
三维伪连续动脉自旋标记灌注成像与正电子发射计算机断层显像在脑部病变诊断中的比较
2014-08-09 03:24陈志晔关志伟于生元
中国医学科学院学报 2014年4期
陈志晔,关志伟,于生元,马 林
中国人民解放军总医院 1放射科 2核医学科 3神经内科,北京100853
动脉自旋标记 (arterial spin labeling,ASL)序列是一个非对比剂增强的脑灌注成像技术,可以用来活体定量测量脑部灌注状态,具有较好的重复性及再现性[1-3]。目前,ASL在临床具有较为广泛的适用性,比如脑梗死后脑灌注状态的评估、脑肿瘤的灌注评估、已经认知功能障碍疾病的脑灌注等。而当前临床常用的ASL流动敏感替代反转恢复序列存在的不足为扫描范围小、分辨率较差、二维扫描。为此,GE公司开展了3D伪连续快速自旋回波动脉自旋标记 (3D pseudo-continuous arterial spin labeling,3D-pCASL)序列,此序列可以进行脑灌注的三维容积采集,分辨率较高,可以覆盖全脑扫描。正电子发射计算机断层摄影 (positron emission tomography-computed tomography,PET/CT)是目前临床常用的评估病变代谢水平的技术,本研究对脑部病变进行3D-pCASL及PET/CT扫描,以评估3D-pCASL及PET/CT在脑部病变诊断中的一致性。
对象和方法
对象 选取中国人民解放军总医院脑部病变住院患者7例,其中肿瘤性病变4例、脑脓肿1例、脱髓鞘1例、脑白质病变1例。所有受试者均为右利手,既往体健。入选标准:无磁共振检查禁忌证、肾功能正常。排除标准:颅脑外伤、脑部器质性病变、精神类疾病史、近期服用过精神类药物或激素。受试者在扫描前1 h内禁止剧烈运动和引用含咖啡因类饮料。
磁共振成像数据采集及分析 所有磁共振成像(magnetic resonance imaging,MRI)数据均采用 GE DISCOVERY MR 750磁共振扫描仪进行成像,采集线圈采用8通道颅脑线圈。扫描序列包括常规T1、T2加权成像,扩散加权成像 (diffusion weighted imaging,DWI),T2液体衰减反转恢复成像,动态磁敏感对比剂增强灌注成像 (dynamic susceptibility contrast-enhanced perfusion weighted imaging,DSC-PWI)及对比剂增强扫描;3D ASL采集参数为重复时间/回波时间 =5 128/15.9 ms,翻转角=111o,视野=20 cm×20 cm,矩阵=1 024×8(螺旋采集),层厚=3.0 mm,标记时间2.0 s。所有患者均接受PET检查。
数据处理主要基于GE ADW4.5工作站及matlab(V7.6)[4-9],生成脑血流 (cerebral blood flow,CBF)图像。
PET数据采集及图像分析 4例患者静脉注射氟代脱氧葡萄糖 (18F-fluorodeoxyglucose,FDG)296~370 MBq,1 h后行PET/CT显像,PET/CT发射断层采集时间为5 min;3例患者静脉注射蛋氨酸 (11C-methionine,MET)555~740 MBq,15 min后行 PET/CT显像,PET/CT发射断层采集时间为6 min。使用西门子64 PET/CT,PET/CT图像矩阵为336×336,采用TrueX方法进行PET/CT图像重建。在病变部位勾划感兴趣区,测量最大标准摄取值 (maximal standard uptake value,SUVmax)。同样的方法在对侧正常组织勾划感兴趣区,测量SUVmax值。
结 果
代谢性疾病3D-pCASL与PET/CT比较 女性患者,38岁,记忆力进行性减退5个月,临床诊断为肾上腺脑白质营养不良。MRI提示双侧额叶病变,呈明显强化 (图1A),DSC-PWI扫描病变与周围组织无强化组织比较呈高灌注 (图1B、1C),3D-pCASL扫描呈高灌注 (图1D),MET-PET/CT呈高代谢 (图1E)。
感染性疾病3D-pCASL与PET/CT比较 男性患者,29岁,头痛3个月,加重伴右侧肢体无力6 d,临床诊断为脑脓肿。MRI提示左侧额叶病变,呈明显强化 (图2A),DWI呈显著高信号 (图2B),DSCPWI病变呈低灌注 (图2C、2D),3D-pCASL呈低灌注 (图2E),而FDG-PET/CT显像呈高代谢 (图2F)。
炎性病变3D-pCASL与PET/CT比较 男性患者,54岁,左手麻木,乏力,间断头痛26 d,临床诊断炎性脱髓鞘。MRI提示病变位于右侧侧脑室后角旁,呈长T2信号影 (图3A、3G),部分病变内可见斑片状强化 (图3B、3H),DSC-PWI显示病变强化,病变呈高灌注 (图3C、3D、3I、3J),3D-pCASL显示病变呈高灌注 (图3E、3K),MET-PET/CT成像显示病变呈高代谢 (图3F、3L)。
肿瘤性病变3D-pCASL与PET/CT比较 共纳入4例肿瘤患者,其中包括胶质母细胞瘤1例 (图4)、非霍奇金氏淋巴瘤1例 (图5)、间变型星形细胞瘤1例(图6)、低级别胶质瘤1例 (图7),4例患者病变的灌注状态与代谢状态均存在一致性,胶质母细胞瘤、非霍奇金氏淋巴瘤和间变型星形细胞瘤患者3D-pCASL成像均为高灌注,PET/CT成像均为高代谢。低级别胶质瘤患者3D-pCASL成像为低灌注,PET/CT成像为低代谢。
CBF和SUVmax定量分析结果 定量测量结果显示各组病变区CBF值与SUVmax值的大小变化具有一致性 (表1)。
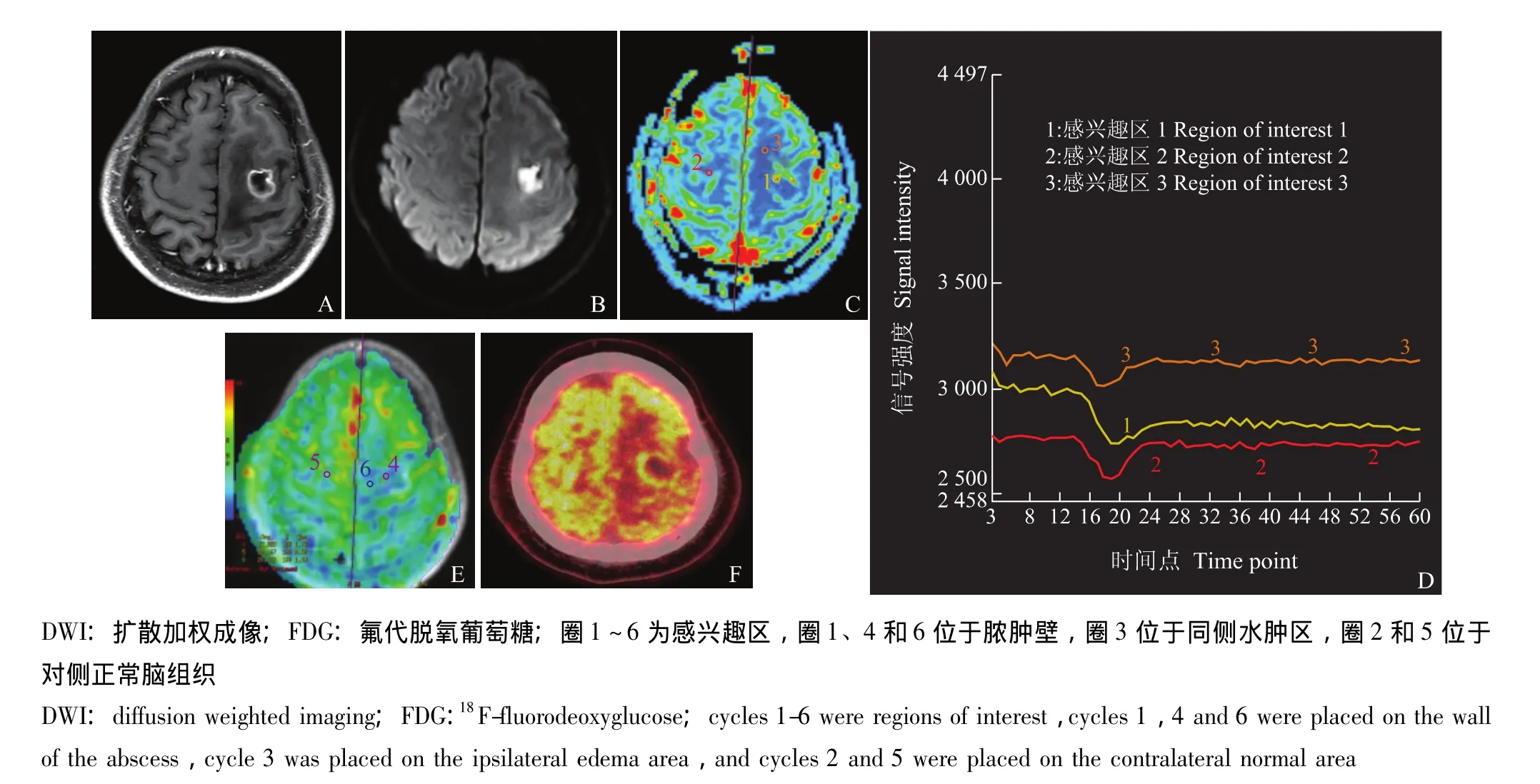
图2 男性,29岁,头痛3 d,无发热,临床诊断为脑脓肿,MRI表现为环形强化 (A),DWI为高信号 (B),DSC-PWI提示脓肿壁为低灌注 (C、D),3D-pCASL脓肿壁为低灌注 (E),FDG-PET提示脓肿壁为高代谢 (F)Fig 2 A 29-year-old male patient who had suffered from headache for 3 days was diagnosed as brain abscess,MRI showed ring-like enhancement(A),hyperintensity on DWI(B),hypoperfusion on DSC-PWI(C and D),3D-pCASL demonstrates hypoperfusion(E)and FDGPET/CT shows hypermetabolism(F)
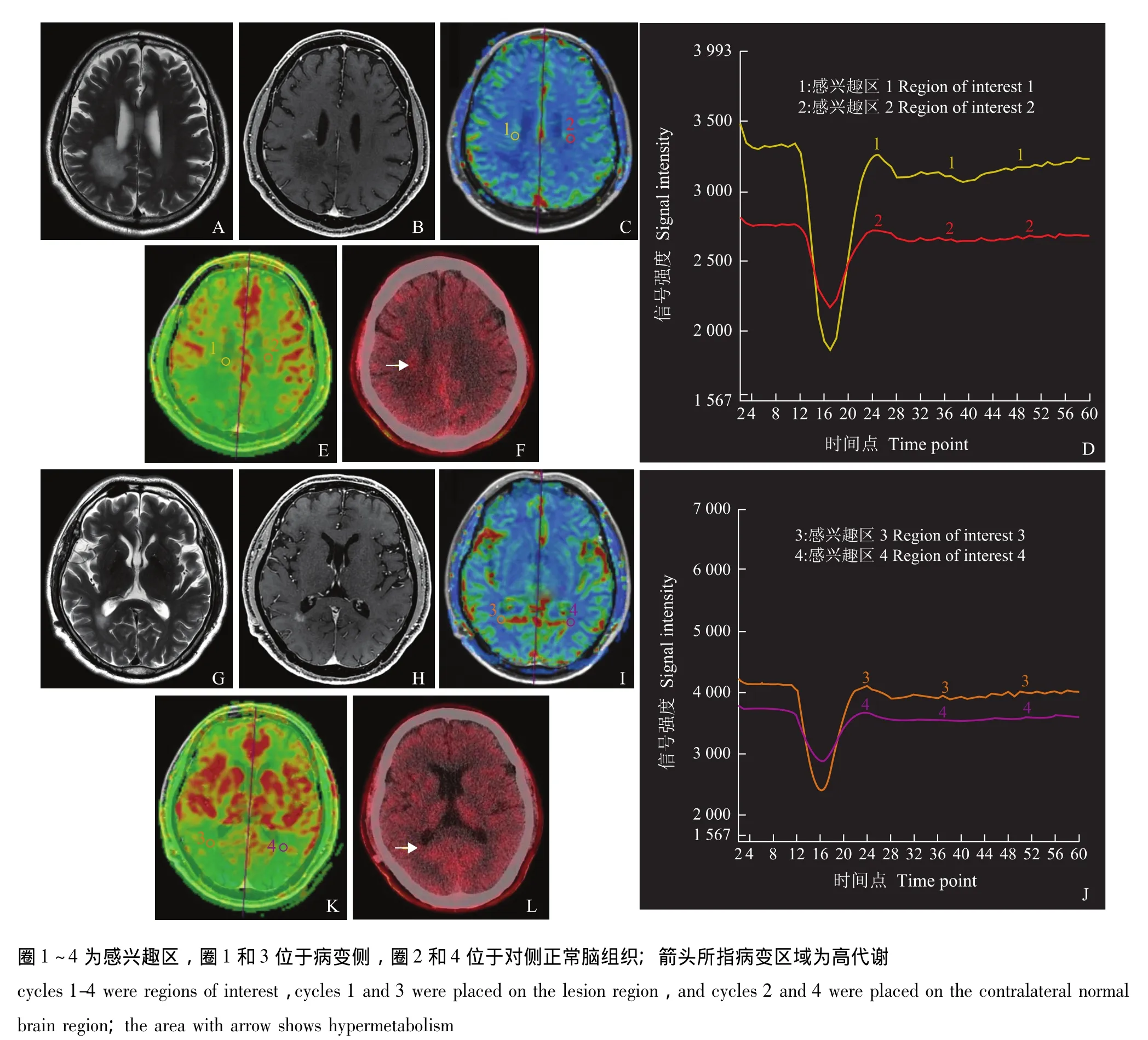
图3 男性,54岁,左手麻木无力,间断头痛26 d,临床诊断为炎性脱髓鞘,病变位于右侧侧脑室后角旁,呈长T2信号影 (A、G),增强后病变明显强化 (B、H),DSC-PWI提示强化部分呈高灌注 (C、D、I、J),3D-pCASL显示病变为高灌注 (E、K),MET-PET/CT提示病变为高代谢 (F、L)Fig 3 A 54-year-old patient who had complained the numbness of left hand and interrupt headache was diagnosed as demyelination.The lesion was mainly located in the posterior horn of the right lateral ventricle.The lesion showed hyperintensity on T2 weighted imaging(A and G),evident enhancement on post-contrast images(B and H),and hyperperfusion on DSC-PWI(C,D,I,and J).3D-pCASL demonstrates hyperperfusion(E and K),and MET-PET/CT presents hypermetabolism(F and L)
讨 论
3D-pCASL主要容积灌注成像,可以对全脑进行三维数据采集,扫描范围覆盖大,信噪比高,相对于传统的流动敏感替代反转恢复成像[10-11]具有较强的优势。但是对于其结果的评价,目前主要以DSC-PWI为金标准进行对照研究,本研究尝试对3D-pCASL、DSC-PWI及PET/CT进行对比研究,以检验3D-pCASL在临床疾病诊断中的价值。
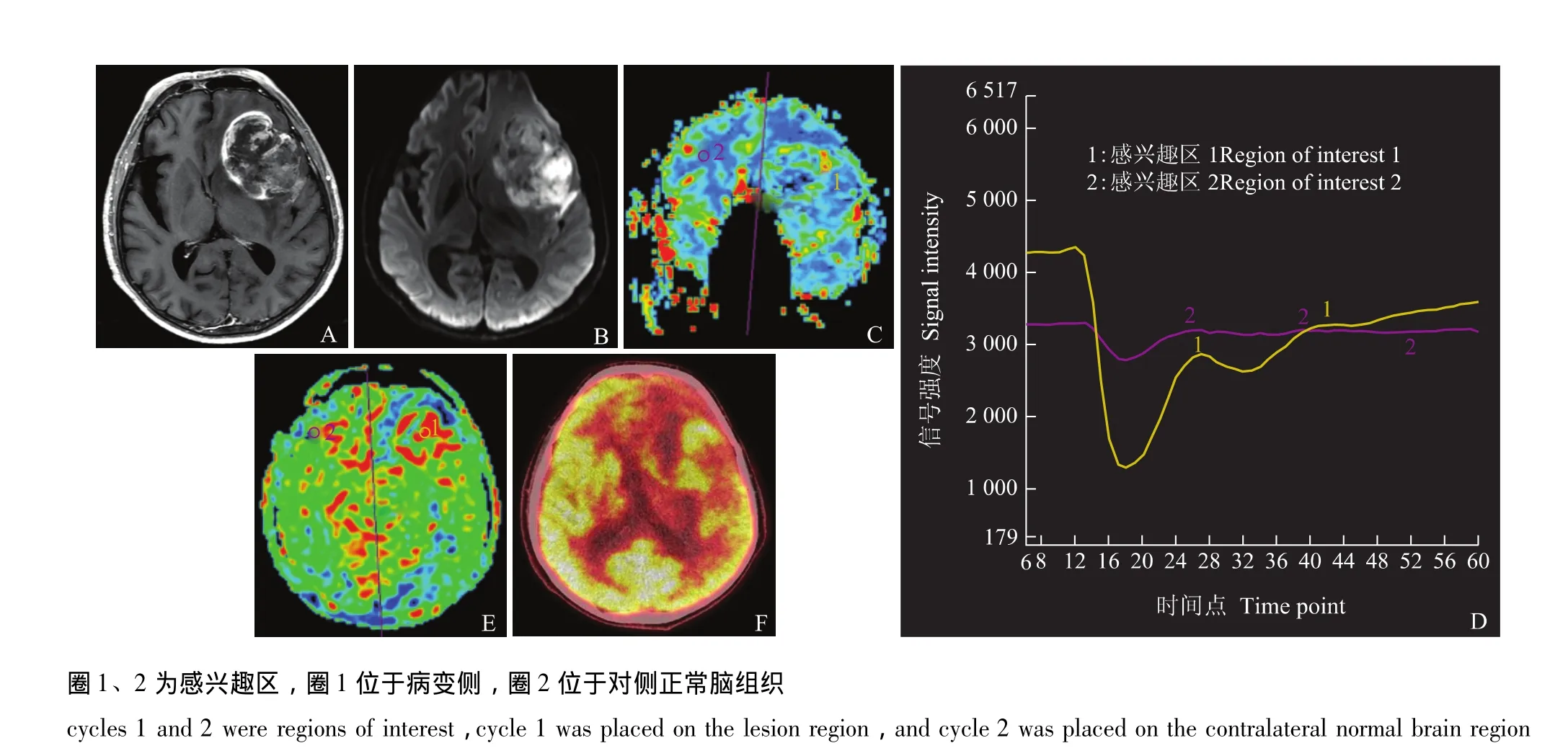
图4 男性,54岁,头痛3个月,病变位于左侧额叶、岛叶及基底节区,MRI证实病变明显强化 (A),DWI为高信号 (B),DSCPWI病变为高灌注 (C、D),3D-pCASL病变为高灌注 (E),FDG-PET/CT显像病变为高代谢 (F)Fig 4 A 54-year-old male patient suffered from headache for 3 months.The lesions were mainly located in the left frontal lobe,insular lobe,and basal ganglia region.The lesion showed evident enhancement on MRI(A)and hyperintensity on DWI(B)and hyperperfusion on DSC-PWI(C and D).3D-pCASL shows hyperperfusion(E),and FDG-PET/CT demonstrates hypermetabolism(F)
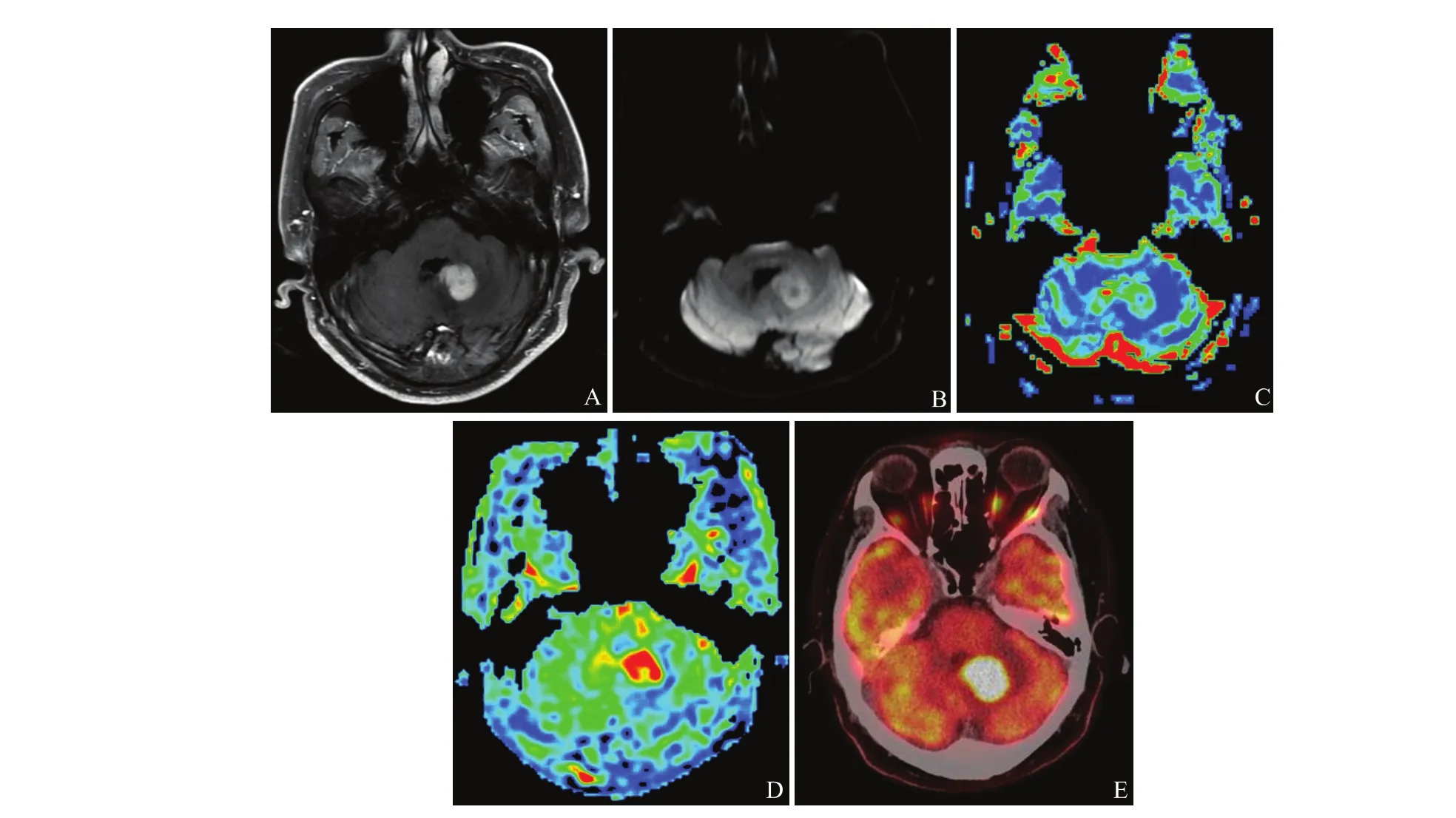
图5 男性,49岁,行走不稳2周,病理诊断为非霍奇金氏淋巴瘤,MRI证实病变位于左侧小脑半球,增强后明显均匀强化 (A),DWI为高信号 (B),DSC-PWI为高灌注 (C),3D-pCASL病变为高灌注 (D),FDG-PET/CT显像为显著高代谢 (E)Fig 5 A 49-year-old male patient complained unstable gait for two weeks,and the pathological diagnosis was non-Hodgkins lymphoma.MRI demonstrates that the lesions were mainly located in the left cerebellum,and showed evident enhancement(A)and hyperintensity on DWI(B)and hyperperfusion on DSC-PWI(C),3D-pCASL shows hyperperfusion(D),and FDG-PET/CT reveals evident hypermetabolism(E)
本研究纳入病变主要分为肿瘤性病变、炎性病变、感染性病变及代谢性脑白质病。对于肿瘤性病变,可以观察到3D-pCASL的灌注和DSC-PWI的灌注是完全一致的。对于胶质瘤,低级别胶质瘤主要表现为低灌注、SUVmax值减低,而高级别胶质瘤表现为高灌注、SUVmax值较对侧增高,表明对于胶质瘤的诊断,3D-pCASL和PET/CT具有相同的诊断价值。本研究纳入原发性中枢神经系统淋巴瘤1例,3D-pCASL及DSC-WPI主要表现为高灌注,FDG-PET/CT表现高代谢 (SUVmax值显著高于胶质瘤的SUVmax值)。对于脑内的淋巴瘤,主要表现为低灌注,因此灌注成像通常用于淋巴瘤与胶质瘤及转移瘤的鉴别[12]。但也有淋巴瘤高灌注的报道[13],高灌注的发生可能与小血管直径的明显增粗有一定的关系,尽管无明显的肿瘤新生血管形成[14]。对于MRI表现为高灌注,但常规影像又不符合胶质瘤表现的患者,FDG-PET/CT的表现对其诊断具有较高价值[15]。
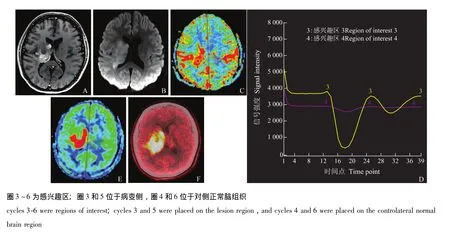
图6 女性,16岁,左侧肢体无力20 d,病理诊断为间变性星形细胞瘤,MRI提示病变主要位于右侧丘脑、尾状核及右侧侧脑室旁白质,MRI证实病变明显强化 (A),DWI为高信号 (B),DSC-PWI为高灌注 (C、D),3D-pCASL为高灌注 (E),FDG-PET/CT显像病变明显高代谢 (F)Fig 6 A 16-year-old female patient suffered from the weakness of left limb for 20 days,and the pathological diagnosis was anaplastic astrocytoma,MRI demonstrated that the lesion showed evident enhancement(A)and hyperintensity on DWI(B),and hyperperfusion on DSCPWI(C and D),the lesion shows hyperperfusion on 3D-pCASL(E)and hypermetabolism on FDG-PET/CT(F)
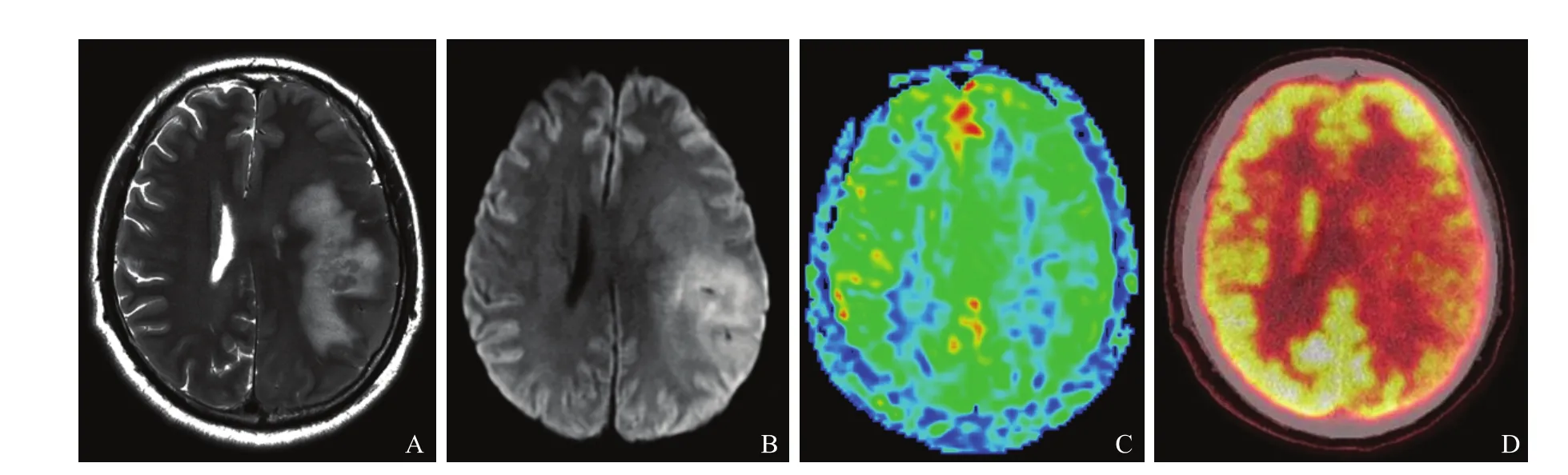
图7 男性,58岁,右侧肢体无力1个月,病理诊断为低级别胶质瘤 (WHOⅡ级),病变位于左侧额顶叶,呈长T2信号影 (A),DWI呈高信号 (B),3D-pCASL病变与对侧比较呈低灌注 (C),FDG-PET/CT病变与对侧比较呈低代谢 (D)Fig 7 A 58-year-old male patients suffered from the weakness of right limb for 1 month,and the pathological diagnosis was low grade glioma(WHOⅡ),the lesions were mainly located in the left frontal and parietal lobe,and shows hyperintensity on T2 weighted imaging(A)and DWI(B),the lesion shows hypoperfusion on 3D-pCASL(C)and hypometabolism on FDG-PET/CT(D)compared with contralateral normal brain parenchyma
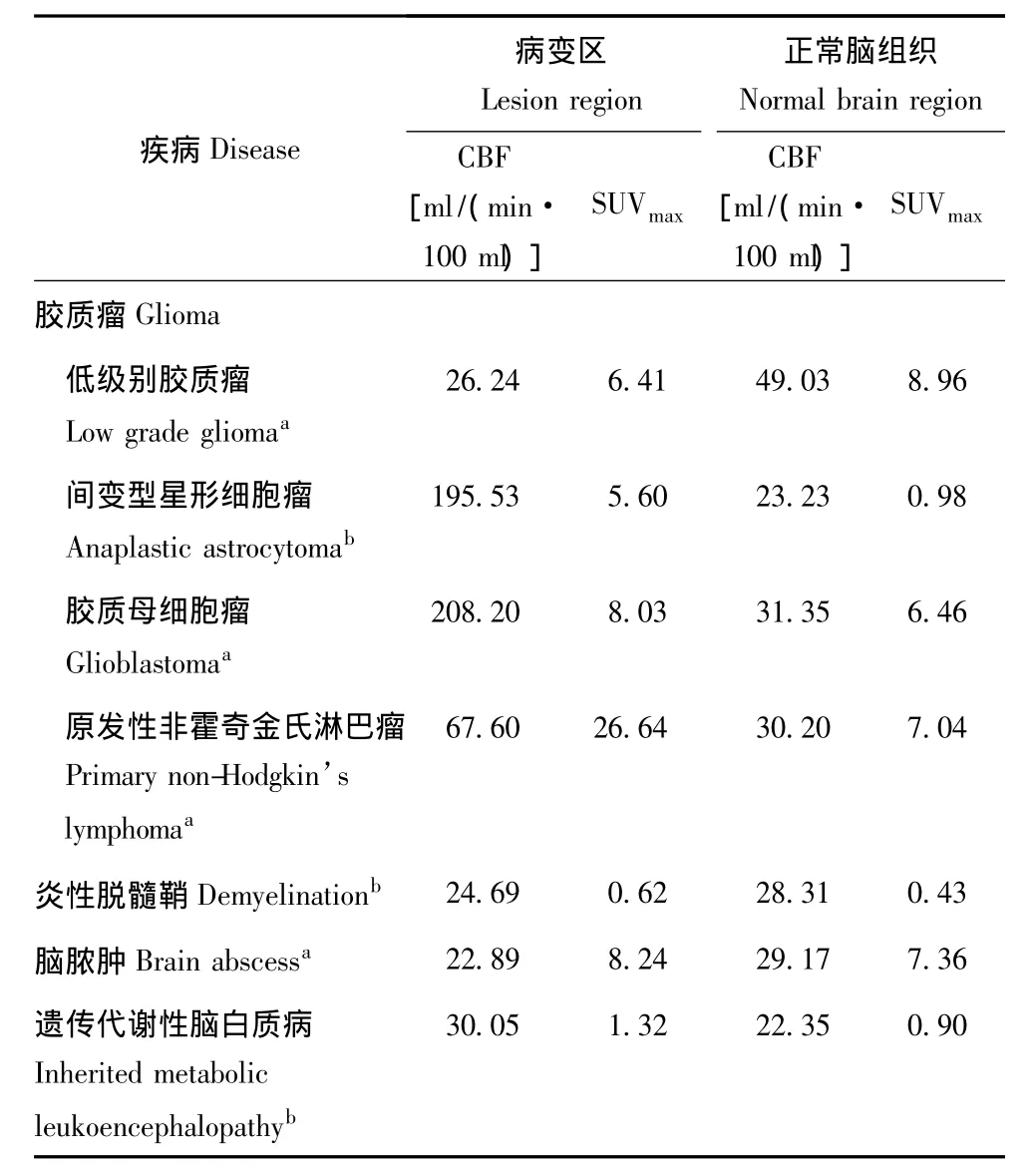
表1 不同疾病脑部病变区及正常脑组织CBF及SUVmax值比较Table 1 Comparison of CBF and SUVmaxvalue for the brain lesions and normal brain tissue in different disease
本研究对1例临床诊断为炎性脱髓鞘的患者进行3D-pCASL、DSC-PWI及PET/CT,测量部位主要为病变强化部分,3D-pCASL与DSC-PWI均表现为高灌注,而PET/CT表现为高代谢。对于炎性脱髓鞘性疾病,增强斑块通常为急性期的斑块,灌注成像表现为高灌注,非增强斑块为慢性期斑块,灌注成像为低灌注[16-20]。因此,3D-pCASL与 DSC-PWI对于炎性病变的诊断具有一定帮助,而3D-pCASL由于其容积灌注成像的特点及不需要注射对比剂,相信其在临床具有广泛的用途,尤其是对于无法使用对比剂的患者。
脑脓肿常规影像学表现为长T1长T2信号,DWI为显著高信号,脓肿壁通常明显强化。但对于不典型的脑脓肿,通常需要与脑内的囊性肿瘤性病变进行鉴别。对于脑内的常见肿瘤为神经上皮肿瘤,通常灌注表现为高灌注,PET/CT为高代谢,而脓肿壁属于炎性病变,通常表现低灌注。对于本研究患者3D-pCASL与 DSC-PWI均表现为低灌注,表明3D-pCASL对于感染性病变具有与DSC-PWI相同的诊断价值。而此患者PET/CT表现为高代谢,这与3D-pCASL的结果预示的诊断方向是相反的。因此,对于感染性病变,3D-pCASL序列具有一定的诊断价值。
对于遗传代谢性脑白质病变,通常病变强化部分可以表现高灌注,本研究患者3D-pCASL与DSC-PWI均表现为高灌注。尽管PET/CT表现为高代谢,但其SUVmax值明显低于本研究的肿瘤性病变的SUVmax值,PET/CT结果提示为脑内非肿瘤性病变。因此,对于脑白质病变患者,3D-pCASL可以客观真实地反应病变的灌注状态。
3D-pCASL反应肿瘤内的肿瘤血管生成程度,而PET/CT是从代谢水平对肿瘤的活性程度进行评价。本研究显示肿瘤性病变3D-pCASL主要表现为高灌注,PET/CT表现为高代谢。而对于非肿瘤性病变,由于炎性细胞的存在和病变部位血管通透性的增高,PET/CT可表现为高代谢,不能更为细致地区分病变,相反,3D-pCASL可以将非肿瘤性病变再进一步细分为高灌注和低灌注两种,对病变进行有效的诊断。
综上,3D-pCASL作为一种新的无需注射对比剂的容积灌注成像可以客观真实地反应病变组织的灌注状态,与PET/CT的诊断结果具有较高的一致性。
[1] Detre JA,Leigh JS,Williams DS,et al.Perfusion imaging[J].Magn Reson Med,1992,23(1):37-45.
[2] Parkes LM,Rashid W,Chard DT,et al.Normal cerebral perfusion measurements using arterial spin labeling:reproducibility,stability,and age and gender effects[J].Magn Reson Med,2004,51(4):736-743.
[3] Amann M,Achtnichts L,Hirsch JG,et al.3D GRASE arterial spin labelling reveals an inverse correlation of cortical perfusion with the white matter lesion volume in MS [J].Mult Scler,2012,18(11):1570-1576.
[4] Jarnum H,Steffensen EG,Knutsson L,et al.Perfusion MRI of brain tumours:a comparative study of pseudo-continuous arterial spin labelling and dynamic susceptibility contrast imaging[J].Neuroradiology,2010,52(4):307-317.
[5] Alsop DC,Detre JA.Reduced transit-time sensitivity in noninvasive magnetic resonance imaging of human cerebral blood flow [J].J Cereb Blood Flow Metab,1996,16(6):1236-1249.
[6] Wang JJ,Zhang Y,Wolf RL,et al.Amplitude-modulated continuous arterial spin-labeling 3.0 T perfusion MR imaging with a single coil:feasibility study [J].Radiology,2005,235(1):218-228.
[7] Garcia DM,Duhamel G,Alsop DC.Efficiency of inversion pulses for background suppressed arterial spin labeling [J].Magn Reson Med,2005,54(2):366-372.
[8] Dai W,Garcia D,de Bazelaire C,et al.Continuous flowdriven inversion for arterial spin labeling using pulsed radio frequency and gradient fields[J].Magn Reson Med,2008,60(6):1488-1497.
[9] Herscovitch P,Raichle ME.What is the correct value for the brain-blood partition coefficient for water?[J].J Cereb Blood Flow Metab,1985,5(1):65-69.
[10] Kim SG.Quantification of relative cerebral blood flow change by flow-sensitive alternating inversion recovery(FAIR)technique:application to functional mapping[J].Magn Reson Med,1995,34(3):293-301.
[11] Tsekos NV,Zhang F,Merkle H,et al.Quantitative measurements of cerebral blood flow in rats using the FAIR technique:correlation with previous iodoantipyrine autoradiographic studies[J].Magn Reson Med,1998,39(4):564-573.
[12] Haldorsen IS,Espeland A,Larsson EM.Central nervous system lymphoma:characteristic findings on traditional and advanced imaging [J].AJNR Am J Neuroradiol,2011,32(6):984-992.
[13] Haque S,Law M,Abrey LE,et al.Imaging of lymphoma of the central nervous system,spine,and orbit[J].Radiol Clin North Am,2008,46(2):339-361.
[14] Ferreri AJ,Reni M.Primary central nervous system lymphoma [J].Crit Rev Oncol Hematol,2007,63(3):257-268.
[15] Palmedo H,Urbach H,Bender H,et al.FDG-PET in immunocompetent patients with primary central nervous system lymphoma:correlation with MRI and clinical follow-up [J].Eur J Nucl Med Mol Imaging,2006,33(2):164-168.
[16] Polman CH,Reingold SC,Banwell B,et al.Diagnostic criteria for multiple sclerosis:2010 revisions to the McDonald criteria [J].Ann Neurol,2011,69(2):292-302.
[17] Zamboni P,Menegatti E,Weinstock-Guttman BA,et al.Hypoperfusion of brain parenchyma is associated with the severity of chronic cerebrospinal venous insufficiency in patients with multiple sclerosis:a cross-sectional preliminary report[J].BMC Med,2011,9:22.
[18] Ingrisch M,Sourbron S,Morhard D,et al.Quantification of perfusion and permeability in multiple sclerosis:dynamic contrast-enhanced MRI in 3D at 3T [J].Invest Radiol,2012,47(4):252-258.
[19] Ge Y,Law M,Johnson G,et al.Dynamic susceptibility contrast perfusion MR imaging of multiple sclerosis lesions:characterizing hemodynamic impairment and inflammatory activity[J].AJNR Am J Neuroradiol,2005,26(6):1539-1547.
[20] Haselhorst R,Kappos L,Bilecen D,et al.Dynamic susceptibility contrast MR imaging of plaque development in multiple sclerosis:application of an extended blood-brain barrier leakage correction [J].J Magn Reson Imaging,2000,11(5):495-505.
猜你喜欢
昆明医科大学学报(2021年3期)2021-07-22
影像研究与医学应用(2021年2期)2021-03-09
中国现代医药杂志(2020年12期)2020-02-06
医学新知(2019年4期)2020-01-02
健康大视野(2019年14期)2019-07-19
中国全科医学(2019年35期)2019-01-09
家教世界·创新阅读(2017年7期)2017-08-09
奥秘(2016年6期)2016-07-30
中华老年多器官疾病杂志(2016年8期)2016-05-14
分忧(2016年3期)2016-05-05
