
关节镜下四骨道双束固定治疗急性肩锁关节RockwoodⅤ型脱位
2014-07-05 13:20陆伟王大平朱伟民欧阳侃柳海峰彭亮权李皓冯文哲
中华肩肘外科电子杂志 2014年3期
陆伟 王大平 朱伟民 欧阳侃 柳海峰 彭亮权 李皓 冯文哲
关节镜下四骨道双束固定治疗急性肩锁关节RockwoodⅤ型脱位
陆伟 王大平 朱伟民 欧阳侃 柳海峰 彭亮权 李皓 冯文哲
目的探讨关节镜下四骨道四袢双束固定修复急性肩锁关节RockwoodⅤ型脱位的方法及近期疗效。方法选择2010年10月至2013年6月,12例急性肩锁关节RockwoodⅤ型损伤的患者(男性9例,女性3例),平均年龄28.2岁。10例为运动致伤,2例为跌倒致伤。具体步骤分为5部分:(1)术前测量患者健侧特定体位喙突CT三维影像特点,测量喙突颈部宽度、喙突与肩胛骨的夹角及喙突与锁骨的关系,明确喙突骨道中心点位置及其于锁骨外端的投影;(2)肩关节镜下经盂肱关节暴露喙突下表面,标记喙突骨道中心;(3)于肩锁关节上方做横切口,保留锁骨外端并切除肩锁关节软骨盘;(4)将肩锁关节复位,克氏针临时固定后,采用自行设计的定位器,根据术前测量的喙突与锁骨的骨道定位,分别于锁骨外缘与喙突下表面间各钻相隔约6mm,直径3.5mm骨道(共4条骨道),穿入牵引导线;(5)采用并列的两套双Endobutton袢和Utra-braid固定系统,分别固定于锁骨外端上表面与喙突颈部下表面间。术后采用较积极的康复程序,随访时间6~30个月。术后采用疼痛VAS评分、恢复运动情况、Constant评分、Karlsson肩锁关节评分评价术后疗效。采用SPSS 18.0统计软件进行统计分析。结果术后11例患者获得随访,X线片和CT三维重建显示Endobutton位置良好,无脱出或断裂,无锁骨或喙突骨质吸收,肩锁关节无再发生脱位或半脱位。8例男性患者与1例女性患者术后3~5个月恢复伤前运动水平,包括对抗与过度运动。另外2例因其他原因放弃原来运动,但不影响正常生活和工作。8例术后平均6.34±3.2周时VAS评分<3分,4例术后肩锁关节疼痛持续时间较长(VAS评分4~6分),但12~18周后VAS评分<3分。术后肩关节活动范围平均恢复时间为6.32±2.11周,术后 Constant评分(91.2±1.67)分(88~100分),术后 Karlsson评分10例优,1例良。患者均对治疗效果满意。结论采用关节镜下四骨道四袢双束固定方法修复急性肩锁关节Rockwood-Ⅴ型脱位,生物固定牢固,手术创伤小,并且避免了双袢单骨道应力过于集中、拉力线单薄等缺点,是治疗急性肩锁关节RockwoodⅤ型损伤较好的方法。
肩锁关节;脱位;肩关节镜;四骨道
治疗肩锁关节RockwoodⅤ型脱位的方法较多。过去常用的是创伤较大的切开法(采用锁骨钩钢板固定)。近年来,有学者采用关节镜辅助下锁骨-喙突螺钉固定方法,但需要在6周后取出;还有学者采用关节镜下双Endobutton袢单束固定方法进行固定,效果不错,但发现部分患者发生Endobutton间的缝合线断裂,复发再脱位或袢下骨质吸收[1-4]。本文介绍采用自行设计的定位装置,四骨道四袢双束固定方法,在肩锁关节复位后进行锁骨与喙突固定的12例患者,效果良好,报道如下。
材料与方法
一、患者选择
2010年10月至2013年6月,选择12例急性肩锁关节RockwoodⅤ型损伤的患者(男性9例,女性3例),平均年龄28.2岁。10例为运动致伤,2例为跌倒致伤。所有患者均在伤后2周内行修复术,且手术均由同一位高年资医生完成。
二、术前骨道定位设计
所有患者均采用双侧肩关节90°内旋位(掌心向下)CT扫描,分别测量肩胛骨长轴与冠状面的角度(A),再于喙突颈部做与肩胛骨长轴平行线(S),测量该平行线在喙突颈部宽度(P),喙突颈部的中点即为准备钻制的两个骨道间的中心原点,做该点的与P线的垂直交叉线,骨道定位位于该原点的Ⅰ、Ⅱ象限,两骨道间相距6mm(图1)。
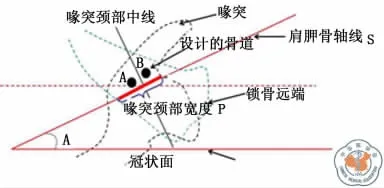
图1 骨道定位示意图
三、手术技术
根据术前测量的骨道数据,用自行设计的肩锁关节双束四骨道定位器。采用两组各两枚Endobutton袢固定方法,进行肩锁关节四骨道双束固定。该技术包括以下5部分内容:(1)肩锁关节探查,喙突下表面显露:采用70°、4.5mm 的关节镜,常规肩锁关节后方入路,并引导做肩锁关节前方入路。于肩胛下肌腱上方,用射频向内侧逐渐分离肩锁关节前内侧关节囊,直到喙突下表面,清理喙突颈部下表面软组织,暴露喙突颈部。(2)肩锁关节探查,肩锁关节盘切除及锁骨外端部分切除成形:经肩锁关节上方做2~3cm与锁骨平行的横切口,分层切开,暴露肩锁关节,清除破裂的关节盘,并将锁骨外端磨平整,之后将肩锁关节复位,克氏针临时固定。(3)采用自行设计的定位器(专利编号ZL 2013 2 0217047.4),将定位器头部放于喙突颈部下表面,横杆及2.4mm定位导针置于锁骨上表面,将导针插入A孔,钻透喙突下表面后,用3.5mm空心钻扩孔。将横杆调整到预先测定的肩胛骨轴线与冠状面的角度,距A孔6mm,再将2.4mm导针插入横杆的B孔扩孔。(4)将一块Endobutton纽扣钢板用3根 Utra-braid线(Smith & Nephew,Andover,Ma)环形连接后,将3条线从喙突下方A孔拉入,锁骨端骨道拉出,纽扣钢板保留在喙突下表面。将另一块Endobutton纽扣钢板穿入拉出的Utrabraid线,收紧后于锁骨端固定并打结,检查肩锁关节固定情况满意。再采用同样方法与B孔进行固定,完成固定过程。(5)固定后采用C臂X线机透视,了解固定效果及内固定物情况。
四、术后康复
术后采用肩锁关节外旋0°位外固定,鼓励患者在48h后进行适当的肩锁关节被动<90°的外展、前屈、外旋活动。术后6周开始主动锻炼,术后3个月开始恢复正常生活、工作并进行有限的恢复性运动。
五、术后评估
采用术后肩锁关节疼痛VAS评分(满分10)、恢复肩锁关节活动范围及恢复运动时间、Constant评分(满分100)、Karlsson肩锁关节评分(A、B、C三个等级)评价术后疗效。
六、统计学分析
应用SPSS 18.0统计软件,采用χ2检验或t检验进行统计学处理。
结 果
一、术前测量结果
12例急性肩锁关节V型脱位患者,术前健侧CT测量,肩胛骨与冠状面夹角为(32.33±5.24)°,喙突与肩胛骨轴线夹角(26.35±1.55)°,喙突颈部横径为(2.05±1.12)cm,喙突骨道中心定位点(骨道原点)在锁骨投影距锁骨外端(2.30±0.69)cm,距锁骨前缘(8.92±0.32)cm,距锁骨后缘(10.89±2.39)cm。
二、术中
术中10例患者定位与术前测量的健侧结果相同,2例患者年龄<20岁,喙突定位点于锁骨的投影较前,骨道钻制较困难。采用将锁骨定位点后移的斜行定位方法,锁骨位点分别后移5~6mm,术中透视及术后影像学检查位置均良好(图2~5)。
三、术后
术后11例患者获得随访,随访时间6~30个月,平均24.2±6.8个月。术后 X线片 Endobutton钛板位置良好,无脱出。8例男性患者与1例女性患者术后3~5个月恢复伤前运动水平,包括对抗与过度运动。另外2例因其他原因放弃原来运动,但不影响正常生活和工作。
8例患者术后平均(6.34±3.2)周时 VAS评分<3分,4例患者术后肩锁关节疼痛持续时间较长(VAS评分4~6分),但12~18周后VAS评分<3分。术后肩锁关节活动范围恢复时间(6.32±2.11)周、术后 Constant评分(91.2±1.67)分(88~100分)、术后Karlsson评分10例优,1例良。与术前相比术后各项评分差异均有统计学意义(表1)。术后无脱位或半脱位复发,患者均对治疗结果满意。

图2~5 肩锁关节Rockwood V型脱位,采用四骨道四Endobutton双束固定后CT扫描所见。图2术前X线片显示右肩锁关节Rockwood V型脱位;图3术后X线片显示肩锁关节完全复位,锁骨端、喙突端固定Endobutton位置良好;图4术后3D-CT显示肩锁关节完全复位,固定Endobutton位置良好;图5术后CT显示骨道-锁骨-喙突的关系
四、典型病例
患者,27岁,因足球守门致伤入院。查体右肩锁关节畸形,隆起,活动障碍。Constant肩锁关节评分22.5分。X线片发现右肩锁关节RockwoodⅤ型脱位。采用全关节镜下四骨道双束4 Endobutton复位固定右肩锁关节,手术过程40min,术后当天出院。术后即开始被动全范围活动锻炼,术后2周开始主动活动锻炼,术后4周肩锁关节活动范围恢复正常,患者恢复日常生活和工作。术后3个月即可开始恢复部分运动。术后6个月恢复足球运动。随访复查内固定位置良好,无肩锁关节松弛或不稳,无锁骨或喙突骨质吸收。Constant评分100分,Karlsson评分优,患者对治疗效果满意。
讨 论
肩锁关节脱位是常见的运动损伤,尤其是在接触性运动如橄榄球、足球、曲棍球、滑雪以及骑自行车时跌倒。根据损伤的严重程度不同,通常将肩锁关节脱位分为RockwoodⅥ型。急性肩锁关节脱位的治疗还存在争议,有报道显示,在一次对超过500位美国骨科运动医学学会的成员的调查结果中,超过80%的受访者选择非手术治疗作为初始方法。然而有20%~40%的患者经保守治疗急性肩锁关节脱位后,出现残余肩锁关节活动时疼痛、感觉异常、无力、抬肩容易疲劳、以及局部畸形等情况[4]。
通常采用的肩锁关节脱位固定的方法为锁骨钩钢板治疗急性肩锁关节RockwoodⅤ型脱位,效果良好。但其创伤较大,肩峰下金属钩可能导致肩峰撞击。多学者报道采用全关节镜下Double-Button固定系统(Smith & Nephew,Andover)固定肩锁关节脱位,其优点是该系统为生物固定,符合肩锁关节微动特点,且固定可靠,足以维持到骨-韧带愈合[1-6]。该装置由2个钛纽扣和4条高强度聚乙烯缝线组成,纽扣分别位于在喙突下和锁骨上方。但该方法有2个明显的缺陷:(1)4条固定缝线可能难以承受较大的喙突-锁骨间分离的张力,导致缝线撕脱或断裂;(2)这种纽扣宽度只有4.0mm,在较大应力下,过度集中的应力会导致其下方的骨质吸收溶解[5,7]。
本组患者采用4骨道双束固定肩锁关节从根本上解决了上述两个问题:12条聚乙烯高强缝线、两端各2个固定袢共4个固定承力单位,分散了应力,增加了固定强度,减小了固定袢下平均受力强度。结果显示随访患者无缝线松脱、无固定袢移位、无固定袢下方骨质吸收溶解,患者对治疗效果满意。本组病例术前测量显示,喙突颈部横径为(2.05±1.12)cm。该结果显示,只要第一个骨道位置不穿破喙突内、外侧骨皮质,假设第一个骨道正好在喙突中点,那么,其距离内侧或外侧喙突皮质的距离至少还有1.05cm,第二个骨道的钻制就是安全的。
全关节镜下或关节镜辅助下进行肩锁关节急性脱位治疗早有报道,主要有螺钉固定与双袢固定两种。前者由切开手术转化而来,固定牢固、可靠,可借助关节镜观察固定情况,但需要在术后3个月取出螺钉,否则可能会因为肩锁关节的微动导致螺钉折断;后者主要为镜下双袢固定,采用的是单束定位器,单束固定,技术相对简单,但因固定点单一,术后问题较多[2,4,6-7]。本技术的关键有 以下几 个方面:首先是术前骨性结构的测量、双骨道中心点的确定。喙突与肩胛骨夹角的测量较重要,如果该夹角太小,要防止术中骨道穿破皮质的可能;其次,骨道中心点位置的确定,该中心点在年龄<18岁的患者会偏前(本组2例),位于锁骨前缘前方,此时,需要相应调整骨道定位器的角度,向后偏离,直到锁骨骨道位置适中为止;最后,B骨道的钻置还要于术中调整定位横杆旋转角度,使其与喙突外倾角对应。另外,破碎的肩锁关节盘必须去除,且应切除锁骨外端5~8mm骨质,防止术后疼痛发生[8]。
该方法有待进一步完善如固定袢所受应力的测量、固定高强缝线所受应力测量,以及需要更长时间的疗效观察。

表1 肩锁关节脱位患者手术前、后评价指标的比较
[1] 赵立连,张耀南,尹自龙,等.全关节镜下双纽扣钢板固定技术治疗急性肩锁关节脱位的初步临床疗效观察[J].中华关节外科杂志:电子版,2010,4(1):11-13.
[2] Paolo RR,Michele FS,Luigi M.Arthroscopic treatment of acute acromioclavicular joint dislocation[J].Arthroscopy,2004,20(6):662-668.
[3] Pierorazio M,Alberto M,Laura B,et al.Suture Rupture in Acromioclavicular Joint Dislocations Treated With Flip Buttons[J].Arthroscopy,2011,27(2):294-298.
[4] Pascal B,Jason O,Olivier G,et al.All-arthroscopic Weaver-Dunn-Chuinard procedure with double-button fixation for chronic acromioclavicular joint dislocation [J].Arthroscopy,2010,26(2):149-160.
[5] Murena L,Vulcano E,Ratti C,et al.Arthroscopic treatment of acute acromioclavicular joint dislocation with double flip button[J].Knee Surg Sports Traumatol Arthrosc,2009,17(12):1511-1515.
[6] 孙贺,陈铭锐,赵卫东,等.喙肩韧带移位重建喙锁韧带的解剖及生物力学研究[J].中国临床解剖学杂志,2002,31(4):303-305.
[7] Liu X,Huangfu X,Zhao J.Arthroscopic treatment of acute acromioclavicular joint dislocation by coracoclavicular ligament augmentation[J].Knee Surg Sports Traumatol Arthrosc,2013.[in print]
[8] 陆伟,王大平,韩云,等.关节镜下肩峰成形与锁骨外端切除术治疗严重肩关节退行性变[J].中华关节外科杂志:电子版,2010,6(1):77-78.
Arthroscopic fixation in the treatment of RockwoodⅤacute acromioclavicular joint dislocation
Lu Wei,Wang Daping,Zhu Weimin,Ou-Yang Kan,Liu Haifeng,Peng Liangquan,Li Hao,Feng Wenzhe.Department of Sport Medicine,1st Affiliated Hospital,Shenzhen University (Shenzhen 2nd People′s Hospital),Shenzhen 518000,China
BackgroundTreatment methods for acromioclavicular joint dislocation of Rockwood type V are numerous.The commonly used is the open surgery with large trauma(by clavicular hook plate fixation).In recent years,some scholars use clavicle-coracoid screws fixation method under arthroscopy,but the screws need to be removed after 6weeks;there are also scholars using arthroscopic double Endobutton loops single bundle fixation method with good effect,but they found suture rupture between the Endobutton,redislocation or fracture,bone absorption under the loops in some patients.This article investigates the method of arthroscopic procedure with four-tunnel quadruple double-bundle Endobutton double-bundle fixation via self-designed positioningapparatus in the treatment of acute acromioclavicular joint(ACJ)RockwoodⅤdegree dislocations and their short-term therapeutic effect.Methods(1)Patient selection:12patients(9male and 3female)with acute acromioclavicular joint dislocation of Rockwood type V were selected from October 2010to June 2013.Their average age is 28.2years.with sports injury in 10cases and fall injury in 2cases.All patients
surgical repair within 2weeks after injury.The operations were performed by the same senior surgeon.(2)Preoperative bone tunnel positioning design:All patients had CT scan in the position of 90°internal rotating of bilateral shoulder joint(palm down).Measure the angle of scapular long axis and coronal section(A)separately,make the line in the coracoid neck parallel to the long axis of scapula(S),and then measure the width of parallel line in the part of coracoid neck(P).The midpoint of the coracoid neck is the center between the two preparatively drilled bone tunnels.Make the cross line vertical to line P,and the bone tunnels are located in the I and II quadrant.The distance between two bone tunnels is 6mm.(3)Surgical techniques:According to the data of preoperative measurement of bone tunnel,the self-designed 4-tunnel double-bundle locator is applied.The 4-tunnel double-bundle acromioclavicular joint fixation is carried out with the method of two Endobutton loops in each of two groups.The technique includes the following 5parts:①Acromioclavicular joint exploration and exposure of subcoracoid surface:make the routine posterior approach of acromioclavicular joint with arthroscope of 70°,4.5mm and guide the anterior approach.Gradually separate the anteromedial joint capsule with radiofrequency coblation from the inside of the subscapularis tendon above to the subcoracoid surface.Clean the soft tissue on its lower surface to expose the coracoid neck.② Acromioclavicular joint exploration,acromioclavicular joint disc excision and partial excision and plasty of the clavicular lateral end:make a 2-3cm transverse incision above the acromioclavicular joint parallel to the clavicle,layered the cut,expose the acromioclavicular joint,remove ruptured joint disc,and rub the clavicular lateral end.Afterwards,reduce the acromioclavicular joint and fix it temporarily with Kirschner wire.③ The self-designed locator(Patent No.ZL 201320217047.4)is adopted.Put the head of the locator on the lower surface of coracoid neck,and the transverse bar and 2.4mm guide pin are arranged on the clavicular surface.The guide pin is inserted into the hole A,drilling through the subcoracoid surface with a 3.5mm hollow drill for reaming.Adjust the transverse bar to the pre-determined angle of scapular axis and coronal section 6mm away from hole A,and then ream the hole B with 2.4mm guide pin inserted.④ After connecting the ring with an Endobutton button plate and 3Utra-braid sutures(Smith & Nephew,Andover,Ma),pull in the 3line from hole A below the coracoid process,and then pull out from the bone tunnel on the clavicular end to maintain the Endobutton plate on the subcoracoid surface.The Utra-braid suture penetrates into the other piece of Endobutton plate and then gets pulled out.Tighten and fix it on the clavicular end and then make a knot.Check the acromioclavicular joint to ensure satisfactory fixation.Complete the process of hole B fixation with the same method.⑤ Use C arm X-ray machine for fluoroscopy to understand the effect of fixation and situations of internal fixator.Aggressive postoperative rehabilitation program was applied,and the follow-up time ranged from 6to 30months.(4)Postoperative rehabilitation:After operation the acromioclavicular joint was externally fixed in 0°of external rotation,and 48hours later the patient was encouraged to take appropriate acromioclavicular joint passive activities of abduction less than 90°,flexion and external rotation.Active exercise was allowed 6weeks after operation,and 3months later the patient began to return to normal life,work and limited recovery movement.(5)Postoperative evaluation:The VAS score(out of 10)of postoperative acromioclavicular joint pain,recovery of range of movement for acromioclavicular joint and recovery time, Constant score (out of 100),and Karlsson acromioclavicular joint score(A,B,C three grades)were applied for postoperative evaluation.(6)Statistical analysis:SPSS 18.0statistical software was applied,andχ2test and t test were adopted respectively for statistical process.Results(1)Resultsof preoperative measurement:Preoperative contralateral CT measurement was conducted in 12cases of acute acromioclavicular joint dislocation with Rockwood type V.The angle between the scapula and coronal section was(32.33±5.24)°,theangle between the coracoid and scapular axis was (26.35±1.55)°,the diameter of coracoid neck was(2.05±1.12)cm,and the central location of coracoid bone tunnel(the original point of clavicular bone tunnel)in the projection of clavicle are(2.30±0.69)cm from the distal clavicle,(8.92±0.32)cm from the front edge of the clavicle,and (10.89±2.39)cm from trailing edge of the clavicle.(2)Intraoperation:Intraoperative positioning and preoperative measurement have the same result in 10 cases.2patients are younger than 20years old and their anchor points are a bit forward in the projection of clavicle,which makes it difficult to drill the bone tunnels.The oblique positioning method of shifting anchor point backward is applied to move the points 5-6mm back on the clavicle,and both the positions are good under intraoperative fluoroscopy and postoperative radiological examination.(3)Post operation:11patients were followed up after operation for 6to 30months with an average of 24.2±6.8months.Postoperative X-ray films and 3D-CT indicated that Endobutton titanium plate was in good position without withdrawal or rupture.No dislocation or subluxation relapse was seen after the operation.8male patients and 1female patient restored pre injury sports level in 3to 5months after surgery,including resistive and excessive movement.The other 2patients returned to normal life but gave up previous sports due to other reasons.The VAS score in 8patients was less than 3after operation in a mean of 6.34±3.2weeks and 4patients had acromioclavicular joint pain of longer duration(VAS score 4-6),but the VAS score turned less than 3in 12-18weeks later.The recovery time was 6.32±2.11weeks in the postoperative range of joint movement.The postoperative Constant score was(91.2±1.67)(88-100)and the postoperative Karlsson score were excellent in 10cases and benign in 1case.Compared with the preoperative and postoperative scores the differences were statistically significant.All the patients were satisfied with the therapeutic outcomes.Conclusions The method of arthroscopic procedure with four-tunnel quadruple Endobutton doublebundle fixation in the treatment of acute acromioclavicular joint dislocation of Rockwood type V provides stable biological fixation with minimal invasion and avoids demerits such as the overconcentrations of stress on double-loop single bone tunnel,weak and thin of the tension line,etc.and it is a better treatment method for acute acromioclavicular joint dislocation of Rockwood type V.
Acromioclavicular joint;Dislocation;Shoulder arthroscopy;4-tunnel
Wang Daping,Email:winerl@sina.com
2014-06-27)
(本文编辑:李静)
10.3877/cma.j.issn.2095-5790.2014.03.005
518000 深圳大学第一附属医院(深圳市第二人民医院)运动医学科
王大平,Email:winerl@sina.com
陆伟,王大平,朱伟民,等.关节镜下四骨道双束固定治疗急性肩锁关节RockwoodⅤ型脱位[J/CD].中华肩肘外科电子杂志,2014,2(3):157-162.
猜你喜欢
创伤外科杂志(2022年1期)2022-01-27
中华养生保健(2020年10期)2021-01-18
中华肩肘外科电子杂志(2020年1期)2020-08-24
中华肩肘外科电子杂志(2019年4期)2019-08-24
中华肩肘外科电子杂志(2019年4期)2019-08-24
中华肩肘外科电子杂志(2019年4期)2019-08-24
意林(2018年6期)2018-04-03
爱你(2017年35期)2017-11-24
Coco薇(2017年5期)2017-06-05
中华骨与关节外科杂志(2017年1期)2017-05-17
