
肘关节镜辅助下复位固定治疗尺骨冠状突骨折
2014-07-05 13:20杨顺向明杨国勇陈杭胡小川唐浩琛
中华肩肘外科电子杂志 2014年3期
杨顺 向明 杨国勇 陈杭 胡小川 唐浩琛
·论著·
肘关节镜辅助下复位固定治疗尺骨冠状突骨折
杨顺 向明 杨国勇 陈杭 胡小川 唐浩琛
目的介绍在肘关节镜辅助下复位固定治疗尺骨冠状突骨折的手术方法,并通过临床病例随访分析其疗效。方法自2009年11月至2012年1月共收治16例尺骨冠状突骨折(Morry-Regan分型Ⅱ~Ⅲ)患者,其中14例得到随访。终末随访时应用X线片评估骨折愈合情况,应用改良肘关节HSS评分评价肘关节功能,根据VAS进行疼痛评分。结果术后平均随访12.6个月(8~24个月)。所有患者术中均达到解剖复位。终末随访时改良肘关节HSS平均33分(28~35分),平均VAS疼痛评分(1.2±0.5)分,平均肘关节屈曲132.4°,平均伸直10.6°,总体优良率为100% (14/14)。结论在肘关节镜辅助下,复位固定治疗尺骨冠状突骨折的手术方式,手术创伤小,复位固定可靠,术后肘关节恢复时间短,是治疗尺骨冠状突骨折的一种有效方法。
关节镜;尺骨骨折;外科手术,最小侵入性
尺骨冠状突骨折反映了肘部创伤的严重程度[1]。主要是由于肘关节伸直位跌倒,冠状突与肱骨滑车碰撞所致,常导致肘关节不稳定[2]。暴力大时常合并肘关节脱位,骨折块较大时由于肌腱牵拉,复位不容易维持,使肘关节稳定性受到严重影响,常需手术治疗,恢复关节的稳定性。本院自2009年11月至2012年1月在肘关节镜辅助下复位固定治疗16例尺骨冠状突骨折,报道如下:
资料与方法
自2009年11月至2012年1月应用肘关节镜辅助下复位固定治疗16例尺骨冠状突骨折患者,其中男性10例,女性6例;年龄24~51岁,平均39岁;摔伤11例,车祸伤5例;左侧6例,右侧10例;合并肱骨小头骨折1例,合并后外侧旋转不稳定3例;骨折按Regan-Morrey分型:Ⅱ型10例,Ⅲ型6例。
术前经肘关节X线、CT及三维成像检查(图1~4)后确诊,精确了解骨折部位、骨折块大小、移位程度[3]。手术在全麻下进行,采用侧卧位,患肢置于肘托上(如图5~10)。术中应用充气式止血带,充气压力240mmHg,止血带时间40~90min,平均(63.3±25.0)min。肘关节镜手术采用屈肘位近端前外侧入路及近端前内侧入路,因为:(1)近端前内侧入路距离尺神经、正中神经最远,为内侧入路中最安全的入路(尺神经的距离为15.5mm,正中神经的距离为13.8mm);(2)近端前外侧入路距离桡神经(距桡神经10mm)最远,镜子操作灵活,镜下视野良好,为外侧入路中最安全、有效的入路;(3)肘关节屈曲90°位与伸直位比较,神经更远离入路穿刺点,因此选择在肘关节屈曲90°位时穿刺更安全[4]。通常采用中外侧入路注水,充盈肘关节,建立关节镜通道,刨削清理关节内瘀血及滑膜,暴露冠状突骨折块,关节镜辅助下以探钩复位,复位满意后行克氏针或螺钉固定,螺钉或克氏针自尺骨后侧至冠状突方向固定,螺钉选择合适长度的直径3.0mm中空螺钉,尖端穿过冠状突前方均不超过2mm(如图11~12)。如应用克氏针,针尾折弯后留于皮下。存在伴随损伤(如肱骨小头骨折)需同时固定及行切开操作,包括(如后外侧旋转不稳定)内、外侧副韧带的修补或重建等。术后屈肘固定1周后,在医生指导下行早期功能锻炼。

图1~4 伤后X线片及CT片。肘关节正位(图1)和侧位(图2)X线片提示尺骨冠状突骨折;肘关节矢状位CT平扫片(图3)和CT重建片(图4)提示尺骨冠状突骨折Regan-MorreyⅡ型

图5~10 术中体位及复位固定照片。图5术中体位;图6关节镜下探查复位冠状突;图7第1枚克氏针固定;图8第2枚克氏针固定;图9螺钉固定后;图10固定后骨折端稳定

图11~12 术后X线片。术后肘关节正位(图11)和侧位(图12)X线片提示尺骨冠状突骨折术后对位对线良好,二枚空心钉固定有效在位
结 果
其中14例得到随访,平均随访12.6(8~24)个月。术后切口均Ⅰ期愈合,无切口渗液、神经损伤及骨折再移位发生,1例发生异位骨化。终末随访时应用X线片评估骨折愈合情况,X线片显示骨折均临床愈合,愈合时间为10~14周,平均12周。所有患者术中均达到解剖复位。终末随访时改良肘关节HSS平均33(28~35)分,视觉模拟评分法平均(visual analog scale,VAS)疼痛评分(1.2±0.5)分,平均肘关节屈曲132.4°,平均伸直10.6°,平均旋前68.5°,平均旋后78.6°(如图13~18),总体优良率为100%(14/14)。
讨 论
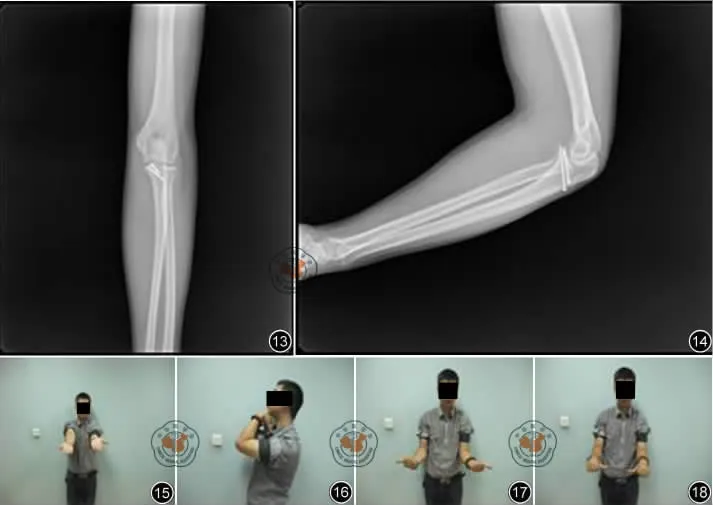
图13~18 术后18个月X线片及功能图像。肘关节正位(图13)和侧位(图14)X线片提示尺骨冠状突骨折术后对位对线良好,二枚空心钉固定有效在位,骨折已愈合;肘关节伸直0°(图15),屈曲130°(图16),旋后80°(图17),旋前60°(图18)
尺骨冠状突与尺骨鹰嘴构成尺骨半月切迹,与肱骨滑车构成屈戌关节。尺骨冠状突是肘关节前方最主要的骨性阻挡结构,与内侧副韧带并列为防止肘关节后脱位及后内侧旋转不稳定的重要组成部分,尺骨冠状突也是肘关节前方重要软组织的附着点,包括前方关节囊、内侧副韧带前束、肱肌等,起抵抗肱二头肌、肱肌和肱三头肌牵拉尺骨向肘后移位的作用,是维持肘关节稳定的主要结构。冠状突是前柱和内侧柱的重要组成部分,构成肘关节前方稳定环[5],当其损伤时,将导致肘关节前方和内侧不稳定。如处理不当或不及时,很容易引起习惯性脱位。因此,在治疗尺骨冠状突骨折时,恢复或重建冠状突的高度和形状以及修补或重建内侧副韧带前束显得非常重要。随着对肘关节研究的深入,尺骨冠状突在肘关节稳定性中的重要作用目前已得到公认,其骨折通常会造成复杂的创伤性肘关节不稳定,因此尺骨冠状突骨折的治疗也越来越受到临床医生的重视[6]。骨折块较大(Regan-MorreyⅡ型、Ⅲ型)时,由于屈肌牵拉、骨折块移位,易伴随肘关节不稳定,手法复位骨折块位置维持困难。由于骨折位于肘窝内,暴露、固定困难,特别是冠状突小块或粉碎性骨折尤为明显。治疗方法不得当,易引起关节失稳,并发创伤性关节炎、骨化性肌炎和关节僵硬等。
冠状突骨折属于关节内骨折,解剖复位和坚强内固定治疗关节内骨折是恢复关节功能的基础。解剖复位有利于关节的活动,减轻关节疼痛,防止创伤性关节炎的发生;坚强内固定利于早期功能锻炼,防止肘关节的僵硬,减少肌肉萎缩,阻止动力性不稳和创伤性关节退变的发生,获得较好的功能。尺骨冠状突骨折常合并肘关节不稳定,国外学者相关系列病例报道中探讨了治疗方案与相关预后,同时也提出了诊断标准及手术治疗方案[7-9];国内学者也有类似报道和文献综述,介绍治疗经验,讨论新手术入路及方案等[8]。
目前主要的固定方法有钢丝固定、克氏针固定、微型螺钉内固定、微型钢板内固定和可吸收螺钉内固定[10-13]等。目前对尺骨冠状突骨折切开复位内固定常规从前路手术,但直视下将骨折的冠状突复位内固定非常困难,因为:(1)肘关节前方血管、神经排列紧密,必须经血管神经间隙或肌间隙进入,可能增加副损伤;(2)冠状突位置较深,触及骨折线难度非常大,因为尺骨冠状突上有很多软组织与之相连并牵拉之,在此情况下很难从前方摸清骨折线并复位;如果将冠状突上的软组织彻底切除,包括前内侧面高耸结节内侧副韧带前束止点、肱肌止点及关节囊,复位虽容易了许多,但在某种程度失去了复位的意义;(3)冠状突骨折块往往比较小,从前方压紧后手指又占据了打孔固定的位置;(4)开放复位手术创伤大,易形成异位骨化,同时遗留较大手术疤痕,影响美观。
随着对肘关节功能解剖的深入了解及患者对肘关节功能要求的提高,微创手术越来越成为关节内骨折安全、有效的治疗方法。因关节镜下手术具有创伤小和恢复快的优点,近年来其应用在肘关节内骨折取得了较快的进展。在急性肘关节创伤中,肘关节镜技术不仅可以进行小骨折块或脱落软骨的清理,还可行复位内固定术。如桡骨头骨折、鹰嘴骨折、冠突骨折、肱骨髁骨折等复位内固定术均有报道[14]。Adams等[15]应用肘关节镜对7例尺骨冠状突骨折进行复位固定,终末随访疗效满意,无异位骨化及肘关节炎发生。
肘关节镜入路采用屈肘位近端前外侧入路及近端前内侧入路,因为:(1)近端前内侧入路距离尺神经、正中神经最远,为内侧入路中最安全的入路(尺神经的距离为15.5mm,正中神经的距离为13.8mm);(2)近端前外侧入路距离桡神经(距桡神经10mm)最远,镜子操作灵活,镜下视野满意,为外侧入路中最安全、有效的入路;(3)肘关节屈曲90°位与伸直位比较,神经更远离入路穿刺点,因此选择在肘关节屈曲90°位时穿刺更安全[4]。对于Regan-MorreyⅡ型且伴粉碎性骨折,术前CT充分估计骨折块大小,因骨折块较小,行空心螺钉固定可能造成骨折块破裂,而且固定效果不确切。为防止这种情况发生,我们对Regan-MorreyⅡ型且伴粉碎性骨折行自尺骨后侧至冠状突方向克氏针固定;对Regan-MorreyⅡ型单纯骨折及Regan-MorreyⅢ型骨折块较大者,行自尺骨后侧至冠状突方向空心螺钉固定。
与其他关节相比,肘关节镜技术要求更高,术者必须非常熟悉肘关节周围的解剖[16]。因为肘关节周围解剖复杂,有很多重要的神经血管,肘关节镜手术虽然作为一种有效微创的治疗手段,并发症的发生率比膝、肩等关节镜手术高,但是绝大多数都是轻微可逆的,并且经过一定的措施这些并发症也是可以避免的,故肘关节镜是一种安全有效的技术[17]。此外,关节镜技术可提供更好的关节内视野,更少的手术创伤,更短的术后康复时间。
应用肘关节镜辅助下复位固定治疗尺骨冠状突骨折的手术方式,肘关节具有手术切口小、创伤小、效果好和恢复快等优点。关节镜能直接观察关节面,使关节内骨折解剖复位,减少创伤性关节炎,并且可使神经、血管损伤等并发症减至最少,还可减少手术创伤,降低肘关节损伤的并发症,但要求术者有丰富的镜下操作经验及局部解剖知识,严格手术适应证的选择,才能最大限度地避免并发症的发生[18]。
[1] Bucholz RW,Heckman JD.Fracture and dislocations of the elbow Rockwood & Green’s Fractures in Adults fracture and dislocations of the elbow [M].Philadelphia LippincottWilliams & Wilkins,2001.
[2] Garrigues GE,Wray WH 3rd,Lindenhovius AL,et al.Fixation of the coronoid process in elbow fracturedislocations[J].J Bone Joint Surg Am,2011,93(20):1873-1881.
[3] 陈子贤,张亮,陈统一.肘三联征诊断和治疗进展[J].国际骨科学杂志,2012,33(5):288-290.
[4] 王虎,蔡道章.肘关节镜的入路选择的应用解剖研究[J].中国临床解剖学杂志,2007,25(4):369-372.
[5] Heim U.Kombinierte verletzungen Von radius and ulna im proximalen untearmsegment[J].Hefte Unfallchir,1994,241:61-79.
[6] Doornberg JN,de Jong IM,Lindenhovius AL,et al.The anteromedial facet of the coronoid process of the ulna[J].J Shoulder Elbow Surg,2007,16(5):667-670.
[7] O′Driscoll SW,Jupiter JB,Cohen MS,et al.Difficult elbow fractures:pearls and pitfalls[J].Instr Course Lect,2003,52(52):113-134.
[8] 李庭,王满宜,蒋协远,等.肘关节“可怕三联征”的诊断与治疗[J].中华骨科杂志,2009,29(12):398-403.
[9] Wells J,Ablove RH.Coronoid fractures of the elbow[J].Clin Med Res,2008,6(1):40-44.
[10] 郭志民,练克俭,丁真奇,等.微型钢板在尺骨冠状突骨折中的临床应用[J].中国骨与关节损伤杂志,2008,23(7):585-586.
[11] Doornberg JN,Ring DC.Fracture of the anteromedial facet of the coronoid process[J].J Bone Joint Surg Am,2006,88(10):2216-2224.
[13] 廖苏平,危蕾,吴波,等.应用微型可吸收钉治疗尺骨冠状突骨折[J].中国骨与关节损伤杂志,2009,24(5):444-445.
[14] 郑佳鹏,张春礼.肘关节镜技术进展[J].中国矫形外科杂志,2008,16(22):1708-1710.
[15] Adams JE,Merten SM,Steinmann SP.Arthroscopic-assisted treatment of coronoid fractures[J].Arthroscopy,2007,23(10):1060-1065.
[16] Atesok K,Doral MN,Whipple T,et al.Arthroscopy-assisted fracture fixation[J].Knee Surg Sports Traumatol Arthrosc,2011,19(2):320-329.
[17] 徐雁,王健全,崔国庆,等.46例肘关节镜手术并发症的分析--10年269例肘关节镜手术回顾[J].中国微创外科杂志,2011,11(7):615-618.
[18] Abboud JA,Ricchetti ET,Tjoumakaris F,et al.Elbow arthroscopy:basic setup and portal placement[J].J Am Acad Orthop Surg,2006,14(5):312-318.
Elbow arthroscope assisted reduction and fixation treatment for coronoid fracture
Yang Shun,Xiang Ming,Yang Guoyong,Chen Hang,Hu Xiaochuan,Tang Haochen.Department of Upper Extremity,Sichuan Province Orthopaedic Hospital,Chengdu 610041,China
BackgroundCoronoid fracture of ulna reflects the severity of the elbow trauma.It is mainly due to the fall with the elbow in a straight position,which caused by collision with trochlea of humerus,leading to elbow instability.Violent trauma often causes elbow dislocation.If the fracture block is large,because of the pulling force of tendon,it is not easy to maintain reduction,and the stability of the elbow is badly affected,often requiring surgery treatment to restore the stability of the joints.In our hospital,From November 2009to January 2012,we treated 16cases with fracture of coronary fracture with elbow arthroscopy assisting reduction and fixation.MethodsFrom November 2009to January 2012,we treated 16cases with fracture of coronary fracture with elbow arthroscopy assisting reduction and fixation,including 10males and 6females,with an average age of 39(24-51).There are 11cases caused by fall and 5cases caused by traffic accidents;6cases were the left side,and 10cases were on the right side;There were one case combined with fracture of the humeral capitellum and 3cases combined with posterolateral rotation instability;According to Regan- Morrey classification:Ⅱ type 10cases,Ⅲ type 6cases.Diagnosis by preoperative elbow CT and threedimensional imaging,we accurately knew of fracture position,size of fracture block,the degree of displacement of fracture.With general anesthesia and lateral position,the patients were positioned with limb in the elbow ancon.To applly pneumatic tourniquet inflation pressure band,with the pressure of 240mmHg,tourniquet time 40-90min,average(63.3±25.0)min.Anterolateral approach in the elbow-flexion position and proximal medial approach from the proximal part were used,because:(1)there is safest distance of ulnar nerve and median nerve in anterolateral approach in the elbow-flexion position,it is the safest approach in the medial approach into the road (the distance to the ulnar nerve is 15.5mm,the distance to the median nerve is 13.8mm).(2)there is safest distance(10mm)to radialnerve in the anterolateral approach to,With the advantage of flexible operation and good microscopic field of vision,it is the most safe and effective one of the lateral approachs into the way;(3)We choose the position of 90°elbow flexion position to puncture operation since nerve is away from point of puncture.Usually water injection were operated from the lateral approach establishing arthroscopy channel,cleaning blood stasis and synovial joints of joint,exposing fracture block of coronary,and completing the reduction with arthroscopy.After the satisfied reduction,to fix the fracture from the back to coronary direction with screws or wires.Usually,the appropriate length of hollow screw is 3.0 mm,and the cutting-edge through coronary is not more than 2mm.Also,the needle tail should be placed subcutaneously after bending.To combined fractures,such as capitellum fractures,open reduction and fixation is needed at the same time,including the repair or reconstruction of the lateral collateral ligament when posterolateral rotation unstability occurrs.Elbow should be fixed in a flexion position no less than 1week,then early functional exercise was operated under the guidance of doctor.Results14cases were followed-up,with an average time of 12.6months(8-24months).All the postoperative incision healed good(typeⅠhealing),no incisional drainage,nerve damage and fracture displacement occurs,with 1case of heterotopic ossification.X ray film was applied at the time of terminal follow-up to assess fracture healing,showing fracture clinical healing of all the cases,and the healing time was 10-14weeks,12weeks on average.All patients reached anatomical reduction in the operation.The improved elbow HSS score was an average of 33 (28-35),average score of Visual Analog Scale is 1.2±0.5,with an average of 132.4°of elbow flexion,and 10.6°of elbow straighten,68.5°of pronation,78.6°of supination.the total good and excellent rate was 100%(14/14).Discussion Discuss Elbow joint is is composed of trochlea of humerus and half-month notch of ulna,composed of coronary and olecranon.Ulna coronary is the most important humeral blocking structure in front of elbow,which is an important part preventing elbow dislocation and posteriormedial rotation unstability.There are many important soft tissue attachment points important structures in front of the elbow including the joint capsule,the medial collateral ligament,brachialis,and so on,.It is the main stable structure of elbow,resisting biceps,brachialis and triceps pulling ulna to elbow.Coronary processes is an important part of the anterior column and the medial column,forming a stable ring in front of the elbow.When it damages,elbow medial and front instability may occurs.Improper handling may lead to habitual dislocation.Therefore,in the treatment of ulna coronary fracture,restore or rebuild the height and shape of the coronary and repair or reconstruction the anterior beam of medial collateral ligament is very important.With development of further research of elbow joint,the important role of elbow has been recognized,the fractures usually lead to complex traumatic elbow instability,so the treatment of ulna coronary fracture also attract more and more attention of surgons.When the fracture fragment is large(Regan-MorreyⅡ,Ⅲ),because of the flexor pull leading fracture displacement,elbow instability easily occurs and it is difficult.to manually reduce and maintain the position of fracture.And because the fracture is hard to expose,and fix,especially for small pieces or comminuted fracture of the coronary.Improper treatment may easily causes joint instability,myositis ossificans,traumatic arthritis,stiff joints,etc.Coronary fracture belongs to intra-articular fracture,anatomical reduction and strong internal fixation is the basis of the joint function recovery in the treatment of intra-articular fractures.Anatomical reduction is beneficial to the activities of the joint,relieve joint pain,and prevent the occurrence of traumatic arthritis;Strong internal fixation is beneficial to early functional exercise and prevent the stiffness of the elbow joint,reduce muscle atrophy,and dynamic instability and prevent the occurrence of traumatic arthritis,achieving good function.Ulna coronary fractures often combined with elbow instability,foreign scholars not only reported and discussed the treatment and prognosis,but also put forward the diagnostic criteria and surgical treatment scheme.Domestic scholars have similar report and literature review,introduces the treatment experience,and discuss new approaches and solutions,etc.The main method of fixation are steel wire fixation,kirschnerwire fixation,mini screw internal fixation,mini plate internal fixation and absorbable screw fixation,etc.Open reduction and internal fixation of coronary fracture was operated through theconventional anterior approach,but it is very difficult to coronary reduction and internal fixation,because:(1)the neurovascular structure in front of the elbow closely packed,operation through blood vessels or nerve gap is safe,and the vice injury occures easily;(2)the position of coronary is deep,it is very difficulty to touch the fracture line,because there is a lot of soft tissue,in this case it is difficult to touch the front clear fracture line and clean.If the soft tissue on the coronary was cleaned radically,including the attachment point of the medial collateral ligament,the brachial muscle,and the joint capsule,the meaning of reduction will lose;(3)fragment of coronal fractures tend to be small,the compaction fingers from the anterior part may occupy the fixing position again;(4)surgery of open reduction is a kind of great trauma,easily lead to heterotopic ossification and larger scars left,affecting beautiful appearance.With the deep understanding of the anatomy of elbow function and the improvement of elbow function requirements of patients,and minimally invasive surgery is more and more become a safe and effective treatment of intra-articular fractures.Because arthroscopy surgery has the advantages of little trauma and quick recovery in recent years,the application in the elbow fracture has made rapid progress.In acute elbow trauma,elbow arthroscopy technology can not only clean up small pieces fragment including cartilage ones,but also compete reduction and internal fixation of fracture feasiblly.And radial head fractures,olecranon fractures,coronoid process fractures,humerus condyle fracture reduction and internal fixation were reported.Adams reported 7cases of ulna coronary condyle fracture appling elbow arthroscopy technology for reduction and fixation,final follow-up showed the curative effect is satisfied,with no heterotopic ossification and elbow arthritis.Operation approach of elbow arthroscopy are anterolateral approach and anteromedial approach in the position of elbow flexion.Because:(1)there is safest distance of ulnar nerve and median nerve in anterolateral approach in the elbow-flexion position,it is the safest approach in the medial approach into the road(the distance to the ulnar nerve is 15.5mm,the distance to the median nerve is 13.8mm).(2)there is safest distance(10mm)to radial nerve in the anterolateral approach to,With the advantage of flexible operation and good microscopic field of vision,it is the most safe and effective one of the lateral approachs into the way;(3)We choose the position of 90°elbow flexion position to puncture operation since nerve is away from point of puncture.For Regan- Morrey Ⅱ type comminuted fracture,preoperative CT fully estimated size of fracture block,due to the small fracture fragment,cannulated screws may break down the fracture fragment and the fixing effect is not exact.To prevent this occurs,for Regan-MorreyⅡtype frature.we fix with kirschner wire from the back of the elbow to coronary direction;For Regan-MorreyⅡtype simple fracture and Regan-MorreyⅢtype fracture,if the fragment is large,hollow screws should be used from the back of the ulna to the coronary direction.Compared with other joints,arthroscopy technical of elbow joint requires higher technique.performer must be very familiar with anatomy around the elbow.Because the structure is complex around the elbow joint with a lot of important nerve and blood vessels,although elbow surgery is a kind of effective and minimally invasive treatment,the incidence of complications than knee and shoulder arthroscopy surgery is higher,but the majority are mild reversible disease,and after some measures,these complications can be avoided,so the elbow arthroscopy surgery is a safe and effective technique.In addition,arthroscopic technique can provide better joint vision,less surgical trauma,less postoperative recovery time.Application of elbow arthroscopic technique assisted reduction and fixation in the treatment of ulna coronary fracture has the advantage of small incision,small trauma,good effect,fast recovery,etc.articular surface can be observed directly under arthroscopy,leading anatomicalintra-articular reduction,reducing traumatic arthritis,and can make the complications such as nerve,blood vessel damage to a minimum extent,still can reduce surgical trauma and reduce the complications of elbow injury.But the performer should has rich experience in the microscopic operation and local anatomical knowledge,strictly control the choice of operation indication,in order to avoid the happening of the complications to the maximum extent.
Arthroscopes;Ulna fractures;Surgical procedures,minimally invasive
Xiang Ming,Email:josceph_xm@sina.com
2013-07-19)
(本文编辑:胡桂英)
10.3877/cma.j.issn.2095-5790.2014.03.003
610041 成都,四川省骨科医院上肢科
向明,Email:josceph_xm@sina.com
杨顺,向明,杨国勇,等.肘关节镜辅助下复位固定治疗尺骨冠状突骨折[J/CD].中华肩肘外科电子杂志,2014,2(3):144-150.
猜你喜欢
人人健康(2022年4期)2022-11-25
实用手外科杂志(2022年2期)2022-08-31
昆明医科大学学报(2022年1期)2022-02-28
临床骨科杂志(2021年3期)2021-06-24
医药前沿(2021年8期)2021-06-10
中华肩肘外科电子杂志(2020年1期)2020-12-20
中华肩肘外科电子杂志(2020年1期)2020-08-24
World Journal of Clinical Cases(2020年7期)2020-04-23
中国现代药物应用(2019年24期)2020-01-01
中华肩肘外科电子杂志(2019年4期)2019-08-24
