
胸腔积液与外周血ELISPOT检测诊断结核性胸膜炎的效果比较
2015-08-24 08:56:58崔丹赵杰刘朋冲冯秀莉李志惠
天津医药 2015年6期
崔丹,赵杰,刘朋冲,冯秀莉,李志惠
胸腔积液与外周血ELISPOT检测诊断结核性胸膜炎的效果比较
崔丹,赵杰,刘朋冲,冯秀莉,李志惠△
目的 通过比较不同途径的酶联免疫斑点(ELISPOT)检测,探讨其对结核性胸膜炎的诊断价值。方法采用T-Spot-TB试剂盒对164例结核性胸腔积液和102例非结核性胸腔积液患者的外周血和胸腔积液标本进行检测。比较两组的斑点形成细胞数(SFC),采用诊断试验比较胸腔积液与外周血ELISPOT检测诊断结核性胸膜炎的灵敏度及特异度。结果 胸腔积液与外周血ELISPOT检测的受试者工作特征曲线下面积分别为0.947和0.905;胸腔积液ELISPOT检测诊断结核性胸膜炎的灵敏度(95.1%)高于外周血(89.0%);特异度(90.2%)也高于外周血(88.2%)。结论 胸腔积液较外周血ELISPOT检测具有更高的诊断结核性胸膜炎的价值。
酶联免疫斑点检测;斑点形成细胞;胸腔积液单个核细胞;外周血单个核细胞
胸腔积液是胸膜疾病的常见临床表现,其中结核性胸腔积液占胸腔积液病因的半数以上[1]。由于胸腔积液涂片抗酸染色阳性率及结核菌培养阳性率极低[2],胸膜活检为有创性检查,故结核性胸膜炎的诊断与鉴别诊断一直是临床难题,迫切需要良好的免疫学诊断指标提高工作效率。近年来,基于外周血淋巴细胞的酶联免疫斑点检测(enzyme-linked immunospotassay,ELISPOT)用于结核分枝杆菌感染的诊断较快速且敏感[3];对于诊断菌阴性肺结核及肺外结核也有重要的参考价值。由于结核感染部位具有隔室化效应,即大量淋巴细胞募集到感染部位,进一步分泌细胞因子发挥免疫学效应[4],故结核性胸膜炎胸腔积液中的局部细胞数量远高于外周血,胸腔积液ELISPOT检测有可能获得比外周血更高的诊断价值,但目前尚无确定的诊断界值。本研究通过对164例结核性胸腔积液和102例恶性胸腔积液者同时行外周血和胸腔积液的ELISPOT检测,探讨ELISPOT诊断结核性胸膜炎的临床价值。
1 对象与方法
1.1 研究对象 选取2012年1月—2015年1月入住我科的初次诊断为结核性胸膜炎的患者164例(结核组),其中男79例,女85例,年龄18~63岁,平均(39±18)岁。入选标准:(1)临床有结核中毒症状(如发热、乏力、消瘦等)。(2)胸腔积液为渗出液,腺苷脱氨酶增高。(3)胸部影像学可见结核灶或无结核灶。(4)胸水、痰检涂片或结核菌培养阳性。(5)结核菌素(PPD)试验阳性。(6)经穿刺规律抗结核治疗2个月内,临床症状消失、胸水吸收。(7)治疗观察1年无复发。选取非结核性胸膜炎患者102例(对照组),其中男58例,女44例,年龄25~65岁,平均年龄(41±16)岁;包括肺癌胸膜转移89例,胸膜间皮瘤3例,淋巴瘤2例,肺炎旁积液8例。2组均人免疫缺陷病毒阴性,无合并糖尿病,无风湿免疫系统疾病,无严重心、肝、肾功能不全。2组年龄(t=1.75)、性别构成(χ2=1.89)差异无统计学意义。
1.2 ELISPOT检测方法 分别采集2组的胸腔积液及外周血,采用英国Oxford Immunotec公司生产的T-Spot-TB试剂盒进行检测:胸腔积液分离得到胸腔积液单个核细胞(PEMC),外周血分离得到外周血单个核细胞(PBMC),并制备成浓度为2.0×106/mL的细胞悬液。细胞培养液为阴性对照,植物血凝素(PHA)为阳性对照,结核菌特异度抗原ESAT-6和CFP-10为刺激抗原。每孔加入含2.5×105个细胞的细胞悬液,将微孔板放在含5%CO2的培养箱中培养18~20 h,第2天洗板后加入生物素标记的二抗,2~8℃反应1 h,洗板后加入显色底物液,室温静置7 min,去离子水终止反应。通过酶联免疫斑点系统自动分析仪(美国CTL公司)记录斑点形成细胞数(SFC)。结果判定标准:当空白对照孔内SFC<6时,任一实验孔SFC减去空白孔SFC≥6,结果为阳性;若空白对照孔SFC≥6,任一实验孔SFC≥2倍空白孔SFC,结果为阳性;否则为阴性。如果不符合上述标准且阳性对照孔正常时,结果为无反应。
1.3 统计学方法 数据用SPSS 18.0软件进行分析,2组间SFC比较采用Mann Whitney U检验,绘制受试者工作特性曲线(ROC曲线),判定ELISPOT检测诊断结核性胸膜炎的准确性。检验水准α=0.05。
2 结果
结核组胸腔积液SFC的中位数为279个/ 106PEMC,高于外周血的44个/106PBMC(U=376.0,P<0.05)。胸腔积液ELISPOT检测诊断结核性胸腔积液的界值为103 SFCs/106PEMC,外周血则为10 SFCs/106PEMC,见图1。胸腔积液ELISPOT检测对于结核性胸腔积液诊断的灵敏度和特异度均较好,诊断效能高于外周血,见表1。
3 讨论
结核菌感染诱导的细胞免疫以Th1型细胞免疫为主,结核菌抗原特异度干扰素(IFN)-γ是其分泌的主要细胞因子。ELISPOT检测是通过检测受试者体内是否存在结核效应T淋巴细胞来判断目前受试者是否感染结核杆菌的新方法。传统对结核病的诊断主要依据细菌学检查与PPD试验,由于结核分枝杆菌(mycobacrterium tuberculosis,MTB)本身生长特点以及卡介苗(bacillus calmette-guerin,BCG)接种在我国的广泛使用,使得这些方法对结核病诊断极为有限。而ELISPOT检测不受卡介苗接种及机体免疫状态的影响,可有效筛查结核感染[5]。该技术已经成为一种新的判断结核分枝杆菌感染的快速辅助方法[6]。Pai等[7]研究表明,ELISPOT检测诊断结核的灵敏度和特异度均为93%。
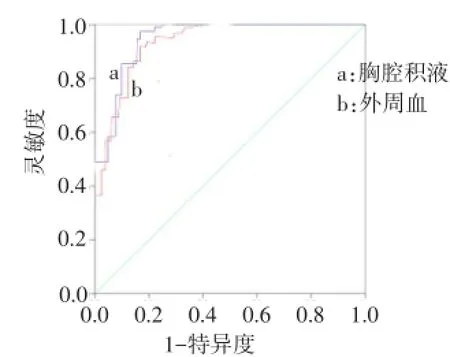
Fig.1 The ROC curve of ELISPOT test using pleural effusion or peripheral blood图1 胸腔积液与外周血ELISPOT检测诊断结核性胸膜炎的ROC曲线
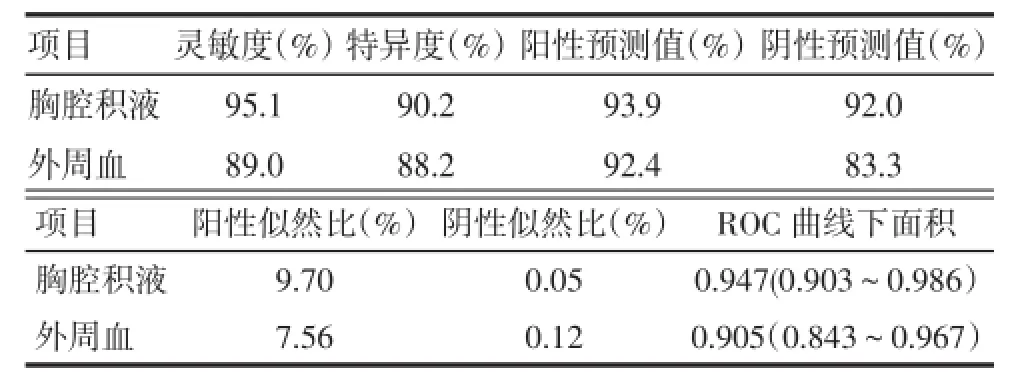
Tab.1 The index of pleural effusion or peripheral blood ELISPOT tests in diagnosing tuberculous pleurisy表1 胸腔积液与外周血ELISPOT检测诊断结核性胸膜炎的指标
虽然越来越多的报道证实ELISPOT检测在结核感染诊断中的重要价值,但也有学者提出ELISPOT检测不能区分结核潜伏感染和活动性结核,致使其诊断的特异度不高[8]。由于结核感染具有隔室化效应,胸腔积液的ELISPOT检测较外周血ELISPOT检测受结核潜伏感染影响较小,可更为准确地诊断结核性胸膜炎。本研究根据结核组和对照组的斑点数建立ROC曲线,胸腔积液和外周血ELISPOT检测曲线下面积分别为0.947和0.905,提示两种检测均可作为诊断结核性胸膜炎的有效指标。胸腔积液ELISPOT检测诊断结核性胸膜炎的灵敏度为95.1%,特异度为90.2%,分别高于外周血的89.0%和88.2%。提示胸腔积液ELISPOT检测在结核性胸膜炎的诊断与鉴别诊断中有更高的参考价值。
国外有报道显示利用ELISPOT检测结核性胸腔积液中SFC大约是外周血SFC的15倍[9]。国内也有报道表明,胸腔、腹腔积液检测SFC分别是外周血的 6.4和 31.9倍[10]。本研究中胸腔积液ELISPOT检测SFC的中位数279个/106PEMC,高于外周血的44个/106PBMC,是外周血的6.3倍,与国内报道相符。证实胸腔积液中结核菌特异性效应T淋巴细胞数要明显高于外周血,提示胸腔积液ELISPOT检测是诊断结核性胸膜炎的快速敏感的方法。
[1]Light RW.Clinical practice pleural effusion[J].N Engl J Med,2002,346(25):1971-1977.
[2]Cao YQ,Zhu ML,Su BL.Value of adenosine deaminase and interferon γ in differential diagnosis of tuberculous and malignant pleural effusion[J].Journal of Clinical Pulmonary Medicine,2012,17(9): 1666-1667.[曹月琴,朱明林,苏百龄.ADA、INF-γ在鉴别诊断结核性和恶性胸腔积液中的价值[J].临床肺科杂志,2012,17(9): 1666-1667].
[3]Kim SH,Choi SJ,Kim HB,et al.Diagnostic usefulness of a T-cell based assay for extrapulmonary tuberculosis[J].Arch Intern Med,2007,167(20):2255-2259.
[4]Nemeth J,Winkler HM,Zwick RH,et al.Recruitment of mycobacterium tubeiculosis specific CD4+T cells to the site of infection for diagnosis of active tuberculosis[J].J Intern Med,2009,265(1):163-168.[3]Seiscento M,Vargas FS,Rujula MJ,et al.Epidemiological aspects of pleural tuberculosis in the state of Sao Paulo,Brazil(1998-2005)[J].J Bras Pneumol,2009,35(6):548-554.
[4]Gopi A,Madhavan SM,Sharma SK,et al.Diagnosis and treatment of tuberculous pleural effusion in 2006[J].Chest,2007,131(3):880-888.
[5]Wang L,Liang Y,Wu XQ,et al.Analysis of Mycobacterium tuberculosis infection and follow-up in recruits of army stationed in Beijing in 2009[J].Med J Chin PLA,2012,37(8):827-832.[王兰,梁艳,吴雪琼,等.2009年驻京部队入伍新兵结核感染及随访情况分析[J].解放军医学杂志,2012,37(8):827-832].
[6]Jia HY,Lan TL,Liu F,et al.Enzyme-linked immunospot assay in the diagnosis of osteoarticular tuberculosis[J].Beijing Medicine,2012,34(10):867-870.[贾红彦,兰汀隆,刘菲,等.酶联免疫斑点试验在骨关节结核中的辅助诊断价值[J].北京医学,2012,34 (10):867-870].
[7]Pai M,Zwerling A,Menzies D,et al.Syatematic Review:T-Cell.BASED assays for the diagnosis of latent tuberculosis infection:an update[J].Ann Intem Med,2008,149(3):177.
[8]Lu F,Zhang ZD,Gao MQ,et al.The comparison of different antigens in enzyme-linked immunospot assay for the diagnosis of tuberculosis[J].Chinese Journal of tuberculosis and respiratory diseases,2009,32(8):838-841.[刘菲,张宗德,高孟秋,等.不同抗原的酶联免疫斑点检测技术对结核病的辅助诊断价值比较[J].中华结核和呼吸杂志,2009,32(8):838-841].
[9]Hirsch CS,Toossi Z,Johnson JL,et al.Augmentation of apoptosis and interferon-gamma production at sites of active Mycobacterium tuberculosis infection in human tuberculosis[J].J Infect Dis,2001,831(5):779-788.
[10]Zhang LF,Liu XQ.Detection of specific interferon-γ-secreting T cell response to mycobacterium tuberculosis rd1-encoded antigens in pleural effusions,ascites,and cerebrospinal fluid[J].Journal of the Academy of Medical Sciences China,2009,31(4):438-442.[张丽帆,刘晓清.胸腹水、脑脊液中结核分枝杆菌RD1基因编码抗原刺激后释放γ干扰素的特异性T细胞检测[J].中国医学科学院学报,2009,31(4):438-442].
(2015-03-17收稿 2015-04-10修回)
(本文编辑 闫娟)
Comparison of effects of ELISPOTs using pleural fluid and peripheral blood in the diagnosis of tuberculous pleurisy
CUI Dan,ZHAO Jie,LIU Pengchong,FENG Xiuli,LI Zhihui△
Department of tuberculosis,Hebei Chest Hospital,He Bei Province,Shijiazhuang 050041,China
△Corresponding Author E-mail:shuiqing_2001@sina.com
Objective To evaluate the effects of ELISPOT(enzyme-link immunospot)test using different samples in diagnosing tuberculous pleurisy.Methods Using T-Spot-TB kit to detect interferon-γ level in pleural effusion and peripheral blood from 164 patients with tuberculous pleural effusion and 102 patients without tuberculous pleural effusion.Number of spot forming cells(SFCs)as well as the specificity and sensitivity of the tests were compared between these two methods (ELISPOT using leural effusion or peripheral blood).Results The area under the ROC curve was 0.947 in pleural effusion Elispot test while it was 0.905 in peripheral blood Elispot test.The sensitivity of pleural effusion ELISPOT test in diagnosis of tuberculous pleurisy(95.1%)was significantly higher than that of peripheral blood ELISPOT test(89.0%).What’s more,the specificity of pleural effusion ELISPOT test in diagnosis of tuberculous pleurisy(90.2%)was higher than that in diagnosis of peripheral blood ELISPOT test(88.2%).Conclusion The pleural effusion ELISPOT test is more valuable than peripheral blood ELISPOT in the diagnosis of tuberculous pleuritis.
enzyme-linked immunospot assay;spot forming cells;pleural effusion mononuclear cells;peripheral blood mononuclear cells
R561.1
A DOI:10.11958/j.issn.0253-9896.2015.06.028
河北省胸科医院结核一科(邮编050041)
崔丹(1982),女,主治医师,硕士,主要从事呼吸、结核疾病研究
△E-mail:shuiqing_2001@sina.com
猜你喜欢
昆明医科大学学报(2020年12期)2021-01-26 00:44:42
国际呼吸杂志(2019年20期)2019-11-23 08:46:14
兽医导刊(2016年12期)2016-05-17 03:51:35
兽医导刊(2016年12期)2016-05-17 03:51:16
吉林大学学报(医学版)(2015年3期)2015-12-17 07:47:50
感染、炎症、修复(2015年2期)2015-12-10 02:37:59
医学研究杂志(2015年5期)2015-06-10 06:43:26
护士进修杂志(2015年13期)2015-03-18 11:21:45
中国当代医药(2015年9期)2015-03-01 02:02:19
祝您健康(1982年5期)1982-12-29 03:52:48
