阿司匹林及氯吡格雷双联抗血小板治疗对女性月经的影响
2015-06-01 09:43:54万继业马淑梅
实用药物与临床 2015年6期
万继业,马淑梅
阿司匹林及氯吡格雷双联抗血小板治疗对女性月经的影响
万继业,马淑梅*
目的 观察女性经皮冠状动脉介入治疗(Percutaneous coronary intervention,PCI)术后全程双联抗血小板药物阿司匹林及氯吡格雷口服治疗对月经的影响。方法 我院心内科2004年1月至2013年6月诊断为急性冠脉综合征且行冠状动脉支架植入术的住院绝经前女性患者,采用回顾性研究的方法观察其口服双联抗血小板药物治疗前及治疗后6个月、1年的月经情况,并采用PABC评分量表对患者的月经量进行定量评分。结果 绝经前女性冠状动脉支架置入术后双联抗血小板药物阿司匹林及氯吡格雷口服治疗1年的月经量较术前无明显变化。结论 绝经前女性应用双联抗血小板药物治疗1年,月经量无明显变化,是相对安全的。
阿司匹林;氯吡格雷;月经
0 引言
近年来,我国心血管疾病的发病率和死亡率呈上升趋势,女性患者(尤其是绝经前女性患者)冠心病的发病率逐年增加,服用非甾体抗炎药物阿司匹林抗血小板治疗已经成为目前临床上治疗冠心病的基本手段之一。非甾体抗炎药物能够减少月经过多女性患者的月经量已经得到许多RCTs研究证实[1-4],然而,目前对于发生急性冠脉综合征(Acute coronary syndrome,ACS)的绝经前女性患者,口服非甾体抗炎药物阿司匹林及ADP受体拮抗剂氯吡格雷双联抗血小板药物治疗对月经的影响尚不明确。本文通过回顾性调查探讨这一特定人群冠状动脉支架植入术后服用阿司匹林及氯吡格雷双联抗血小板药物1年期间月经的变化情况,探讨其对女性月经的影响,从而为临床用药提供参考。
1 资料与方法
1.1 临床资料 2004年1月至2013年6月于我院心内科住院、诊断为ACS、行冠状动脉支架植入术的绝经前女性患者,排除术后1年有妊娠计划、患有严重肝肾疾病且预计生存期不超过1年的患者,平均年龄(44±5.2)岁。术后严格遵医嘱每天口服双联抗血小板药物拜阿司匹林肠溶片100 mg及氯吡格雷片75 mg治疗。
1.2 研究方法 对于符合纳入及排除标准的患者统一建立随访档案,记录患者的住院号、民族、文化程度、家族史、吸烟史、发病年龄及住院时收缩压、舒张压、心率、血液生化、冠脉病变情况等一般基线资料;同时记录患者住院前2个月的月经周期、经期及经量情况,并采用PABC(Pictorial blood loss assessment chart)月经量评分量表对患者的月经量统一进行半定量评分[5];术后6个月、1年分别通过门诊或电话随访的方式获知患者近2个月的月经周期、经期及经量情况,亦采用PABC评分量表对患者月经量进行评分。
1.3 统计学分析 应用SPSS 13.0软件统计录入数据,采用重复测量资料的方差分析对患者术前及术后6个月、1年的月经量进行统计分析,P<0.05为差异有统计学意义。
2 结果
2.1 基线情况分析 符合纳入及排除标准的患者共27例,失访3例,有效样本数24例。汉族22例,鲜族2例;文化程度:初中以下7例,占29.2%,高中15例,占62.5%,大学2例,占8.3%;三代以内直系亲属有心脑血管疾病病史3例,占12.5%;有吸烟史2例,占8.3%;合并高血压10例,占41.7%,合并高血压及糖尿病1例,占4.2%,合并高血压及脑卒中1例,占4.2%;冠状动脉左前降支置入支架13例,左回旋支置入支架6例,右冠状动脉置入支架9例,人均置入支架1.3个。样本人群的血压、心率及血液生化等一般基线情况见表1。

表1 样本人群的基线特征
注:*使用Kolmogorov-Smirnov方法的正态性检验结果(下同)
2.2 月经情况分析
2.2.1 月经周期及经期的变化 通过电话随访获知符合条件的24例患者术前月经周期及经期较以往无明显变化,术后2例患者自觉周期较术前延长,4例患者诉经期较术前延长,其中1例患者诉月经周期及经期均较术前延长。
2.2.2 月经量的变化 使用PABC评分量表对患者冠状动脉支架植入术前及术后6个月、1年的月经量情况进行半定量评分,其基本检验统计量见表2。患者术前及术后6个月、1年的PABC评分分值均分别行Kolmogorov-Smirnov正态性检验,P均>0.1,提示样本人群术前及术后6个月、1年的PABC月经量评分分值均服从正态性分布。
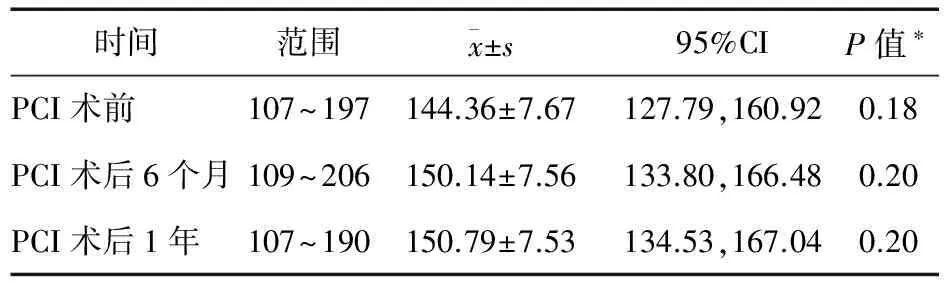
表2 PCI术前及术后6个月、1年样本人群月经量PABC积分
样本人群术前及术后6个月、1年的PABC评分分值样本Mauchly球对称检验结果:P=0.41(>0.1),符合球对称假设,使用重复测量的方差分析法分析患者口服双联抗血小板药物阿司匹林及氯吡格雷治疗前及治疗后6个月、1年月经量的变化时,无需校正自由度,其方差分析的结果显示,P=0.6(>0.1),说明月经正常女性冠状动脉支架植入术前及术后6个月、1年的月经量无明显变化。
3 讨论
阿司匹林通过不可逆地乙酰化前列腺素环氧化酶,阻止花生四烯酸转化为前列腺素,抑制血栓素A2的生成,从而间接发挥抗血小板作用。波利维在体内水解成无生物活性的药物前体,通过肝脏细胞色素P450(包括CYP3A4、CYP2C19、CYP1A2、CYP2B6)氧化成具有生物活性的物质,通过抑制ADP与血小板P2Y12受体结合,从而抑制血小板活化及血栓的形成[6]。
发生ACS的患者由于冠状动脉粥样斑块破裂,内皮下组织因子暴露,血小板激活,并介导了血管内血栓的形成[7-8],血液会在相当长的一段时间内处于高凝状态,由此引发的心脏缺血事件风险增加[9],加上冠状动脉内支架置入后,支架作为外源性异物本身亦导致血小板的过度激活。临床研究证实,双联抗血小板药物阿司匹林及氯吡格雷联合治疗能大幅度降低缺血事件[8-10],尤其与单用阿司匹林治疗相比,住院再缺血事件、再梗死、中风及再次血运重建率明显降低,主要出血事件却无明显增加[11-14],因此双联抗血小板药物治疗已经成为支架植入术后预防冠脉再狭窄及支架内血栓形成的常规治疗措施。
随着双联抗血小板药物阿司匹林及氯吡格雷的广泛应用,患者消化道出血及颅内出血的发生率也在增加。研究显示,PCI术后口服双联抗血小板药物胃肠道出血的发生率均在2%左右,高龄、既往消化溃疡病史、合并应用其他非甾体抗炎药物或抗凝药物均能增加消化道出血的发生率[15-17]。既往有消化道出血病史是服用阿司匹林和/或氯吡格雷药物后发生消化道出血的预测因子,且消化道出血与近期及远期死亡密切相关[18-23]。Shiotani等[24]认为,双联抗血小板药物治疗亦能够加重小肠的损伤。在使用阿司匹林和氯吡格雷抑制血小板活性的同时,颅内出血事件风险增加,并且部分抵消了抗血小板药物降低心血管事件风险所带来的获益[25-26]。
虽然双联抗血小板治疗对于患者消化道出血及颅内出血的影响研究较多,但对于绝经前女性发生ACS事件后,口服双联抗血小板药物后月经量的变化情况并不清楚。有报道,在月经过多的人群中发现存在子宫内膜环氧化酶及前列腺素的过度表达[27-29],前列腺素类物质通过与细胞膜G蛋白受体偶联,通过第二信使途径使细胞内cAMP浓度增加,调节基因的表达,来发挥其生物学作用[30]。尤其是前列腺素E及前列腺素F在月经期间对于调节子宫内膜的生理功能起重要作用[31-32],而非甾体抗炎药物阿司匹林能通过环氧化酶抑制前列腺素的生成,影响月经量。已经有临床研究证实,服用非甾体抗炎药物能减少月经过多女性患者的月经量[1-4],且不同种类的非甾体抗炎药物之间疗效相似。然而对于月经量正常的女性患者,非甾体抗炎药物对月经量的影响的研究甚少。
本文通过对冠脉支架植入术前未绝经女性术后1年的观察,并未观察到患者口服阿司匹林及氯吡格雷后月经量较前有所变化,提示对于月经正常的女性,发生ACS事件后,口服阿司匹林及氯吡格雷治疗对月经量影响不大,是相对安全的。
[1] Smith OP,Jabbour HN,Critchley HO.Cyclooxygenase enzyme expression and E series prostaglandin receptor signalling are enhanced in heavy menstruation[J].Hum Reprod,2007,22(5):1450-1456.
[2] Wellington K,Wagstaff AJ.Tranexamic acid:a review of its use in the management of menorrhagia[J].Drugs,2003,63(13):1417-1433.
[3] Bonnar J,Sheppard BL.Treatment of menorrhagia during menstruation:randomized controlled trial of ethamsylate,mefenamic acid,and tranexamic acid[J].BMJ,1996,313(7057):579-582.
[4] Lethaby A,Augood C,Duckitt K,et al.Nonsteroidal anti-inflammatory drugs for hevy menstrual bleeding[J].Cochrane Database of Systematic Reviews,2007,17(4):CD000400.
[5] Higham JM,O′Brien PM,Shaw RW.Assessment of menstrual blood loss using a pictorial chart[J].British Journal of Obstetrics Gynaecology,1990,97(8):734-739.
[6] Jiang X,Samant S,Lesko LJ,et al.Clinical pharmacokinetics and pharmacodynamics of clopidogrel[J].Clin Pharmacokinet,2015,54(2):147-166.
[7] Fuster V,Moreno PR,Fayad ZA,et al.Atherothrombosis and high-risk plaque:part I:evolving concepts[J].J Am Coll Cardiol,2005,46:937-954.
[8] Depta JP,Bhatt DL.Aspirin and platelet adenosine diphosphate receptor antagonists in acute coronary ayndromes and percutaneous coronary intervention:role in therapy and strategies to overcome resistance[J].Am J Cardiovasc Drugs,2008,8:91-112.
[9] Fox KA,Anderson FA Jr,Goodman SG,et al.Tine course of events in acute coronary syndromes:implications for clinical practice from the GRACE registry[J].Nature Clinical Practice Cardiovascular Medicine,2008,5:580-589.
[10]Antithrombotic Trialists′ Collaboration.Collaborative meta-analysis of randomized trials of antiplatelet therapy for prevention of death,myocardial infarction,and stroke in high risk patients[J].BMJ,2002,324:71-86.
[11]Yusuf S,Zhao F,Mehta SR,et al.Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation[J].N Engl J Med,2001,345(7):494-502.
[12]Chen ZM,Jiang LX,Chen YP,et al.Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction:randomized placebo-controlled trial[J].Lancet,2005,366(9497):1607-1621.
[13]Steinbubl SR,Berger PB,Mann JT 3rd,et al.Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention:a randomized controlled trial[J].JAMA,2002,288(19):2411-2420.
[14]Mehta SR,Yusuf S,Peters RJ,et al.Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention:the PCI-CURE study[J].Lancet,2001,358:527-533.
[15]Tanigawa T,Watanabe T,Nadatani Y,et al.Gstrointestinal bleeding after percutaneous coronary intervention[J].Digestion,2011,83(3):153-160.
[16]Delaney JA,Opatrny L,Brophy JM,et al.Drug-drug interactions between antithrombotic medications and the risk of gastrointestinal bleeding[J].CMAJ,2007,177:347-351.
[17]Hallas J,Dall M,Andries A,et al.Use of single and combined antithrombotic therapy and risk of serious upper gastrointestinal bleeding:population based case-control study[J].BMJ,2006,333:726.
[18]Alli O,Smith C,Hoffman M,et al.Incidence,predictors,and outcomes of gastrointestinal bleeding in patients on dual antiplatelet therapy with aspirin and clopidogrel[J].J Clin Gastroenterol,2011,45(5):410-414.
[19]Ng FH,Wong SY,Chang CM,et al.High incidence of clopidogrel-associated gastrointestinal bleeding in patients with previous peptic ulcer diseases[J].Aliment Pharmacol Ther,2003,18(4):443-449.
[20]Nikolsky E,Stone GW,Kirtane AJ,et al.Gastrointestinal bleeding in patients with acute coronary syndromes:Incidence,predictors,and clinical implications:analysis from the ACUITY(Acute Catheterization and Urgent Intervention Triage Strategy)trial[J].Journal of the American College of Cardiology,2009,54:1293-1302.
[21]Chin MW,Yong G,Bulsara MK,et al.Predictive and protective factors associated with upper gastrointestinal bleeding after percutaneous coronary intervention:a case-control study[J].American Journal of Gastroenterology,2007,102:2411-2416.
[22]Moscucci M,Fox KA,Cannon CP,et al.Predictors of major bleeding in acute coronary syndromes:the Global Registry of Acute Coronary Events(GRACE)[J].Eur Heart J,2003,24:1815-1823.
[23]Ko DT,Yun L,Wijeysundera HC,et al.Incidence,predictors,and prognostic implications of hospitalization for late bleeding after percutaneous coronary intervention for patients older than 65 years[J].Circulation-Cardiovascular Interventions,2010,3:140-147.
[24]Shiotani A,Honda K,Murao T,et al.Combination of low-dose apirin and thienopyridine exacerbates small bowel injury[J].Scandinavian Journal of Gastroenterology,2011,46(3):281-286.
[25]Naidech AM,Bendok BR,Garg RK,et al.Reduced platelet activity is associated with more intraventricular hemorrhage[J].Neurosurgery,2009,65(4):684-688.
[26]Cattaneo M.Haemorrhagic stroke during anti-platelet therapy[J].Eur J Anaesthesiol,2008,42(Suppl):12-15.
[27]Smith OP,Jabbour HN,Critchley HO.Cyclooxygenase enzyme expression and E series prostaglandin receptor signaling are enhanced in heavy menstruation[J].Hum Reprod,2007,22(5):1450-1456.
[28]Maybin JA,Hirani N,Broun P,et al.The regulation of vascular endothelial growth factor by hypoxia and prostaglandin F during human endometrial repair[J].J Clin Endocrinol Metab,2011,96(8):2475-2483.
[29]Sales KJ,Jabbour HN.Cyclooxygenase enzymes and prostaglandins in pathology of the endometrium[J].Reproductionm,2003,126(5):559-567.
[30]Coleman RA,Smith WL,Narumiya S.International Union of Pharmacology classification of prostanoid receptors properties,distribution,and structure of the receptors and their subtypes[J].Pharmacol Rev,1994,46:205-229.
[31]Lumsden MA,Kelly RW,Baird DT.Primary dysmenorrhoea:the importance of both prostaglandins E2 and F2 alpha[J].British Journal of Obstetrics and Gynaecology,1983,90(12):1135-1140.
[32]Baird DT,Cameron ST,Critchley HO,et al.Prostaglandins and menstruation[J].European Journal of Obstetrics & Gynecology Reproductive Biology,1996,70(1):15-17.
Influence of dual anti-platelet therapy of asprin and clopidogrel on menstrual changes
WAN Ji-ye,MA Shu-mei*
(Department of Cardiology,Shengjing Hospital of China Medical University,Shenyang 110004,China)
Objective To observe the influence of dual anti-platelet therapy of aspirin and clopidogrel on the menstruation changes of patients after percutaneous coronary intervention.Methods Twenty-four premenopausal female patients who was diagnosed as ACS(Acute coronary syndrome)and lined of coronary artery stent implantation in our hospital from January 2004 to June 2013 were chosen,all the patients were given dural anti-platelet therapy of aspirin and clopidogrel.The menstruation situation before treatment and at 0.5,1 year after treatment were observed by a retrospective method,and the amount of menstruation was assessed by PABC(pictorial blood loss assessment chart).Results No significant difference was observed in the amount of menstruation in premenopausal female patients before surgery and after one year dual anti-platelet therapy.Conclusion The dual anti-platelet therapy for the premenopausal female patients(lasting one year)has no obvious influence on the amount of menstruation,it is relatively safe.
Aspirin;Clopidogrel;Menstruation
2014-09-24
中国医科大学附属盛京医院心内科,沈阳 110004
*通信作者
10.14053/j.cnki.ppcr.201506013
猜你喜欢
中华养生保健(2020年7期)2020-11-16 01:13:34
金色少年(奇趣科普)(2017年9期)2017-12-04 01:36:10
中国医药指南(2017年3期)2017-11-13 02:56:22
中央社会主义学院学报(2017年1期)2017-04-16 05:34:03
上海金属(2016年1期)2016-11-23 05:17:43
中国卫生标准管理(2015年18期)2016-01-20 09:27:09
新疆钢铁(2015年3期)2015-11-08 01:59:21
城市地理(2015年24期)2015-08-15 00:52:57
中国工程咨询(2015年6期)2015-02-16 05:33:34
中国卫生标准管理(2015年15期)2015-01-26 20:32:38