
Surgicaloutcomes ofmini-open Wiltse approach and conventional open approach in patients with single-segment thoracolumbar fractures withoutneurologic injury
2015-01-10 06:16:32HaijunLiLeiYangHaoXieLipengYuHaifengWeiXiaojianCao
Haijun Li,Lei Yang,Hao Xie,Lipeng Yu,Haifeng Wei,Xiaojian Cao,✉
1Department of Orthopaedics,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China;
2Department of Orthopaedics,the Second Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu,China;
3Department of Radiology,Taizhou Peopleˊs Hospital affiliated to Nantong University,Taizhou,Jiangsu,China.
Surgicaloutcomes ofmini-open Wiltse approach and conventional open approach in patients with single-segment thoracolumbar fractures withoutneurologic injury
Haijun Li1,Lei Yang1,Hao Xie2,Lipeng Yu1,Haifeng Wei3,Xiaojian Cao1,✉
1Department of Orthopaedics,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China;
2Department of Orthopaedics,the Second Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu,China;
3Department of Radiology,Taizhou Peopleˊs Hospital affiliated to Nantong University,Taizhou,Jiangsu,China.
Thisstudy aimed to introduce a novelmini-open pedicle screw fixation technique via Wiltse approach,and compared itwith the traditionalposterior open method.A totalof 72 cases of single-segmentthoracolumbarfractures withoutneurologic injury underwentpedicle screw fixation via two differentapproaches.Among them,37 patients were treated using posterioropen surgery,and 35 patients received mini-open operation via Wiltse approach.Crew placement accuracy rate,operative time,blood loss,postoperative drainage,postoperative hospitalization time, radiation exposure time,postoperative improvementin R value,Cobbˊs angle and visualanalog scale(VAS)scores of the two methods were compared.There were no significant differences in the accuracy rate of pedicle screw placement,radiation exposure and postoperative R value and Cobbˊs angle improvementbetween the two groups. However,the mini-open method had obvious advantages over the conventional open method in operative time, blood loss,postoperative drainage,postoperative hospitalization time,and postoperative improvementin VAS. The mini-open pedicle screw technique could be applied in treatment of single-segment thoracolumbar fracture without neurologic injury and had advantages of less tissue trauma,short operative and rehabilitative time on the premise of guaranteed accuracy rate and no increased radiation exposure.
thoracolumbar fracture,pedicle screw,Mini-open,Wiltse approach,minimally invasive
Introduction
The thoracolumbar spine is one of the most common areasforspinalfractures[1,2].Fortreatmentofcaseswith neurological injuries,internal fixation after decompression has been widely accepted.The choice of treatment in the absence of a neurological deficit depends on the Thoracolumbar Injury Classification and Severity Score(TLICS)scores[3,4].However,for patients with thoracolumbar biomechanical changes as a result of a certain degree of spinal deformity, low back pain and even neurological symptoms may occur over time,which may seriously jeopardize their work and daily life.Therefore,some scholars advocate early surgical treatment,even for stable thoracolumbar fractures(TLICS:score≤3)[5,6].
In the conventional open posterior pedicle screw fixation with posterior midline incision,detachmentof the paraspinalmuscles may be required to reduce softtissue ischemia,alleviate dysfunction ofthe paraspinal muscles and relieve chronic pain[7-10].In addition,this open approach may be disadvantaged by prolonged operative time,increased intraoperative bleeding and delayed functional rehabilitation[11].All these problems appear to defeatour originalintention of surgical treatment.With the advantage of no paraspinal muscle stripping,the percutaneous pedicle screw placementtechnique is attracting increasing attention as itbrings a multitude of benefits including less bleeding, lower infection risk,lower incidence of postoperative pain,shorter rehabilitative time and reduced hospitalization time[12-20].It is also worth mentioning that the incidences of both postoperative intractable low back pain and muscle atrophy are also significantly reduced[12,16,21-24].
Although percutaneous pedicle screw fixation is a mature technique,itstillrequiresspecialized equipments and long learning curve[25]before implementation.High incidence ofscrew malposition[26,27]and large doses of radiation exposure[28,29]have caused a sluggish evolution.
In this study,we described a novelmini-open pedicle screw fixation technique via Wiltse approach forsinglesegmentthoracolumbar fractures and compared the reliability and safety ofthis approach with the conventionalposterioropen method.
Patients and methods
Patients
The clinical data of 72 cases of single-segment thoracolumbarfractures withoutneurologic injury were reviewed.Among them,35 cases(21 males and 14 females)from the mini-open group underwentpedicle screw internalfixation via Wiltse approach.Thirty-seven cases(23 males and 14 females)received conventional open surgeries via the posterior midline approach.The inclusion criteria were as follows:patients with singlesegmentthoracolumbar vertebralfractures classified as A1,A2,A3 or B1 type according to the AO classification,aged from 16 to 65 years,patients had fresh fracturesand were treated surgically within 10 daysafter the injury,TLICS score≥4 and load-sharing score<7. The exclusion criteria were as follows:patients with neurologicalinjury,spinal anatomical variations or vertebraldeformity,a history ofneurologicaldysfunction or mentalillness,significantsurgicalcontraindications, osteoporosis[dual-energy X-ray absorptiometry(DEXA) examination,T value≤-2.5],and patients who refused to sign informed consent.
Surgical methods
For the conventional posterior open approach,we firstly performed a posterior midline incision at the targetsegmentand striped the paraspinalmuscle along the spinous process and the vertebrallamina.Then,the facet joints and roots of the transverse process were exposed by an automatic retractor.The entry pointwas determined based on anatomicallandmarks according to the AO method.
Forpedicle screw internalfixation via Wiltse approach, body positioning and anesthesia were performed the same asforpatientsreceiving the conventionalposterior open approach.Manipulative reduction was performed to correctthe kyphosis ofthe fractured vertebralbody before routine sterilization.Positions offoursmallincisionswere accurately determined by thelocatorand C-arm (Fig.1A).Then,dissection wasperformed tillthe outer edge of the facet joints was reached through the intermuscularplane between the multifidus and the longissimus muscles after four 1.5-2.0-centimeter-long incisions were made(Fig.1B).With the help of mini-retractor designed by ourselves,the pedicle entry point was exposed clearly(Fig.2).The determination ofthe entry pointwas also based on the anatomicallandmarks usingthe same method as the conventionalopen group.The guide wire was inserted perpendicular to the corresponding supraspinalligament[30],and then C-arm was performed to check whether the guide wire was in the pedicle before pedicle screw placement.If the guide wire was in a satisfactory position,the pedicle screw could be inserted;otherwise,position ofthe guide wire should be adjusted.Likewise,afterthe procedure ofrod installation and distraction for restoration,positions of pedicle screwsand heightofthe fractured vertebraewere confirmed using C-arm again.
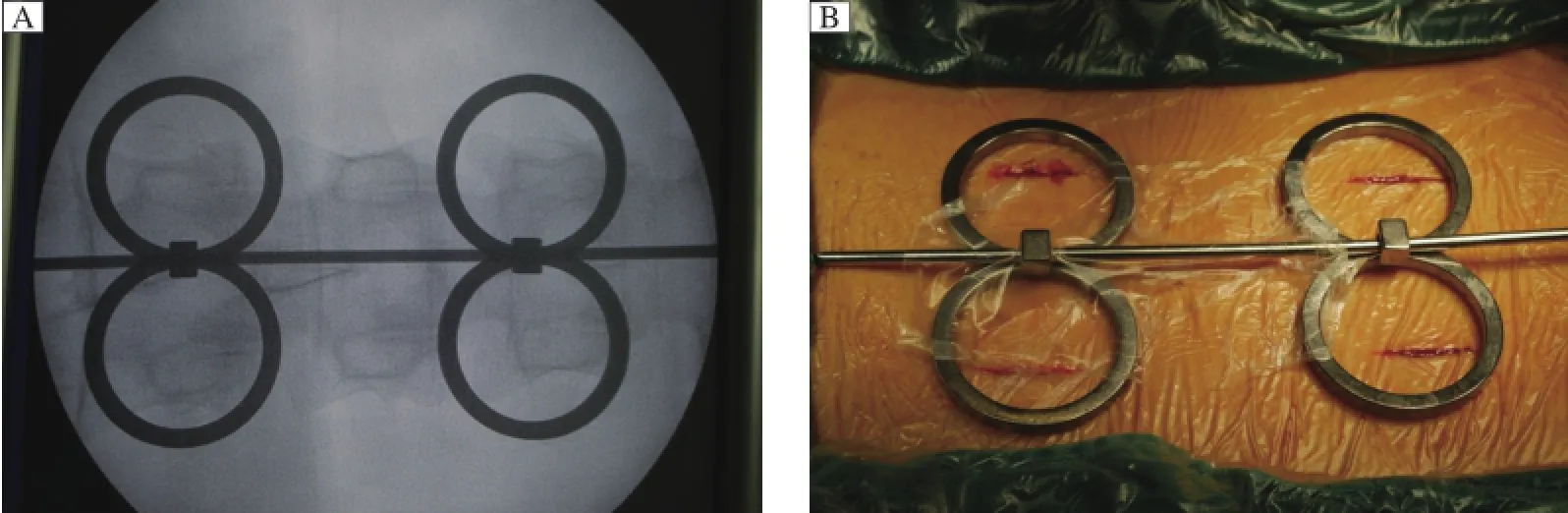
Fig.1 Location of four small incisions.A:Four small incisions can be accurately determined by the locator and C-arm.B:Four 1.5-2.0-centimeter-long incisions are made with reference to the locator.
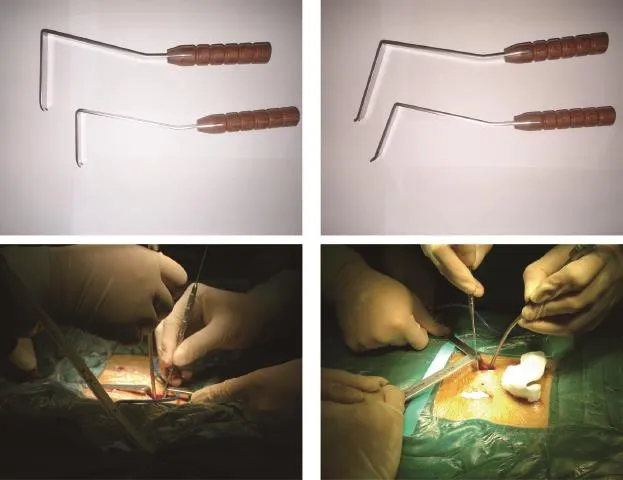
Fig.2Self-designed mini-retractor.With the help of the mini-retractor,the pedicle entry point is exposed clearly and the determination of the entry point is based on the anatomical landmarks using the same method as in the conventional open group.
Study parameters
The study parameters included operative time from the firstskin incision to skin suture,estimated blood loss,postoperative drainage,postoperative hospital stays,X-ray exposure time,which was automatically accumulated by C-arm machine,R value,Cobbˊs angle, visualanalog scale(VAS)scores,postoperative complications,and accuracy rate of screws.Blood loss was carefully measured by weighing the sponges and determining the volume of shed blood in the suction bottle.The volume of postoperative drainage was estimated by weighing wound dressings in the mini-open group as drainage tube placement was notrequired and was estimated by blood volume in the drainage bag and wound dressings in the open group.Hospital stay was calculated from the first postoperative day to the discharge day.R value was determined by the following formula:
The mean height of the fractured vertebral body/the mean height of upper and lower adjacent vertebral bodies×100%
Cobbˊs angle was delineated on lateral radiographs as the angle of the verticalline to the upper endplate of the upper adjacent vertebralbody and lower endplate of the lower adjacent vertebralbody.VAS was evaluated preoperatively,three days and one week postoperatively.Positions of pedicle screws were assessed by a single-blinded,independent and boardcertified spine surgeon according to postoperative CT scans within one week after surgery.Screw which was extrapedicular or breached the front edge of the vertebral body,inferio r or superior endplate was regarded as a failure.
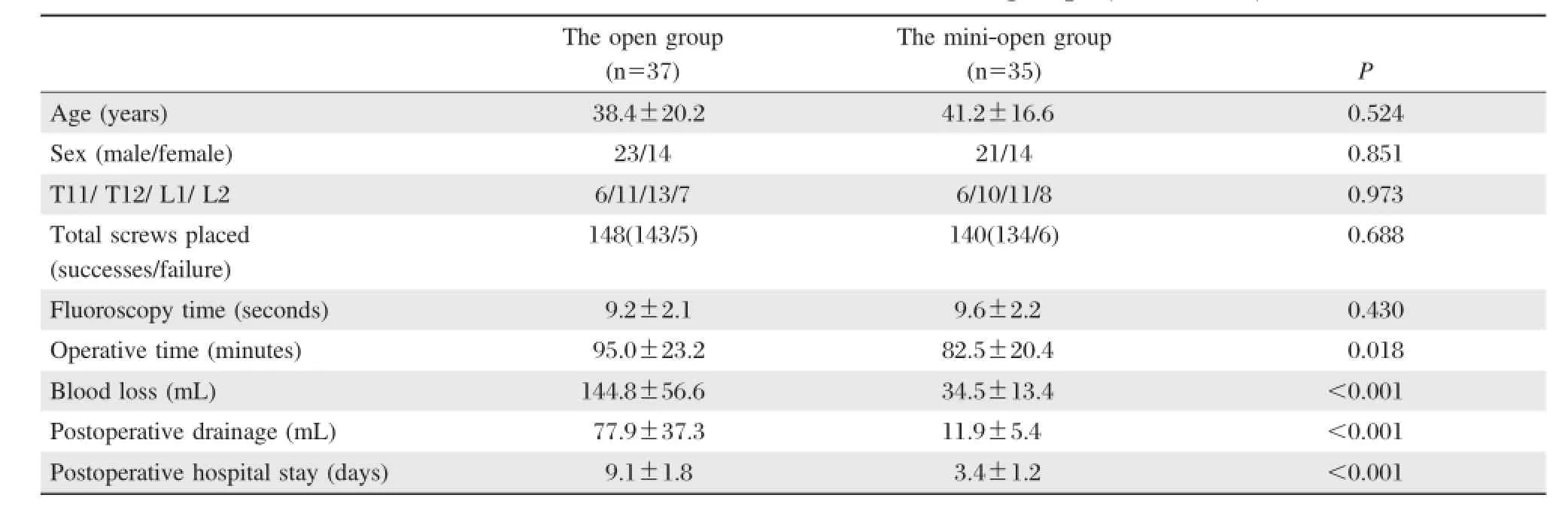
Table 1 Patient data and clinical outcomes in two groups(mean±SD)
Statistical analysis
All continuous data were presented as mean± standard deviation(SD)and allcategoricaldata as percentages or numbers.Statisticalanalyses for comparisons between groups were performed using the unpaired Studentˊs t-test,Χ2 test,or non-parametric Kruskal-Wallistest.P<0.05 wasconsidered statistically significant.Statisticalanalysis was done using SPSS 20.0(SPSS,Chicago,IL,USA).
Results
Accuracy rate of pedicle screw placement
Among all the pedicle screws,both groups required no intraoperative adjustment.No complications such as spinal cord,nerve root or blood vessel injuries occurred.In the open group,according to postoperative CT image,two screws broke through the medial cortex of the pedicle;two broke through the lateral cortex; one broke through the front cortex of the vertebral body.No screw broke through vertebral endplates. The accuracy rate of pedicle screw placement was 96.6%.In the mini-open group:five pedicle screws broke through the lateral cortex of pedicle;one broke through the frontcortex ofthe vertebralbody;no screw broke through the vertebralendplate.The accuracy rate was 95.7%.There was no significantdifference in the accuracy rate of pedicle screw placement between the two groups(Table 1).
Surgical outcomes
There were significantdifferences in operative time (P=0.018),blood loss(P<0.001),postoperative drainage(P<0.001)and postoperative hospitalization time(P<0.001)between the two groups(Table 1). The results showed that the mini-open method had obvious advantages in these aspects compared with the conventionalopen method.There were no significantdifferences in R value and Cobbˊs angle between the two groups before and after surgery(P>0.05, Table 2).But in either group,operation brought significantimprovementcompared with preoperative data (P<0.001,Table 3).No significantdifferences were found in improvement of R value and Cobbˊs angle between the two groups(P>0.05,Table 2).
Preoperative VAS for the two groups showed no significant difference(P>0.05).In general,VAS forboth groups showed significantimprovementcompared with preoperative value(P<0.01).However, the degree of this improvement between the two groups was not the same.The results showed thatthe mini-open method had greater improvement in VAS scores at postoperative day 3 and 7(P<0.01)than the open approach(Table 4).
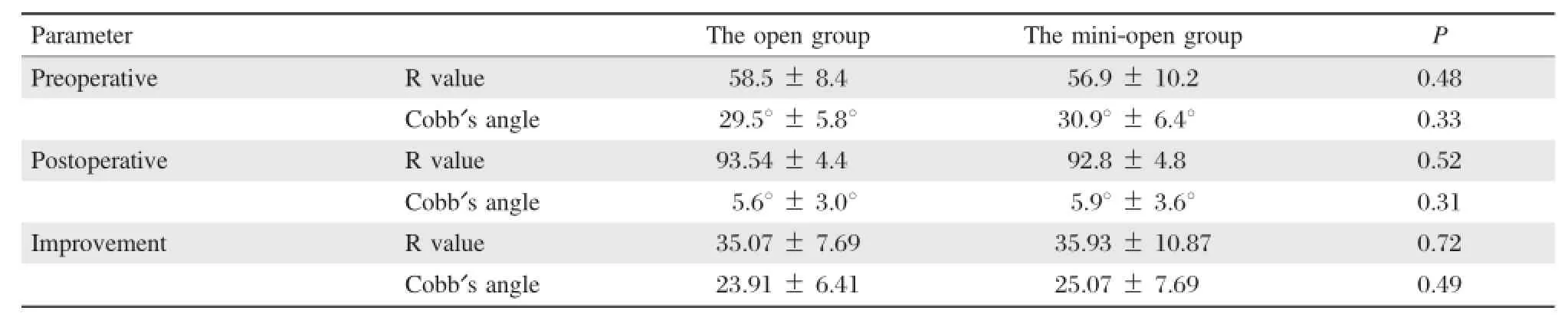
Table 2 Comparison of R value and Cobbˊs angle between the two groups(mean±SD)

Table3 Comparison between preoperative and postoperative Rvalue and Cobbˊs angle in the two groups(mean±SD)
Discussion
In 1968,Wiltse[31]first described the paraspinal sacrospinalis-splitting approach between the multifidus and the longissimus which was associated with less bleeding and tissue dissection compared with the single midline incision approach[32-34].Drawbacks including extensive stripping ofthe paraspinalmuscle, electrical-burn damage from electricknife and prolonged mechanicalcompression by automatic retractor could be effectively avoided in the procedure of entry point exposure through the mini-open method via Wiltse approach.The mini-open approach had rapid recovery with slight pain and markedly shorter hospitalization time compared with the traditionalopen approach.All patients from the mini-open group were mobile with the protection of the waistbrace 24 hours aftersurgery and discharged afteran average of3.4 days postoperatively.However,for those patients who underwent the open surgery,the drainage tubeswere removed on postoperative day 2,the mean postoperative hospitalstay was 9.1 days,and activity was permitted atleasttwo weeks aftersurgery.
The conventionalopen method had advantage over the mini-open technique in exposure of pedicle screw entry point based on clear anatomical landmarks. However,the operation time in the open group was prolonged,which may be due to more soft tissue dissection and skin suture.Smooth surgicalprocedure of the mini-open group was another important reason. Foursmallincisionswere rapidly located by the locator with few X-ray exposure(Fig.1A);Two separated blunthook teeth of the retractor which were confirmed suitable for varied local bone structures played an important role in preventing muscles slipping away (Fig.2).Aimed by the self-designed retractor,the entry point could also be easily exposed and determined based on the anatomicallandmarks identical to the open approach.With intactcoverage of the sarcolemma,muscle creep could be effectively avoided in muscle dissection if only the approach was strictly along the muscle gap.Especially for segments of L4 and L5,muscle gaps were absolutely clear and the sarcolemmas were relatively hypertrophic[35].
Radiation exposure in pedicle screw placementhas always been the focus of attention,and the risk of long-term low-doses X-ray remains unclear[29].In our research,determination of pedicle screw entry point in the two groups both required C-arm assistance. For the reason given above,there was no obvious difference in X-ray exposure(9.2±2.1 seconds for the open group vs.9.6±2.2 seconds forthe mini-open group)between the two groups.Namely,the mini-open approach did not increase radiation exposure in the operation.
The mini-open technique is similar to the open metho d in restoration o f vertebral body height, improvement of Cobbˊs angle and accuracy rate of screw placement.There were no cases of spinalcord, nerve orvesselinjury in both groups.Study limitations included lack of long-term follow-up in such as postoperative loss ofthe vertebralheight.However,the only distinction between the two groups was the surgical approach.In aspects of fixation method and pedicle screw type,the two techniques were the same. Therefore,we can infer thatthe mini-open approach was similar to the open method in postoperative loss ofvertebralheightin long-term follow-up.
The biggest current limitation of the mini-open approach is that it is not suitable for posterior lami-nectomy and posterolateral fusion.Therefore,the inclusion criteria was strictly limited to cases of single segmentthoracolumbarvertebralfractures classified as A1,A2,A3 or B1 type according to AO classification. Additionally,the patientˊs load-sharing score(spinal load scoring system)must be less than seven points to ensure the security of only posterior fixation for thoracolumbar fractures.Narrow indication is the drawback of this technique.

Table 4 VAS scores of the two groups(mean±SD)
In conclusion,compared with the traditional open posterior surgery,the mini-open surgery via Wiltse approach has the following advantages on the premise of no increased radiation exposure,less bleeding, shorter operative time,less postoperative pain and tissue trauma,and shorter rehabilitative and hospitalization time.Therefore,itis reliable in treating cases of thoracolumbarfractures withoutneurologicaldamage.
Acknowledgement
This work was supported by the National Natural Science Foundation of China(Grant No.30973058, 81171694,and 81371968);the Program for Development of Innovative Research Team in the First Affiliated Hospital of NJMU(No.IRT-015),and A Project Funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions. This study was approved by Ethical Committee of the First Affiliated Hospital of Nanjing Medical University.The clinicltrails.gov number is‘‘ChiCTROCC-10001133’’,and written informed consent were obtained from allpatients.
Reference
[1]Gertzbein SD.Spine update.Classification of thoracic and lumbar fractures.Spine(Phila Pa 1976)1994;19(5):626-628.
[2]Magerl F,Aebi M,Gertzbein SD,etal.A comprehensive classification of thoracic and lumbar injuries.Eur Spine J 1994;3(4):184-201.
[3]Vaccaro AR,Zeiller SC,Hulbert RJ,et al.The thoracolumbar injury severity score:a proposed treatment algorithm.J Spinal Disord Tech 2005;18(3):209-215.
[4]Vaccaro AR,Lehman RA,Jr.,Hurlbert RJ,et al.A new classification of thoracolumbar injuries:the importance of injury morphology,the integrity of the posterior ligamentous complex,and neurologic status.Spine(Phila Pa 1976)2005;30(20):2325-2333.
[5]Domenicucci M,Preite R,RamieriA,etal.Thoracolumbar fractures without neurosurgical involvement:surgical or conservative treatment?J Neurosurg Sci1996;40(1):1-10.
[6]Siebenga J,Leferink VJ,Segers MJ,et al.Treatment of traumatic thoracolumbar spine fractures:a multicenter prospective randomized study of operative versus nonsurgicaltreatment.Spine(Phila Pa 1976)2006;31(25):2881-2890.
[7]Kawaguchi Y,Yabuki S,Styf J,et al.Back muscle injury after posterior lumbar spine surgery.Topographic evaluation of intramuscular pressure and blood flow in the porcine back muscle during surgery.Spine(Phila Pa 1976) 1996;21(22):2683-2688.
[8]KawaguchiY,MatsuiH,Tsuji H.Back muscle injury after posteriorlumbarspine surgery.Ahistologic and enzymatic analysis.Spine(Phila Pa 1976)1996;21(8):941-944.
[9]Sihvonen T,Herno A,Paljarvi L,et al.Localdenervation atrophy of paraspinalmuscles in postoperative failed back syndrome.Spine(Phila Pa 1976)1993;18(5):575-581.
[10]Styf JR,Willen J.The effects of external compression by three different retractors on pressure in the erector spine muscles during and after posterior lumbar spine surgery in humans.Spine(Phila Pa 1976)1998;23(3): 354-358.
[11]Kim DH,Vaccaro AR.Osteoporotic compression fractures of the spine;current options and considerations for treatment.Spine J 2006;6(5):479-487.
[12]Kim DY,Lee SH,Chung SK,etal.Comparison of multifidus muscle atrophy and trunk extension muscle strength: percutaneous versus open pedicle screw fixation.Spine (Phila Pa 1976)2005;30(1):123-129.
[13]CourtC,Vincent C.Percutaneous fixation of thoracolumbar fractures:current concepts.Orthop Traumatol Surg Res 2012;98(8):900-909.
[14]Cox JB,Yang M,Jacob RP,et al.Temporary percutaneous pedicle screw fixation for treatmentof thoracolumbar injuries in young adults.J Neurol Surg A Cent Eur Neurosurg 2013;74(1):7-11.
[15]Ma YQ,Li XL,Dong J,et al.[Comparison of percutaneous versus open monosegment instrumentation in the treatment of incomplete thoracolumbar burst fracture]. Zhonghua Yi Xue Za Zhi 2012;92(13):904-908.
[16]Song HP,Lu JW,Liu H,et al.Case-control studies between two methods of minimally invasive surgery and traditional open operation for thoracolumbar fractures. Zhongguo Gu Shang 2012;25(4):313-316.(in Chinese)
[17]De Iure F,Cappuccio M,Paderni S,etal.Minimal invasive percutaneous fixation of thoracic and lumbar spine fractures.Minim Invasive Surg 2012;2012:141032.
[18]Palmisani M,Gasbarrini A,Brodano GB,etal.Minimally invasive percutaneous fixation in the treatmentof thoracic and lumbarspine fractures.Eur Spine J 2009;18(Suppl1): 71-74.
[19]Yang WE,Ng ZX,Koh KM,et al.Percutaneous pedicle screw fixation for thoracolumbar burst fracture:a Singapore experience.Singapore Med J 2012;53(9):577-581.
[20]Fang LM,Zhang YJ,Zhang J,et al.Minimally invasive percutaneous pedicle screw fixation for the treatment of thoracolumbar fractures and posterior ligamentous complex injuries.Beijing Da Xue Xue Bao 2012;44(6):851-854.(in Chinese)
[21]Zhang ZC,Sun TS,Liu Z,etal.[Minimally invasive percutanuous cannulated pedicle screw system fixation for the treatmentof thoracolumbarflexion-distraction fracture without neurologic impairment].Zhongguo Gu Shang 2011;24(10):802-805.(in Chinese)
[22]Rampersaud YR,Annand N,Dekutoski MB.Use of minimally invasive surgicaltechniques in the management ofthoracolumbartrauma:currentconcepts.Spine(Phila Pa 1976)2006;31(11 Suppl):S96-102;discussion S104.
[23]Chen Z,Zhao JQ,Fu JW,etal.Modified minimally invasive percutaneous pedicle screws osteosynthesis for the treatment o f thoracolumbar fracture without neural impairment.Zhonghua Yi Xue Za Zhi 2010;90(21): 1491-1493.(in Chinese)
[24]Luo P,Xu LF,Ni WF,etal.Therapeutic effects and complications of percutaneous pedicle screw fixation for thoracolumbar fractures.Zhonghua Wai Ke Za Zhi 2011; 49(2):130-134.(in Chinese)
[25]Garfin SR,Fardon DF.Emerging technologies in spine surgery.Spine J 2002;2(20):1-4.
[26]Ringel F,Stoffel M,Stuer C,et al.Minimally invasive transmuscular pedicle screw fixation of the thoracic and lumbar spine.Neurosurgery 2006;59(4 Suppl2):ONS361-366;discussion ONS366-367.
[27]Schizas C,Michel J,Kosmopoulos V,et al.Computer tomography assessmentof pedicle screw insertion in percutaneous posterior transpedicular stabilization.Eur Spine J 2007;16(5):613-617.
[28]Perisinakis K,Theocharopoulos N,Damilakis J,et al. Estimation of patient dose and associated radiogenic risks from fluoroscopically guided pedicle screw insertion. Spine(Phila Pa 1976)2004;29(14):1555-1560.
[29]Rampersaud YR,Foley KT,Shen AC,et al.Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion.Spine(Phila Pa 1976) 2000;25(20):2637-2645.
[30]Li J,Zhao H,Xie H,etal.A new free-hand pedicle screw placement technique with reference to the supraspinal ligament.J Biomed Res 2014;28(1):64-70.
[31]Wiltse LL,Bateman JG,Hutchinson RH,etal.The paraspinal sacrospinalis-splitting approach to the lumbar spine.J Bone Joint Surg Am 1968;50(5):919-926.
[32]Wiltse LL,Spencer CW.New uses and refinements of the paraspinal approach to the lumbar spine.Spine(Phila Pa 1976)1988;13(6):696-706.
[33]Olivier E,Beldame J,Ould Slimane M,etal.Comparison between one midline cutaneous incision and two lateral incisions in the lumbar paraspinal approach by Wiltse:a cadaver study.Surg Radiol Anat 2006;28(5):494-497.
[34]Wiltse LL.The paraspinalsacrospinalis-splitting approach to the lumbar spine.Clin Orthop Relat Res 1973;(91):48-57.
[35]Vialle R,Wicart P,Drain O,et al.The Wiltse paraspinal approach to the lumbarspine revisited:an anatomic study. Clin Orthop Relat Res 2006;445:175-180.
✉Corresponding author:Prof.Xiaojian Cao,Department of Orthopaedics,the First Affiliated Hospital of Nanjing Medical University,300 Guangzhou Road,Nanjing,Jiangsu 210029,China, Tel/Fax:86-013002505801/86-25-83724440,E-mail:xiaojiancao@gmail.com.
Received 01 June 2014,Revised 27 Octorber 2014,Accepted 19 December 2014,Epub 16 January 2015
The authors reported no conflict of interests.
©2015 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.29.20140083
 THE JOURNAL OF BIOMEDICAL RESEARCH2015年1期
THE JOURNAL OF BIOMEDICAL RESEARCH2015年1期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Ventricular tachycardia ablation and substrate modification in ICD patients with electrical storm
- Induced pluripotentstem cells are induced pluripotentstem cell-like cells
- HLA antigens and anti-sperm antibody production in Iranian vasectomized men
- Unruptured pregnancy in a noncommunicating rudimentary horn at 37 weeks with a live fetus:a case report
- Portalvein arterialization promotes liver regeneration after extended partialhepatectomy in a rat model
- Prevalence ofenteric pathogen-associated community gastroenteritis among kindergarten children in Gaza