
Use of a mouth-facial supportor to facilitate mask ventilation in toothless elderly patients
2013-11-08 03:29LIUSuZHANGXiaoqingLIUJianhuiQINXiaojing
外科研究与新技术 2013年1期
LIU Su,ZHANG Xiao-qing,LIU Jian-hui,QIN Xiao-jing
Department of Anesthesiology,Tongji Hospital,Tongji University School of Medicine,Shanghai 200065,China
Mask ventilation is an important part during the induction of general anesthesia.Difficult mask ventilation is defined as follow:it is not possible for the anesthesiologist to provide adequate face mask ventilation due to one or more of the following problems inadequate mask seal,excessive gas leak,or excessive resistance to the ingress or egress of gas.It is reported that difficult mask ventilation (DMV) due to edentation accounts for 25%-30.6% of the overall DMV rate[1-2].The number of people aged 65 years and above in China has risen to 160 million,or more than 12% of the total population[3].Incomplete dentition,or missing teeth associated with aging,is also becoming a more common physiologic phenomenon.To solve the problem of mask ventilation leakage (MVL)during anesthesia induction,we use a mouth-facial supportor in toothless patients.This study was designed to validate the effectiveness of this mouth-facial supportor in mask ventilation during the induction of general anesthesia.We tested the hypothesis that the mouth-facial supportor used in toothless patients resulted in more effective mask ventilation compared with the toothless patients not veritilated without it.
Materials and methods
This study was approved by the Ethics Committee of Shanghai Tongji Hospital affiliated to Tongji University in Shanghai,China.Written informed consent was obtained from all participants in the study.Subjects were 65 years or older (ASA physical status Ⅱ-Ⅲ),and scheduled for surgeries with general anesthesia.Exclusion criteria were a history of difficult intubation,Mallampati score IV,mouth opening< 1 cm,Thyromental Distance (TMD)<6 cm,abnormal facial anatomy,giant epiglottic cysts and other anatomic abnormalities of the upper airway.
Preoperative medication included intramuscular injection of phenobarbital 100 mg and atropine 0.5 mg(or scopolamine 0.3mg).Dentures were removed before patients were brought into the operating room.Standard ASA monitors were used during anesthesia.Before induction of general anesthesia,the oxygen flow on the anesthesia machine (S/5 Aespire,Detex-Ohmeda,Madison,WI) was set at 3 L/min;the adjustable pressure limit (APL)valve was set at 30 cmH2O;the inspiratory tidal volume was set at 10 ml/kg;and the respiratory rate was set at 15/min.Anesthesia induction was achieved by intravenous injection of midazolam 2 mg,etomidate 0.3 mg/kg,atracurium 0.5 mg/kg and sufentanil 0.5 μg/kg.After the muscle relaxant was given,Intermittent positive pressure ventilation was performed by a male anesthesiologist with 10-years of experience who used a single hand to hold the mask(single-use,cushioned 7000 series face mask(Air Safety Ltd.,Morecambe,Lancashire,England)).
The shape of the mouth-facial supportor was quite similar to commercially available bite-blocks.The modification was expanding the wingspan of a bite-block to 8 cm (Figure 1),which is to be placed between the gum and buccal and the alveolar mucosa to support the cheeks from inside to restore some normal shape of the maxilla and mandibula,therefore improving the seal between the mask and the face.The mouth-facial supportor was custom-made by Jiangyan Medical Instrument Factory,Jiangsu Province,China.
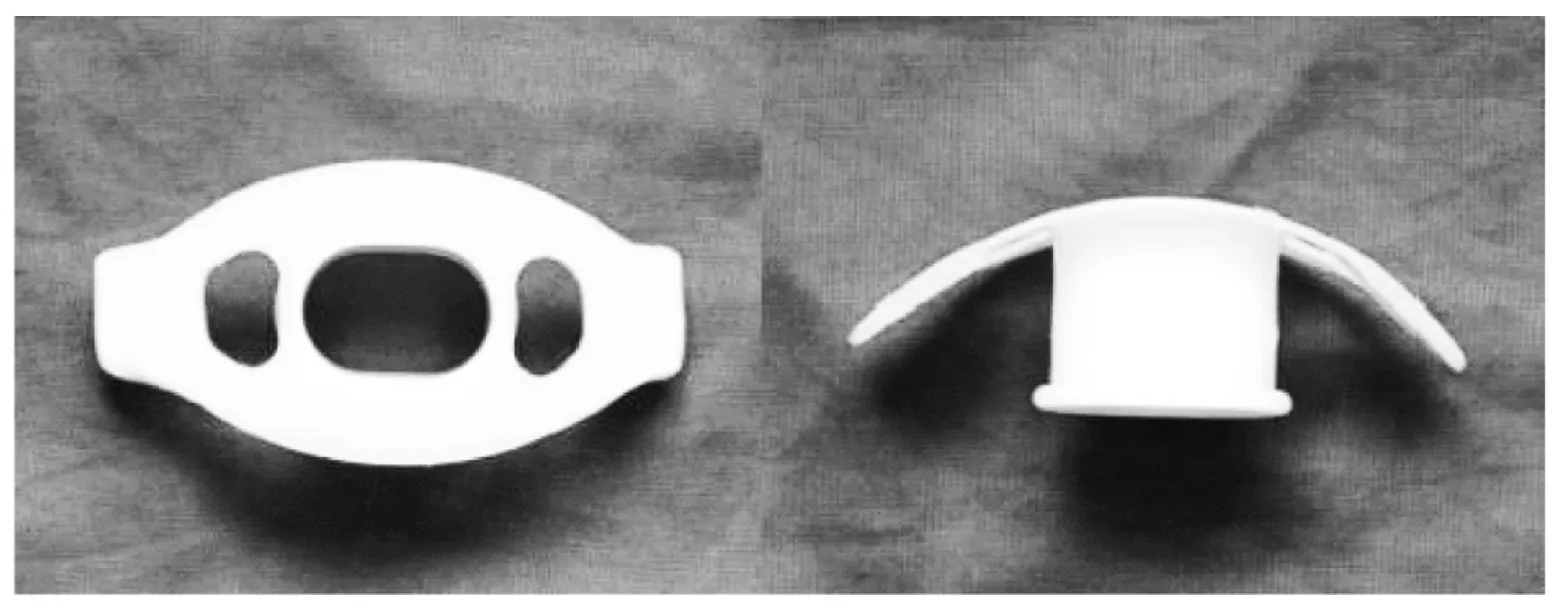
Fig.1 Mouth-facial supportor图1 口面部支撑装置
The toothless patients were assigned randomly to either Group A or B by drawing a number from a sealed envelope prior to induction of anesthesia.Patients in Group A used the mouth-facial supportor during mask ventilation,and those in group B did not use the mouthfacial supportor.The remaining patients who had normal dentition were assigned to Group C.All patients went through the operational process as indicated by the study protocol (Figure 2).After anesthesia induction,the mouth-facial supportor was placed between the lip buccal and alveolar mucosa of the patients in group A,while patients in the other two groups did not use the mouth-facial supportor during mask ventilation.Successful mask ventilation was defined as EtCO2trace reaching 20 mmHg or higher during expiration and then returning back to the baseline during inspiration,when the total fresh gas flow rate was 3 L/min and the APL valve pressure was 30 cmH2O.If mask ventilation was sufficient,it would be maintained for three minutes before tracheal intubation,otherwise a predetermined protocol was followed to ensure adequate mask ventilation,including inserting an oropharyngeal airway,increasing the fresh gas flow to 6L/min,holding the mask with two hands,placing an laryngeal mask airway (LMA)or tracheal intubation or any other emergency measures necessary to maintain patent airway to ensure patient safety.
The volume and rate of MVL:The MVL volume was expressed by the difference between the set tidal volume and actual expiratory tidal volume,and MVL rate was calculated using the following equation:
MVL rate=(MVL volume/ set tidal volume)×100%
Data are expressed as mean ± SD ()and statistically analyzed using SPSS14.0.Single-factor analysis of variance was used to compare continuous variables.Chi-square test was used for categorical data.Data were considered statistically significant when P<0.05.
Results
Of a total of 186 patients evaluated,116 patients were toothless (60 patients were assigned to Group A,while 56 patients were assigned to Group B).Group There was no significant difference in age,gender,body mass index (BMI),snoring,mouth opening and TMD between the three groups (Insee Table 1 here).
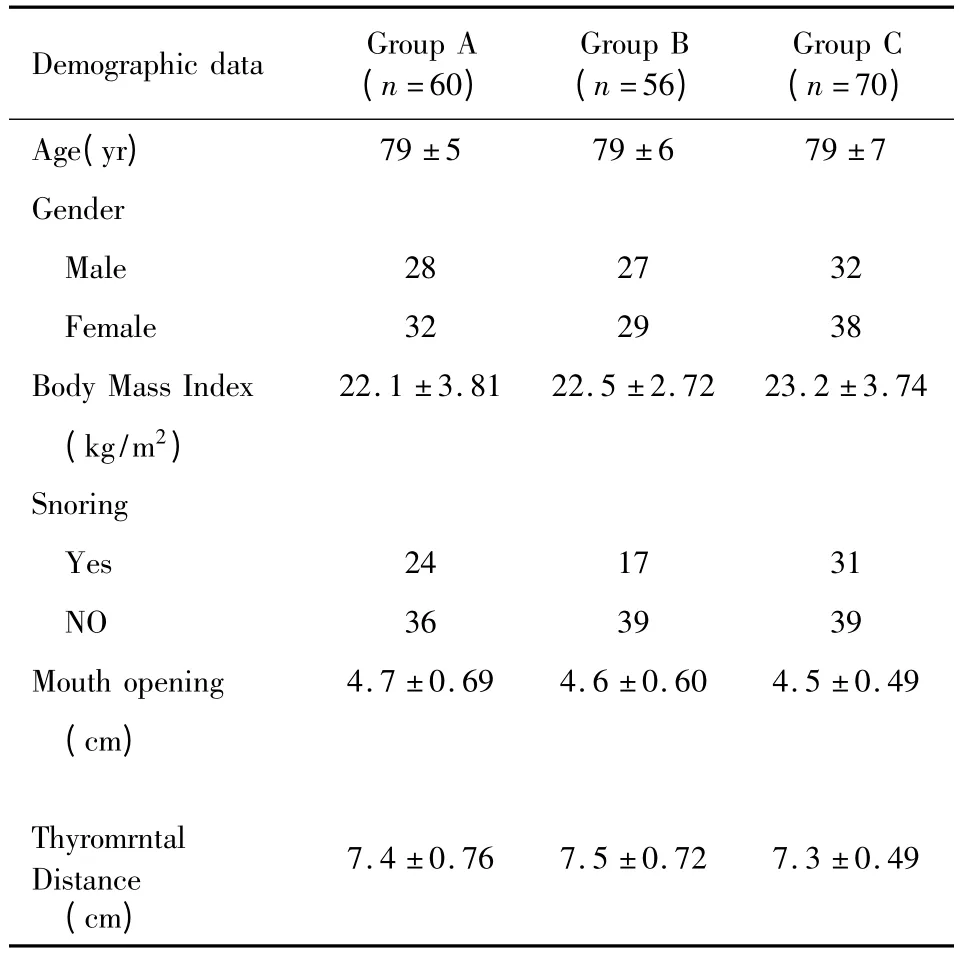
Tab.1 Characteristics of patients表1 患者资料
The success rate of mask ventilation were 83.3%(50/60),17.9% (10/56)and 75.7% (53/70)for Group A,B and C,respectively.Addition of an oropharyngeal airway or increasing the oxygen flow rate significantly increased the success rate of mask ventilation in Group A and C compared to that in group B (P<0.05),while there was no significant difference between Group A and C.There was no significant difference in the success rate of two-hand holding mask ventilation among three groups (Insee Table 2 here).However,there were five patients in Group B that failed to achieve sufficient mask ventilation even with twohand holding mask ventilation;emergency tracheal intubation had to be performed in those patients.
Both MVL volume and rate in Group B were higher than those in Group A or C during induction(P<0.05),while there was no significant difference between Group A and C (Insee Table 3 here).
Discussion
Mask ventilation is an important step during induction of general anesthesia.Insufficient mask ventilation could cause hypoxia,hypercapnia,and may contribute to patient death.
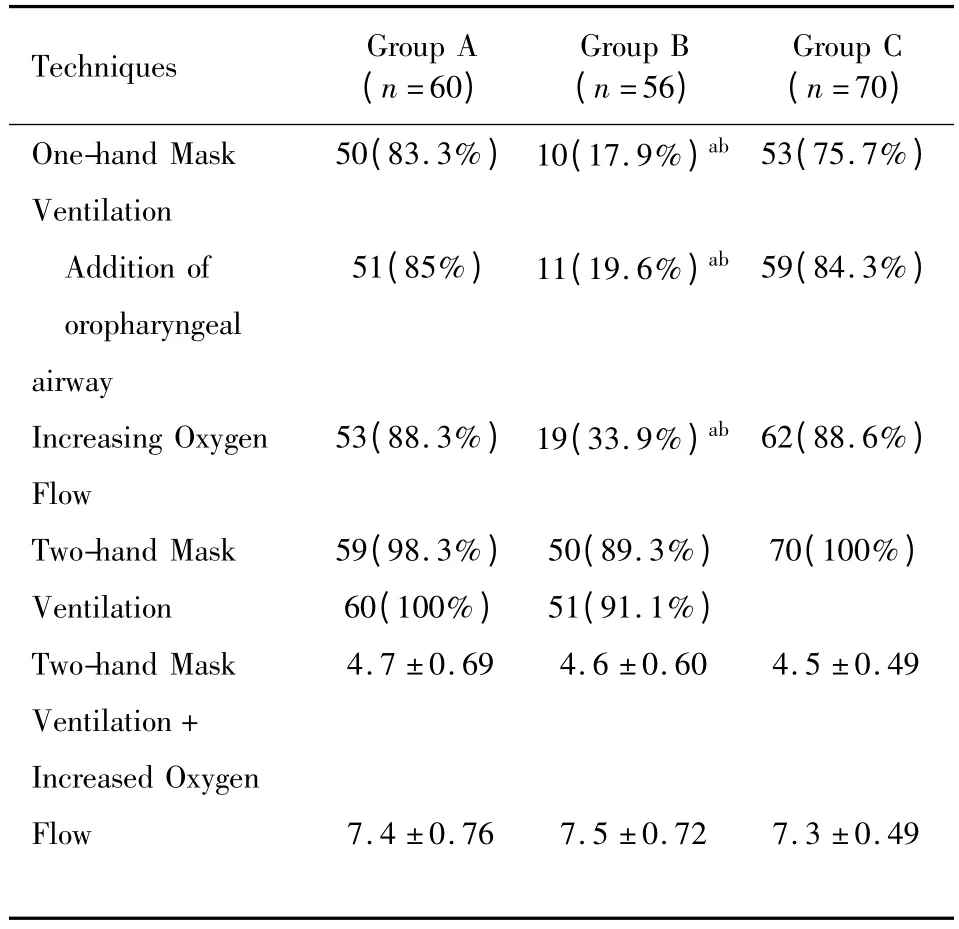
Tab.2 Success rates of the three groups表2 三组患者通气成功率
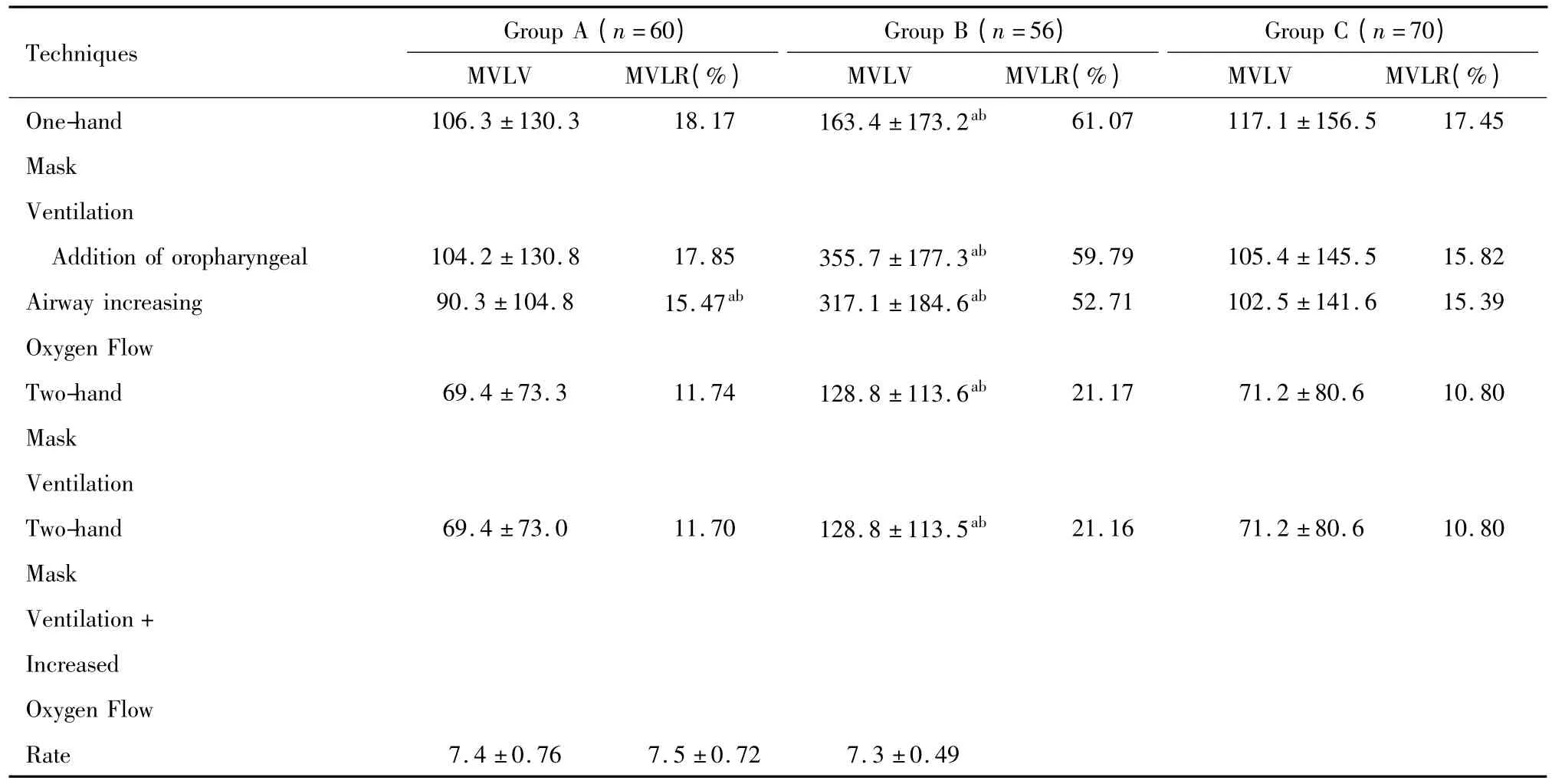
Tab.3 Mask ventilation leakage volumes and rates of the three groups表3 三组患者漏气量及漏气率
The reason for edentulism causing insufficient mask ventilation is mainly due to loss of vertical dimension of occlusion[5].The changes include gingival recession,decrease in subcutaneous tissue,increase in skin wrinkles,downward fall of the mouth corners,and protrusion of the zygomatic and mental processes.All these changes may prevent close contacts between the mask and the face,resulting in MVL (Figure 3).In addition,anesthetics and muscle relaxants induce posterior displacement of the tongue and soft palate relaxation,and the resulting airway obstruction can further aggravate DMV.The notion that closer contact between the mask and the patient’s face may improve mask ventilation led us to modify a bite-block to be used in toothless patients.The elongated front piece of the mouth-facial supportor is placed between the lip and the gums supporting the cheeks to restore some degree of facial contour and to improve the seal between the mask and the face (Figure 4).The mouthfacial supportor can be used along with an oropharyngeal airway to prevent airway obstruction due to posterior displacement of the tongue.Our study demonstrated that the mouth-facial supportor was able to increase the success rate of mask ventilation significantly and improve mask ventilation effectively in toothless elderly patients.

Fig.3 Before the placement of mouth-facial supportor图3 放置口面部支撑器前
Fig.4 After the placement of mouth-facial supportor图4 放置口面部支撑器后
Some of previously reported solutions for edentiainduced MVL were packing gauze around the mask,keeping dentures in place[5-6],and using a chin strap to provide a better seal during mask ventilation in edentulous patients[7],each with limited success.Conlon et al[8]reported that retaining dentures increased success rate of mask ventilation from 49% to 74% during anesthesia induction.But their technique may carry some risks,such as difficulty in removing dentures,the denture falling off,the denture becoming dislodged the airway or esophagus,and damaging dentures or teeth during tracheal intubation.Damage to the teeth is one of the most commonly reported adverse incidents in anesthesia.Damage to the endotracheal tube balloon or laryngeal mask airway is another risk reported[9],which can cause ventilation leakage,aspiration,and other complications.Our mouth-facial supportor alleviates some of the risks associating with retaining dentures.It is convenient to place and remove,less likely to obstruct the airway,and has no risk of damaging a patient’s dentures.Racine et al[10]used the lower lip placement to reduce airleak in edentulous patients,and found that reduced the air leak by 95%.But they also mentioned that it uras difficult to maintain adequate seal with only one hand,so this process needs two-hand technique.While using the bite-block we can increase the success rate to 83.3%with single hand,because the wingspans of the mouthfacial supportor were expanded to 8 cm so that it won’t move when the mask ventilation wiss performed with single hand.
Our results also shows that the success rate of single-hand mask ventilation in toothless elderly patients wiss only 17.9%,which wiss lower than 49%reported by Conlon.One possible reason of the disparity may be due to the fact that part of the patients in Conlon’s study were not completely edentulous patients.The left teeth may facilitate the mask ventilation.The fact that our mouth-facial supportor increased the success rate of mask ventilation in toothless patients to 83.3%,which is higher than the success rate of 75.7% in patients with normal dentition,and which is comparable to the success rate of 89.3% with two-hand ventilation,the fact mentioned above suggests our mouth-facial supportor might be a useful tool in improving mask ventilation in toothless patients.
There are limitations in our study.Our study did not include elderly patients between toothless and with normal dentition,because the left teeth may effect the placement of this mouth-facial supportor.For patients who still have some teeth,retaining denture in place during anesthesia induction may be a better choice[9].
In summary,the success rate of one-hand mask ventilation by an experienced anesthesiologist with oxygen flow rate at 3L/min and a pressure at 30 cmH2O,in toothless elderly patients was only 17.9%.Our mouth-facial supportor was able to raise the success rate of mask ventilation in those patients to a level comparable to that in patients with normal dentition.Thus our customized bite-block can reduce MVL in toothless elderly patients,improve the efficiency of mask ventilation and may improve safety during anesthesia induction.
We thank Jian Hang,MD,PhD,Professional Anesthesia Consultants,LLP,for guidance with revising our manuscript.
[1]Yildiz TS,Solak M,Toker K.The incidence and risk factors of difficult mask ventilation[J].J Anesth,2005,19(1):7-11.
[2]Langeron O,Masso E,Huraux C,et al.Prediction of Difficult Mask Ventilation[J].Anesthesiology,2000,92(5):1229-1236.
[3].Kincannon CL,He W,West LA.Demography of Aging in China and the United States and the Economic Well- Being of their Older Populations[J].J Cross Cult Gerontol,2005,20:243-255.
[4]Sutton DN,Lewis BRK,Patel M,et al.Changes in facial form relative to progressive atrophy of the edentulous jaws[J].International journal of oral&maxillofacial surgery,2004,33(7):676-682.
[5]Hazen SE,Larsen PD,Martin JLH.General anesthesia and elderly surgical patients[J].AORN,1997,65(4):815-822.
[6]Stevenson Judy.When the trauma patient is elderly[J].Journal of PeriAnesthesia Nursing,2004,19(6):392-400.
[7]Farrero Eva,Prats Enric,Manresa Frederic,et al.Outcome of non- invasive domiciliary ventilation in elderly patients[J].Respiratory Medicine,2007,101(6):1068.
[8]Conlon NP,Sullivan RP,Herbison PG,et al.The effect of leaving dentures in place on bag-mask ventilation at induction of general anesthesia[J].Anesthesia & Analgesia,2007,105 (2):370-373.
[9]Shah T,Jones N.Well-fitting dentures:friend or foe?[J].Anaesthesia,2004,59(9):921-922.
[10]Racine SX et al.Face mask ventilation in edentulous patients:a comparison of mandibular groove and lower lip placement[J].Anesthesiology.2010,112(5):1190-1193.
猜你喜欢
当代水产(2022年6期)2022-06-29
中国生殖健康(2020年8期)2021-01-18
中华养生保健(2020年3期)2020-11-16
幼儿教育·父母孩子版(2020年2期)2020-05-12
学生天地(2019年29期)2019-08-25
国际呼吸杂志(2019年8期)2019-04-29
国际呼吸杂志(2019年5期)2019-03-30
中国生殖健康(2018年3期)2018-11-06
通信电源技术(2018年3期)2018-06-26
海峡姐妹(2015年5期)2015-02-27
