
Systematic Review of Acupuncture for Functional Constipation
2014-06-19 16:18,
,
1 The Second Clinical Medical School of Nanjing University of Chinese Medicine, Nanjing 210023, China
2 Jiangsu Province Hospital of Traditional Chinese Medicine, Nanjing 210029, China
SYSTEMATIC REVIEW
Systematic Review of Acupuncture for Functional Constipation
Zhang Wei1, Sun Jian-hua2, Pei Li-xia1,2, Wu Xiao-liang2, Chen Lu2, Jiao Dai-yan1
1 The Second Clinical Medical School of Nanjing University of Chinese Medicine, Nanjing 210023, China
2 Jiangsu Province Hospital of Traditional Chinese Medicine, Nanjing 210029, China
Author: Zhang Wei, master degree candidate
Objective: To systematically analyze the therapeutic efficacy and safety of acupuncture in treating functional constipation (FC).
Methods: By searching the Cochrane Library, PubMed, Web of Science, Embase, CBM, CNKI, WanFang databases, the randomized controlled trials (RCTs) comparing acupuncture with Western medication in treating FC were retrieved, from the inception of the databases to September 2013. When the literatures were arranged according to the inclusion and exclusion criteria, and the methodological qualities were evaluated, RevMan 5.2 was adopted for meta-analysis.
Results: Ten RCTs were included, covering 1 041 cases of FC. The meta-analysis showed that there was no significant difference in comparing spontaneous bowel movements per week between shallow acupuncture at Tianshu (ST 25) and Western medication [MD=-0.47, 95% CI (-1.28, 0.34)]; there was a significant difference in comparing the spontaneous bowel movements per week between deep acupuncture at Tianshu (ST 25) and Western medication [MD=0.53, 95% CI (0.13, 0.92)], but the difference was insignificant according to the sensitivity analysis [MD=0.38, 95% CI (-0.03, 0.80)], indicating the low reliability of the conclusion. Regarding the Cleveland clinic score (CCS), the difference between shallow acupuncture at Tianshu (ST 25) and Western medication was insignificant [MD=0.39, 95% CI (-1.13, 1.91)]; the difference between deep acupuncture at Tianshu (ST 25) and Western medication was significant [MD=2.64, 95% CI (1.32, 3.97)]. In the evaluation of security, the incidence rate of adverse events in acupuncture treatment (0.31%) was significantly lower than that in Western medication treatment (3.4%).
Conclusion: Although the present systematic review showed that deep acupuncture at Tianshu (ST 25) should have better therapeutic efficacy than Western medication, the reliability and quality of the evidences were poor, and thus the above results require proving by more RCTs of higher quality.
Acupuncture Therapy; Constipation; Randomized Controlled Trial; System Review
Functional constipation (FC) is a type of gastrointestinal disorder characterized by infrequent bowel movements, hard stools, and difficulty defecating, with physical causes excluded by examinations. A crosssectional survey studied the current status and distribution features of constipation of people over 60 years old[1], showing that the prevalence rate of constipation is 11.5% in people over 60; the prevalence rate in the northern part of China is higher than that in the southern part; females were more easily affected than males; the prevalence rate is increasingwith age. In America, the prevalence rate of constipation is 12%-19%[2]; it’s reached up to 27.2% in Canada[3]. It’s believed that low social status, gender, improper diet, life habits, lack of exercises, and aging are all risk factors for the development of constipation[4-6]. Chronic constipation does not only bring abdominal distention and pain, headache, poor appetite and nausea[7], but also put stress on the heart, easily leading to cardio-cerebrovascular diseases and severely affecting the patient’s quality of life[8-9].
In Western medicine, stimulant, bulk-forming, and osmotic laxatives are often used in treating FC. Regardless of certain treatment effects, long-term use of the above drugs may cause drug dependence, melanosis coli, and laxative-dependent constipation, etc.[10]In foreign countries, many constipation patients turn to acupuncture when they don’t respond to Western medications[11]. Animal experiments have found that acupuncture can improve the colonic transit by ameliorating the rhythm of colonic slow wave and enhancing the positive expression of interstitial cells of Cajal (ICC) in colonic smooth muscle[12-13]. Currently, clinical studies on both acupuncture and Western medication have been increasing. However, the conclusions are varied because of the limitation of sample size and poor methodological quality. Therefore, to objectively evaluate the treatment effect of acupuncture for FC, we adopted the Cochrane review method to evaluate the effectiveness and safety of acupuncture compared with Western medication in treating FC.
1 Materials and Methods
1.1 Inclusion criteria
1.1.1 Study type
Randomized controlled trials (RCTs) comparing acupuncture with Western medication for FC; the generation of random sequence should be clearly described; blinding method is not required; articles written in Chinese or English.
1.1.2 Subject
The age, gender, and source of subjects were not limited; in accordance with the diagnostic criteria of FC.
1.1.3 Intervention
Acupuncture was adopted in the treatment group (acupuncture apparatus, acupoint selection, manipulations, needle-retaining time, and treatment courses were not limited); Western medication was adopted in the control group (the type of medication was not limited).
1.1.4 Parameter
Spontaneous bowel movements per week; Cleveland clinic score (CCS); adverse events.
1.2 Exclusion criteria
Studies that only mentioned randomization but without detailed randomization method; RCTs comparing acupoint injection with medication; for duplicate publications, the one with more rigorous method was chosen; studies with undefined results.
1.3 Search methods
The electronic searches were undertaken of Cochrane Library, PubMed, Web of Sicence, Embase, CBM, CNKI, and WanFang databases from their inception to September 2013. The subject headings and free words were used together for retrieval [Pubmed (MeSH), Embase (EMTREE), CBM (subject headings)] depending on the type of database. The relevant references were all retrieved.
For example, the search of PubMed is as follows: (Constipation or chronic constipation or colon* inerti* or gastrointestinal* motility or colonic motility or intestinal* dysmotility* or functional* colonic* disease*) and [acupuncture or acup* or electroacupuncture (EA) or auricular acupuncture or scalp acupuncture].
1.4 Data collection and extraction
Two independent reviewers read the titles and abstracts. When the obvious ineligible studies were excluded, the rest would be read through the whole article. The indefinite ones were discussed among the reviewers. Data were extracted on details including: title, authors, source, design of the study, method of randomization, allocation concealment, participants, inclusion criteria, exclusion criteria, intervention in the treatment group, intervention in the control group, treatment course, criteria of therapeutic efficacy, and adverse events, etc. When data were extracted, the two reviewers would cross-check the data.
1.5 Evaluation methods
The quality of study was evaluated by using the Cochrane ‘risk of bias’ tool[14]. We selected 6 categories from this tool: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other bias. The studies were scored as low risk of bias, high risk of bias, or unclear. The data were extracted and cross-checked by the review authors independently, and disagreements were solved by discussion.
1.6 Statistical analysis
The extracted data were analyzed by using RevMan 5.2 provided by Cochrane. Chi-square and Ι2testswere used for evaluating the heterogeneity.P>0.10 and Ι2≤50% indicated insignificance of heterogeneity and fixed effects model could be used in this condition;P≤0.10 and Ι2>50% indicated significant heterogeneity and random effects model was adopted according to the subgroup analysis of study design and treatment protocol. Descriptive qualitative analysis was used when there was a clinical heterogeneity or the statistical heterogeneity was too significant. RR and 95% CI were used for measurement of enumeration data, MD for measurement data. When the included studies were sufficient (n≥9), funnel plot was used to determine the publication bias.
2 Treatment Methods
2.1 General condition of included studies
Of the 1 159 extracted studies, 498 were excluded for duplicate publication by using EndNote X6, and 589 studies including review, animal study, or studies with ineligible interventions were excluded. Eightyeight studies were initially included. By further scan, 17 studies were excluded for duplicate publication of candidate dissertation, 2 meta-analysis studies and 59 with improper method of randomization were also excluded. Ten RCTs were finally included. The process and result of data collection are shown in Figure 1.

Figure 1. Data collection
The 10 included studies were all from China, but 8 were written in Chinese[15-22]and 2 in English[23-24]. All of the 10 studies conducted a 4-week treatment, 5 studies performed a follow-up of 1-6 month, and 6 studies respectively compared deep acupuncture and shallow acupuncture at Tianshu (ST 25) with Western medication in treatment of FC[16-21]. The basic characteristics of the included studies are shown in Table 1.
2.2 Evaluation of literature quality
The included 10 RCTs all provided the general data of the subjects and the details of randomization. Six studies used allocation concealment, of which, 5 fused central distribution[16-19,21]and 1 used envelope concealment[22]. Two RCTs used blinding of outcome assessment[19-20], 7 reported dropouts and analyzed the outcome and the missing data[17-21,23-24], and only 1 study did intention-to-treat (ITT) analysis[21]. The evaluation of methodological quality of the included studies is shown in Table 2.
2.3 Meta-analysis results
2.3.1 Spontaneous bowel movements per week
Four studies reported spontaneous bowel movements per week at the end of treatment, and evaluated the therapeutic efficacy according to the changes of spontaneous bowel movements per week. The changes after treatment were calculated by using the Handbook of Cochrane meta-analysis. As the included four studies all had 3 arms, they were analyzed by using sub-group analysis according to the clinical heterogeneity [difference in acupuncture depth at Tianshu (ST 25)]. The meta-analysis showed that there was no significant difference in comparing the change of spontaneous bowel movements per week at the end of treatment between shallow acupuncture and Western medication [MD=-0.47, 95% CI (-1.28, 0.34)]; there was a significant difference in comparing the change between deep acupuncture and Western medication [MD=0.53, 95% CI (0.13, 0.92)] (Figure 2). Therefore, it can be concluded that FC patients intervened by deep acupuncture at Tianshu (ST 25) had better improvement of spontaneous bowel movements per week than those who received Western medication at the end of treatment.
When Wang CW, et al (2010)[21]was excluded, the sensitivity analysis of the rest studies showed that there was no significant heterogeneity in comparing shallow acupuncture with Western medication (P=0.67, Ι2=0), indicating the reliability of the result; in comparing deep acupuncture at Tianshu (ST 25) with Western medication, when Chen L (2010)[17]was excluded, the analysis showed homogeneity among the studies (P=0.72, Ι2=0), and the meta analysis showed that there was no significant difference incomparing the change of spontaneous bowel movements per week [MD=0.38, 95% CI (-0.03, 0.80)] (Figure 3), indicating the low reliability of the conclusion.

Table 1. Characteristics of the included studies
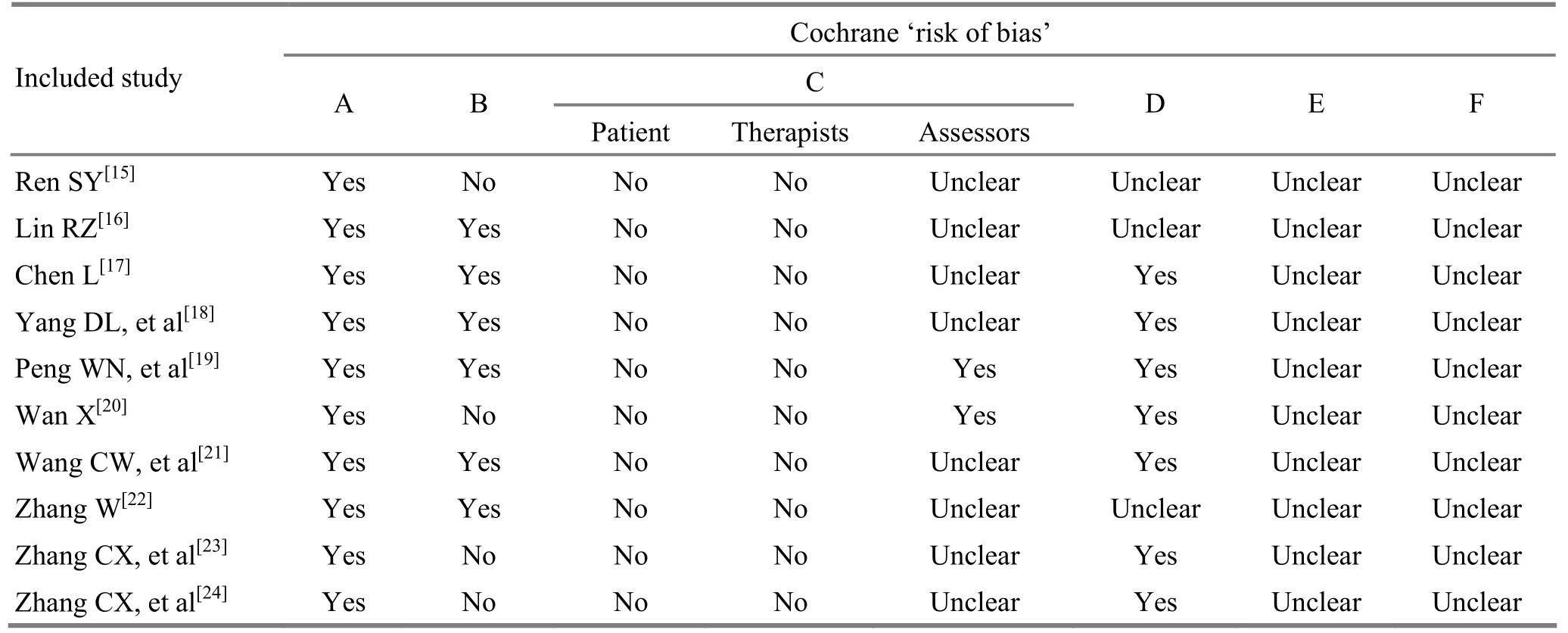
Table 2. Evaluation of the quality of the included studies

Figure 2. Meta-analysis of the changes of spontaneous bowel movements per week
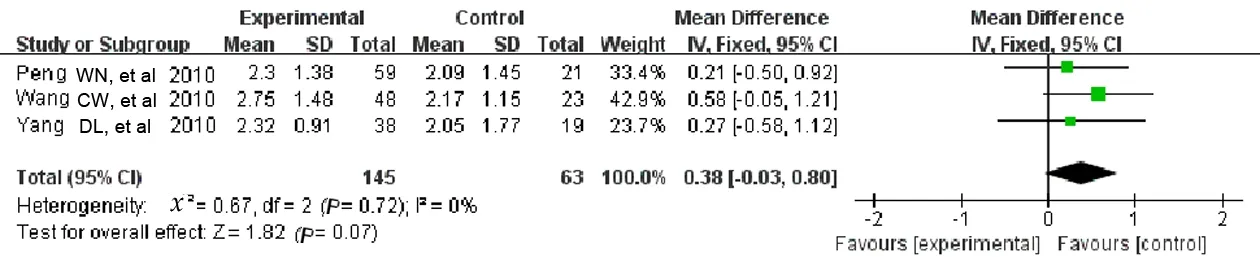
Figure 3. Meta-analysis after Chen L (2010) was excluded
2.3.2 CCS scoring
Six studies compared the CCS between shallow acupuncture at Tianshu (ST 25) and Western medication, and the meta-analysis showed that there was no significant difference in comparing the change of CCS at the end of treatment [MD=0.39, 95% CI (-1.13, 1.91)] (Figure 4). Seven studies compared the CCS between deep acupuncture at Tianshu (ST 25) and Western medication, and the result showed a significant difference in comparing the change of CCS [MD=2.64, 95% CI (1.32, 3.97)] (Figure 4). The sensitivity analysis showed that the combination of effect size was not remarkably influenced by any single study.
2.3.3 Adverse events
Five studies reported adverse events. Of the 638 subjects undergone acupuncture treatment, 2 experienced mild abdominal pain after receiving deep acupuncture; of the 403 who received Western medication, 5 felt abdominal distension and discomfort and 9 had diarrhea. The incidence rate of adverse events of acupuncture treatment (0.31%) was significantly lower than that of Western medication (3.4%).
3 Discussion
3.1 Major findings of the current study
The results showed that there was no significant difference between shallow acupuncture and Western medication in comparing the change of spontaneous bowel movements per week at the end of treatment, indicating that the two therapies should have similar effectiveness; there was a significant difference in comparing the change of spontaneous bowel movements per week between deep acupuncture at Tianshu (ST 25) and Western medication and the improvement in the deep acupuncture at Tianshu (ST 25) group was better than that in the Western medication group, but the sensitivity analysis finally revealed its low reliability. Regarding the evaluation of CCS, compared to Western medication, deep acupuncture at Tianshu (ST 25) can effectively relieve the symptoms of FC patients, while the effect of shallow acupuncture at Tianshu (ST 25) was similar to that of Western medication.

Figure 4. Meta-analysis of changes of CCS
3.2 Evaluation of the methodological quality of the included studies
In this review, 10 RCTs were included, but generally had a low quality. They were scored as low risk of bias on the generation of random sequence as they all described the detailed information; 6 studies adopted allocation concealment, 5 with central distribution and 1 with envelope concealment, thus can effectively control the selection bias. Since the studies only adopted subjective parameters in the evaluation of therapeutic efficacy, the results could be easily influenced by the evaluator of the outcomes. Plus, it’s really not practical to blind the operation to the acupuncture practitioners and subjects. Therefore, the allocation concealment and blinding in the outcome measurement have become very important. Of the included studies, only 2 performed blinding to the outcome evaluators; 7 reported loss to the follow-up, but only 1 study did the ITT analysis of the missing data. Therefore, the outcomes could possibly be mis-evaluated[25]. The evaluations of the outcomes were scored as unclear because the original data were not retrievable; the rest evaluation items were also scored as unclear because the difficulty judging the bias.
3.3 Limitations of the current study
Although our review rigorously followed the method of Cochrane meta-analysis, limitations still exist: the studies were all located in China, and the study designs and sample sizes were rather limited, making the extrapolation and reliability limited; it’s not proper to evaluate the security only from the incidence rate of adverse events, as it’s not sufficient to determine the degree of severity; in consideration of the number of the included studies and the power of test, our review didn’t compare acupuncture with different types of Western medication, but only regarded the Western medications as a whole.
In summary, compared to the Western medicine, deep acupuncture can effectively enhance the spontaneous bowel movements per week and improve the symptoms of FC patients. But, limited by the quality of the included studies and the power of test, this conclusion is not reliable. Therefore, we sincerely suggest that the future clinical studies should strictly conform to the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA), to provide reliable evidences for the treatment of FC.
Conflict of Interest
There is no potential conflict of interest.
Acknowledgments
This work was supported by National Natural Science Foundation of China (No. 30973794 and No.81273839).
[1] Yu PL, Li ZG, Zheng H. The survey of the current status and distribution of elderly constipation in China. Zhonghua Laonian Yixue Zazhi, 2001, 20(2): 132-134.
[2] Eoff JC. Optimal treatment of chronic constipation in managed care: review and roundtable discussion. J Manag Care Pharm, 2008, 14(9): 1-15.
[3] Pare P, Ferrazzi S, Thomapson WG, Irvine EJ, Rance L. An epidemiological survey of constipation in Canada: definitions, rates, demographics, and predictors of health care seeking. Am J Gastroenterol, 2001, 96(11): 3130-3137.
[4] Peters HP, De Vires WR, Vaberge-Henegouwen GP, Akkermans LM. Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. Gut, 2001, 48(3): 435-439.
[5] Talley NJ, Jones M, Nuyts G, Dubois D. Risk factors for chronic constipation based on a general practice sample. Am J Gastroenterol, 2003, 98(5): 1107-1111.
[6] Chang L, Toner BB, Fukudo S, Guthrie E, Locke GR, Norton NJ, Sperber AD. Gender, age, society, culture, and the patient's perspective in the functional gastrointestinal disorders. Gastroenterology, 2006, 130(5): 1435-1446.
[7] Hall GR, Karstens M, Rakel B, Swanson E, Davidson A. Managing constipation using a research-based protocol. Medsurg Nurs, 1995, 4(1): 11-18.
[8] Wald A, Scarpignato C, Kamm MA, Mueller-Lissner S, Helfrich I, Schuijt C, Bubeck J, Limoni C, Petrini O. The burden of constipation on quality of life: results of a multinational survey. Aliment Pharmacol Ther, 2007, 26(2): 227-236.
[9] Dennison C, Prasad M, Lioyd A, Bhattacharyya SK, Chawan R, Coyne K. The health-related quality of life and economic burden of constipation. Pharmaco Economics, 2005, 23(5): 361-476.
[10] Camilleri M, Kerstens R, Rykx A, Vandeplassche L. A placebo-controlled trial of Prucalopride for severe chronic constipation. N Engl J Med, 2008, 358(22): 2344-2354.
[11] van Tilburg MA, Palsson OS, Levy RL, Feld AD, Turner MJ, Drossman DA, Whitehead WE. Complementary and alternative medicine use and cost in functional bowel disorders: a six month prospective study in a large HMO. BMC Complement Altern Med, 2008, 8: 46.
[12] Sun JH, Guo H, Chen L, Wu XL, Li H, Pei LX, Peng YJ, Lu B. Effect of electroacupuncture at “Tianshu” (ST 25) on colonic smooth muscle structure and interstitial cells of Cajal in slow transit constipation rats. Zhenci Yanjiu, 2011, 36(3): 171-175.
[13] Sun JH, Guo H, Chen L, Wu XL, Li H, Pei LX, Peng YJ, Lu B. Effect of electroacupuncture at Tianshu (ST 25) on colonic electromyography in slow transit constipation rats. Zhonghua Zhongyiyao Zazhi, 2011, 26(9): 2077-2079.
[14] Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011.
[15] Ren SY. The clinical observation of electrical-warmed acupuncture with the method of “Shu-Mu point allocation”in treating with slow transit constipation. Chengdu: Master Thesis of Chengdu University of Traditional Chinese Medicine, 2010.
[16] Lin RZ. Clinical study of deep acupuncture at Tianshu (ST 25) for treatment of chronic functional constipation. Nanjing: Master Thesis of Nanjing University of Traditional Chinese Medicine, 2010.
[17] Chen L. A clinical observation on the timeliness of deep acupuncture at Tianshu (ST 25) in the treatment of chronic functional constipation. Nanjing: Master Thesis of Nanjing University of Traditional Chinese Medicine, 2010.
[18] Yang DL, Liu ZS. A clinical observation on deep acupuncture at Tianshu (ST 25) for functional constipation. Beijing Zhongyiyao, 2010, 29(5): 366-368.
[19] Peng WN, Qin PP, Guo J, Liu ZS, Cai HJ, Duan JX, Ni JN, Yang DL, Zhang W. Effect and safety evaluation of deep needle insertion at Tianshu (ST 25) in treating colonic slow transit constipation. Jiangsu Zhongyiyao, 2010, 42(7): 43-45.
[20] Wan X. Observation of long-term therapeutic effect of deep electro-acupuncture at Tianshu (ST 25) for treatment of functional constipation. Nanjing: Master Thesis of Nanjing University of Traditional Chinese Medicine, 2010.
[21] Wang CW, He HB, Li N, Wen Q, Liu ZS. Observation on therapeutic effect of electroacupuncture at Tianshu (ST 25) with deep needling technique on functional constipation. Zhongguo Zhenjiu, 2010, 30(9): 705-708.
[22] Zhang W. Evaluation of therapeutic effect and safety of deep acupuncture at Tianshu (ST 25) for treatment of slow transit constipation. Zhongyi Zazhi, 2006, 47(2): 105-107.
[23] Zhang CX, Qin YM. Study on efficacy and safety of acupuncture for treatment of functional constipation. Shijie Zhenjiu Zazhi, 2010, 20(3): 6-12.
[24] Zhang CX, Guo LK, Guo XF, Li GY, Guo XH. Short and long-term efficacy of combining Fuzhengliqi mixture with acupuncture in treatment of functional constipation. J Tradit Chin Med, 2013, 33(1): 51-59.
[25] Porta N, Bonet C, Cobo E. Discordance between reported intention-to-treat and per protocol analyses. J Clin Epidemiol, 2007, 60(7): 663-669.
Translator:Hong Jue
Sun Jian-hua, professor.
E-mail: drjhsun@sina.com
R246.1
: A
Date:December 15, 2013
 Journal of Acupuncture and Tuina Science2014年2期
Journal of Acupuncture and Tuina Science2014年2期
- Journal of Acupuncture and Tuina Science的其它文章
- Effect of Combined Acupuncture and Shen Zao An Shen Tang on Sleep Quality of Insomnia Patients Due to Deficiency of the Heart and Spleen
- Treatment of Primary Dysmenorrhea with Herbpartitioned Moxibustion plus Ultra-short Wave
- Effect of Moxibustion on the Motility, Absorption and Activities of ATPase in Small Intestine of Spleen-deficiency Rats
- Analysis of the Frequency of Clinical Acupoint Use Based on ‘Traditional Chinese Medical Acupuncture-moxibustion Information Databank’
- Therapeutic Efficacy Observation on Combined Aerobic Exercise with Auricular Point Sticking for Insomnia in College Students
- Effect of Foot Bath and Massage on Insomnia in Patients with Liver Cirrhosis and Investigation of Nursing Satisfaction