persistence to dimensional expression across mental disorders.Psychol Med. 2013; 43: 1133-1149
13. Wigman JT, van Os J, Abidi L, Huibers MJ, Roelofs J, Arntz A,et al. Subclinical psychotic experiences and bipolar spectrum features in depression: association with outcome of psychotherapy.Psychol Med. 2014; 44: 325-336. doi: http://dx.doi.org/10.1017/S0033291713000871
14. Perlis RH, Uher R, Ostacher M, Goldberg JF, Trivedi MH, Rush AJ, et al. Association between bipolar spectrum features and treatment outcomes in outpatients with major depressive disorder.Arch Gen Psychiatry. 2011; 68: 351-360. doi: http://dx.doi.org/10.1001/archgenpsychiatry.2010.179
15. Kendler KS, Zachar P, Craver C. What kinds of things are psychiatric disorders?Psychological Medicine. 2010; 41(6):1-8. doi: http://dx.doi.org/10.1017/S0033291710001844
16. Guloksuz S, van Nierop M, Lieb R, et al. Evidence that the presence of psychosis in non-psychotic disorder is environment-dependent and mediated by severity of nonpsychotic psychopathology.Psychol Med. 2015; 42(11): 1-13.http://dx.doi.org/10.1017/S0033291715000380
17. Kaymaz N, Drukker M, Lieb R, Wittchen H-U, Werbeloff N, Weiser M,et al. Do subthreshold psychotic experiences predict clinical outcomes in unselected non-help-seeking population-based samples? A systematic review and meta-analysis, enriched with new results.Psychol Med.2012; 42: 2239-2253. doi: http://dx.doi.org/10.1017/S0033291711002911
18. Dominguez MD, Saka MC, Lieb R, Wittchen HU, van Os J. Early expression of negative/disorganized symptoms predicting psychotic experiences and subsequent clinical psychosis: a 10-year study.Am J Psychiatry. 2010;167: 1075-1082. doi: http://dx.doi.org/10.1176/appi.ajp.2010.09060883
19. Kaymaz N, van Os J, de Graaf R, Ten Have M, Nolen W, Krabbendam L. The impact of subclinical psychosis on the transition from subclinicial mania to bipolar disorder.J Affect Disord. 2007; 98: 55-64
20. Freeman D, Stahl D, McManus S, Meltzer H, Brugha T, Wiles N, et al. Insomnia, worry, anxiety and depression as predictors of the occurrence and persistence of paranoid thinking.Soc Psychiatry Psychiatr Epidemiol. 2012; 47: 1195-1203. doi: http://dx.doi.org/10.1007/s00127-011-0433-1
21. Smeets F, Lataster T, Dominguez MD, Hommes J, Lieb R,Wittchen H-U, et al. Evidence that onset of psychosis in the population reflects early hallucinatory experiences that through environmental risks and affective dysregulation become complicated by delusions.Schizophre Bull. 2012; 38:531-542. doi: http://dx.doi.org/10.1093/schbul/sbq117
22. van Rossum I, Dominguez MD, Lieb R, Wittchen HU, van Os J. Affective dysregulation and reality distortion: a 10-year prospective study of their association and clinical relevance.Schizophre Bull. 2011; 37: 561-571. doi: http://dx.doi.org/10.1093/schbul/sbp101
23. van Os J, Murray RM. Can we identify and treat"schizophrenia light" to prevent true psychotic illness?BMJ.2013; 346: f304
24. Wigman JT, Collip D, Wichers M, Delespaul P, Derom C,Thiery E, et al. Altered transfer of momentary mental states(ATOMS) as the basic unit of psychosis liability in interaction with environment and emotions.PLoS One. 2013; 8: e54653.doi: http://dx.doi.org/10.1371/journal.pone.0054653
25. van Os J, Delespaul P, Wigman J, Myin-Germeys I, Wichers M. Beyond DSM and ICD: introducing "precision diagnosis"for psychiatry using momentary assessment technology.World Psychiatry. 2013; 12:113-117. doi: http://dx.doi.org/10.1136/bmj.f304
, 2015-04-05; accepted, 2015-04-07)
Jim van Os trained in Psychiatry at the Institute of Psychiatry, King’s College, London (UK). After his clinical training he was awarded a three-year UK Medical Research Council Training Fellowship in Clinical Epidemiology at the London School of Hygiene and Tropical Medicine. He is on the editorial board of European and American psychiatric journals such as ‘Acta Psychiatrica Scandinavica’,‘European Psychiatry’, ‘Psychological Medicine’, ‘Schizophrenia Research’, ‘Schizophrenia Bulletin’, and‘Early Intervention in Psychiatry’. He is also an Academic Editor at ‘PLoS ONE’. In 2011, he was elected member of the Royal Netherlands Academy of Arts and Sciences (KNAW); he appears on the 2014 Thomson-Reuter Web of Science list of the world’s ‘most in fluential scienti fic minds’ of our time. Jim van Os is coordinator of a €12M EU FP7 IP project on gene-environment interactions in schizophrenia and is also active in clinical gene-environment interaction research in depression and bipolar disorder. He was a member of the Psychosis Group of the DSM-5 Task Force.
精神病的跨诊断维度:对精神疾病的分类学与研究的意义
van Os J
精神病;诊断;疾病分类学;流行病学调查;精神分裂症;跨诊断的
Summary:If psychosis is a transdiagnostic dimension, the expression of which is governed by a dynamic set of contextual and emotional factors that are amenable to treatment, current approaches in psychiatric nosology and therapeutic research may need to be revised. The dominant approach to date is to clinically and conceptually situate psychotic symptoms in the construct of schizophrenia. However, schizophrenia,which has a lifetime prevalence of 1%, only represents the poor outcome fraction of a much broader spectrum of psychotic disorders which have a lifetime prevalence of 3.5%. Therefore, research findings in schizophrenia may reflect mechanisms of prognosis rather than fundamental associations with psychosis and other symptom domainsper se. Similarly, the discovery that up to 30% of individuals with non-psychotic common mental disorders have subthreshold psychotic symptoms that situate them on the transdiagnostic dimension of psychosis – and which impact clinical severity and treatment response – indicates that the rigid separation between ‘psychotic’ and ‘non-psychotic’ hampers both clinical practice and research.Diagnostic manuals in psychiatry would benefit from a system of transdiagnostic dimensions, including a transdiagnostic dimension of psychosis. Introduction of transdiagnostic dimensions allows for a system combining a nomothetic (i.e., group-specific) categorical diagnosis with an idiographic (i.e., person-specific)combination of dimensional scores. The advantage of such a system is that it encourages consideration of how symptoms dynamically interact with each other in a network of psychopathology, and of how this network is impacted by the social world.
[Shanghai Arch Psychiatry. 2015; 27(2): 82-86.
http://dx.doi.org/10.11919/j.issn.1002-0829.215041]
Maastricht University Medical Centre, South Limburg Mental Health Research and Teaching Network, EURON, Maastricht, The Netherlands King’s College London, King’s Health Partners, Department of Psychosis Studies, Institute of Psychiatry, London, United Kingdom
correspondence: vanosj@gmail.com
概述:如果精神病是一种跨诊断的维度,精神病性症状的出现受动态变化的情境和情感因素左右,而后者又是可治疗的,那么目前精神科疾病的分类学和治疗研究的方法可能需要修改。迄今为止,无论在临床工作上还是在疾病概念上,占主导地位的方法是将精神病性症状置于精神分裂症的框架中。然而,终生患病率为1%的精神分裂症只代表了部分预后不佳的精神病谱系障碍,而后者发生更多,终生患病率为3.5%。因此,精神分裂症的研究结果可能反映了预后相关的机制,而非精神病和其他症状维度之间本质上的相关性。同样,常见的非精神病性精神障碍中高达30%的个体有阈下精神病性症状,他们会被归于精神病的跨诊断维度之下,这些精神症状还会影响临床严重程度和治疗有效性 。上述发现也同样提示武断区分“精神病性”与“非精神病性”的做法妨碍了临床实践和研究。精神病学诊断手册可以借鉴跨诊断维度(包括精神病的跨诊断维度)的体系。引入跨诊断维度,则既能根据原则进行分类诊断(即疾病分组的特异性),又可结合个体特有的多维度综合评分(即个体特异性)。这样的益处在于促使人们思考在精神病理学中症状之间是如何动态地交互作用的,并思考社会环境是如何影响精神病理症状的。
本文全文中文版从2015年06月06日起在http://dx.doi.org/10.11919/j.issn.1002-0829.215041可供免费阅览下载
猜你喜欢
课堂内外·教师版(2022年4期)2022-05-23
健康体检与管理(2022年2期)2022-04-15
考试与评价·高一版(2021年5期)2021-08-14
天津医科大学学报(2021年3期)2021-07-21
昆明医科大学学报(2021年1期)2021-02-07
小小说大世界(2020年2期)2020-11-24
文苑(2018年19期)2018-11-09
中央民族大学学报(自然科学版)(2016年2期)2016-06-27
中国男科学杂志(2016年9期)2016-03-20
新疆大学学报(哲学社会科学版)(2015年6期)2015-10-12
- 上海精神医学的其它文章
- Unravelling psychosis: psychosocial epidemiology,mechanism, and meaning
- Finding a solution to psychosis: the emergence of a new path
- Prenatal choline and the development of schizophrenia
- Efficacy and safety of the Chinese herbal medicine shuganjieyu with and without adjunctive repetitive transcranial magnetic stimulation (rTMS) for geriatric depression: a randomized controlled trial
- Gene-based and pathway-based genome-wide association study of alcohol dependence
- Are the revised diagnostic criteria for Alzheimer’s disease useful in low- and middle-income countries?