蛋白C和抗凝血酶Ⅲ检测对老年心房颤动患者口服华法令出血和血栓并发症诊断的意义
2013-08-20 05:47:36杨发满敬泽慧
中国实验诊断学 2013年5期
杨发满,敬泽慧,刘 冀,田 颖
(1.青海大学附属医院 老年病科,青海 西宁 810001;2.首都医科大学附属北京朝阳医院心脏中心,北京 100020)
蛋白C和抗凝血酶Ⅲ检测对老年心房颤动患者口服华法令出血和血栓并发症诊断的意义
杨发满1,敬泽慧1,刘 冀1,田 颖2
(1.青海大学附属医院 老年病科,青海 西宁 810001;2.首都医科大学附属北京朝阳医院心脏中心,北京 100020)
目的 分析血浆蛋白C、抗凝血酶Ⅲ以及常规凝血指标在口服华法令导致出血和血栓等并发症中的诊断意义。方法选取来我院治疗的98例老年心房颤动患者,取静脉血浆,PC采用凝固法,ATⅢ采用发色底物法,检测两组人群中血浆PC、ATⅢ以及PT、APTT、TT、FIB、D-二聚体水平。结果口服华法令后,89例有出血表现的患者中,59例符合DIC诊断标准,并伴随PC、ATⅢ明显降低和D-二聚体升高;其他30例出血患者中有明显PT、APTT延长,但PC、ATⅢ仍在参考值,PLT、PC、ATⅢ检测结果与诊断DIC组相比有统计学差异(P<0.05)。此外,PC、ATⅢ水平与纤溶及DIC病情程度负相关(P<0.05)。结论通过结合PC、ATⅢ以及常规凝血指标检查,可以为临床早期诊断提供参考
蛋白C;抗凝血酶Ⅲ;心房颤动;华法令
(ChinJLabDiagn,2013,17:0835)
心房颤动是常见的心律失常之一,多发于老年患者。据统计,59岁-70岁心房颤动的发病率约为2%,81岁-90岁为10%。目前心房颤动临床上多选用抗凝药物进行治疗,华法令是临床上治疗心房颤动常用口服药,但是该药存在出血和形成血栓等并发症。如何早期诊断口服华法令并发DIC以及纤溶亢进的患者,对节约治疗成本、提高治疗效果有着重要意义。血浆蛋白C和抗凝酶是体内重要的抗凝物质,在防止机体血栓形成、维持抗凝和凝血平衡方面有着重要作用。本研究通过对老年患者口服华法令时血浆蛋白C(PC)、抗凝血酶Ⅲ(ATⅢ)进行活性检测,同时对D-二聚体以及其他凝血指标进行检测分析,探讨其在华法令治疗导致出血和血栓等并发症中的诊断意义,现报道如下。
1 资料与方法
1.1 一般资料选取2007年8月-2012年8月来我院治疗的98例老年心房颤动患者,其中男性57例,女性41例;年龄58-79岁,平均年龄68.34±10.78岁;所有患者心电图检查确诊为心房颤动[1],67例为永久性心房颤动,31例为持续性心房颤动;其中合并高血压38例、合并2型糖尿病29例、合并缺血性脑卒中20例、合并暂时性脑缺血发作11例;所有患者均口服华法令抗凝治疗。
1.2 方法两组人群均于清晨空腹肘部静脉取血1.5ml,放入试管中,用3.8%枸橼酸钠1∶9抗凝,30min内在4℃下离心(1 500r/min×15min),取血浆分装,在-80℃冰箱中保存,备用[2]。PC、ATⅢ均采用全自动血凝仪进行检测,其中PC采用凝固法,ATⅢ采用发色底物法,试剂盒均购于USCMLIFE公司,所有操作均严格按照试剂盒说明书进行。同时测定患者凝血酶原时间(PT)、部分凝血酶原时间(APTT)、凝血酶时间(TT)、血浆纤维蛋白原含量(FIB)和D-二聚体含量。
1.3 统计学分析所有数据均采用SPSS 20.0统计软件分析,计量指标以均数(±s)表示,组间比较采用两独立样本t检验,多组间比较采用方差分析,P<0.05表示差异有统计学意义。
2 结果
2.1 患者出凝血相关指标分析
98例用药患者中,有9例没有出血症状,其中4例为PT、APTT延长,并伴随FIB下降;89例有出血表现的患者中,59例符合DIC诊断标准,并伴随PC、ATⅢ明显降低和D-二聚体升高;其他30例出血患者中有明显PT、APTT延长,但PC、ATⅢ仍在正常值,这提示患者主要存在以纤溶为主的凝血机制障碍,其血小板计数(PLT)、PC、ATⅢ检测结果与诊断DIC组相比有统计学差异(P<0.05),见表1。
表1 口服华法令患者出凝血相关指标检测结果对比(±s)

表1 口服华法令患者出凝血相关指标检测结果对比(±s)
注:有出血症状患者中,PLT、ATⅢ、PC与无DIC组间相比,▲P<0.05(t=2.634);▼P<0.05(t=1.988);★P<0.05(t=2.002)
组别 例数 PLT(109/L)PT(INR)APTT(s)TT(s)FIB(g/L)ATⅢ(mg/L)PC(mg/L)D-二聚体(mg/L)无出血症 有DIC 0 0 0 0 0 0 0 0 0状患者 无 DIC 9 22.67±17.98 1.19±0.48 39.78±16.69 19.68±7.12 2.48±0.58 301.31±61.34 27.95±6.32 1.23±0.36有出血症 有DIC 59 5.98±8.01▲ 2.75±1.20 67.50±21.50 31.00±4.98 1.30±1.15 152.00±38.50▼ 7.89±4.94★ 3.62±0.58状患者 无 DIC 30 18.95±13.04 2.15±0.82 59.27±15.73 42.37±16.21 0.73±1.92 289.03±46.35 26.24±9.572.21±0.83
2.2 口服华法令患者检测结果与治疗分析
根据研究结果可以发现,PC、ATⅢ水平与纤溶及DIC病情程度负相关,见表2;随着治疗不断进行,PC、ATⅢ水平不断降低,因此可以针对有出血的患者,改变治疗方案,改善凝血指标。
表2 口服华法令患者治疗前后PC、ATⅢ测定结果对比(±s)
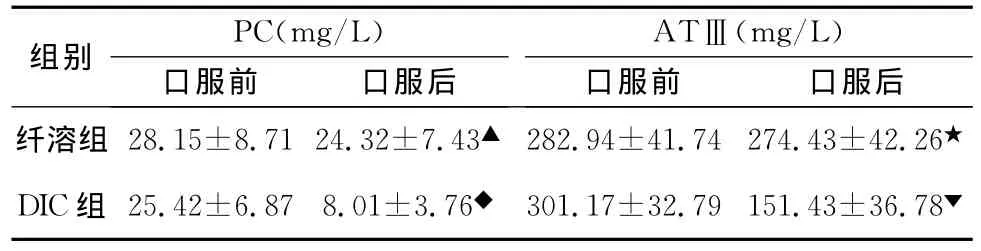
表2 口服华法令患者治疗前后PC、ATⅢ测定结果对比(±s)
注,与口服华法令前相比,▲P<0.05(t=2.614),★P<0.05(t=2.134),◆P<0.05(t=2.325);▼P<0.05(t=3.561);
组别 PC(mg/L)ATⅢ(mg/L)口服前 口服后纤溶组 28.15±8.71 24.32±7.43▲ 282.94±41.74 274.43±42.26口服前 口服后★DIC组 25.42±6.87 8.01±3.76◆ 301.17±32.79 151.43±36.78▼
3 讨论
华法令治疗心房颤动的疗效毋庸置疑,但存在出血和血栓并发症发生率高等问题,影响了患者的用药依从性[3],患者年纪越大,引起缺血性脑卒中的风险也越高,发生出血或血栓的可能性也越大[4],但即使如此,临床上华法令治疗心房颤动依然是无可替代的。国外学者[5]对比阿司匹林联合氯吡格雷与华法令预防房颤患者血栓发生率的疗效,结果发现华法令显著优于阿司匹林联合氯吡格雷。目前认为[6]在使用华法令时及时诊断血栓和出血等并发症,并提前预防和治疗是预防华法令不良反应的最佳方式。
PC、AT是人体内两种抗凝物质,在防止机体血栓形成、维持抗凝和凝血平衡方面有着重要作用。PC系统主要调节血液凝固,防止血栓形成[7],其中,PC是核心环节。PC是维生素K依赖性蛋白,通过灭活凝血因子Ⅹ和凝血酶发挥抗凝作用[8]。AT在内皮细胞中合成,通过抑制凝血酶和凝血因子Ⅸ、Ⅹ、Ⅺ、Ⅻ发挥作用。研究发现[9],AT 可以灭活50%-65%的凝血酶。当体内AT水平低下时,可以导致凝血酶灭活减少,机体凝血功能亢进形成血栓,因此AT是反映凝血酶形成的重要指标[10]。
本研究显示,口服华法令后,89例有出血表现的患者中,59例符合DIC诊断标准,并伴随PC、ATⅢ明显降低和D-二聚体升高;其他30例出血患者中有明显PT、APTT延长,但PC、ATⅢ仍为正常值,提示患者主要存在以纤溶为主的凝血机制障碍,其血小板计数(PLT)、PC、ATⅢ检测结果与诊断DIC组相比有统计学差异(P<0.05)。此外,PC、ATⅢ水平与纤溶及DIC病情程度负相关,因此可以针对有出血的患者,改变治疗方案,改善凝血指标。
综上所述,通过结合PC、ATⅢ以及常规凝血指标检查,可以为临床早期诊断提供参考。
[1]Van Walderveen MC,Berry LR,Chan AK et al.Effect of covalent antithrombin-heparin on activated protein C inactivation by protein C inhibitor[J].The Journal of Biochemistry,2010,148(2):255.
[2]Van Walderveen MC,Berry LR,Chan AK et al.Effect of covalent antithrombin-heparin on activated protein C inactivation by protein C inhibitor[J].The Journal of Biochemistry,2010,148(2):255.
[3]Zhu T,Ding Q,Bai X et al.Normal ranges and genetic variants of antithrombin,protein C and protein S in the general Chinese population.Resultsof the Chinese Hemostasis Investigation on Natural Anticoagulants Study I Group[J].Haematologica,2011,96(7):1033.
[4]El Beshlawy A,Alaraby I,Abou Hussein et al.Study of protein C,protein S,and antithrombin III in newborns with sepsis[J].Pediatric critical care medicine,2010,11(1):52.
[5]Tientadakul P,Chinthammitr Y,Sanpakit K et al.Inappropriate use of protein C,protein S,and antithrombin testing for hereditary thrombophilia screening:an experience from a large university hospital[J].International journal of laboratory hematology,2011,33(6):593.
[6]Furugohri T,Sugiyama N,Morishima Y et al.Antithrombin-inde-pendent thrombin inhibitors,but not direct factor Xa inhibitors,enhance thrombin generation in plasma through inhibition of thrombin-thrombomodulin-protein C system[J].Thrombosis and Haemostasis,2011,106(6):1076.
[7]Van Walderveen MC,Berry LR,Atkinson HM et al.Covalent antithrombin-heparin effect on thrombin-thrombomodulin and activated protein C reaction with factor V/Va.[J].Thrombosis and Haemostasis,2010,103(5):910.
[8]D.E.LaCroix,M.Anand.A model for the formation,growth,and dissolution of clots in vitro.Effect of the intrinsic pathway on antithrombin III deficiency and protein C deficiency[J].International journal of advances in engineering sciences and applied mathematics,2011,3(1/4):93.
[9]Sask KN,Berry LR,Chan AKC,et al.Modification of polyurethane surface with an antithrombin-heparin complex for blood contact:Influence of molecular linker/spacer[J].Langmuir,2012,28(4):2099.
[10]Said JM,Ignjatovic V,Monagle PT et al.Altered reference ranges for protein C and protein S during early pregnancy:Implications for the diagnosis of protein C and protein S deficiency during pregnancy[J].Thrombosis and Haemostasis,2010,103(5):984.
The diagnostic significance of Protein C and antithrombinⅢdetection of warfarin in patients with hemorrhage and throm- bosis in elderly atrial fibrillation
YANGFa-man,GUOZe-hui,LIUYi,etal.(1.AffiliatedHospitalofQinghaiU-niversityGeriatricsDepartmentQinghaiXining810001,China;2.CapitalMedicalUniversity,BeijingChaoyang Hospital,HeartCenter)
ObjectiveAnalysis of diagnostic significance of plasma protein C,antithrombinⅢin oral warfarin lead to hemorrhage and thrombosis.MethodsSelected from our hospital treatment of 98cases of elderly patients with atrial fibrillation patients as the observation group,PC by coagulation method,ATⅢby chromogenic substrate method,detect two groups of plasma PC,AT Ⅲand PT、APTT、TT、FIB、D-dimer level.ResultsThe observation group PC lower than that of the control group,two groups compared with statistical difference(P<0.05);in addition,the observation group of antithrombin III is lower than that of the control group,the two groups had significant difference(P<0.05).ConclusionDetection of plasma protein C and thrombin III can be used as the early clinical diagnosis standard,to provide an objective basis for the further treatment.
PC;ATⅢ;Atrial fibrillation;Warfarin
R541.7
A
1007-4287(2013)05-0835-03
国家自然科学基金(81100125)
杨发满(1963-),男,副主任医师,硕士,研究方向:老年血液病学。
book=837,ebook=411
2013-02-18)
猜你喜欢
成都医学院学报(2021年2期)2021-07-19 08:35:20
海峡姐妹(2020年9期)2021-01-04 01:35:36
中华养生保健(2020年7期)2020-11-16 01:14:16
天然产物研究与开发(2018年10期)2018-11-06 07:43:50
米娜·女性大世界(2016年9期)2016-12-02 19:13:48
现代检验医学杂志(2016年2期)2016-11-14 02:38:00
健康必读(2015年11期)2015-12-04 18:54:54
中国生化药物杂志(2015年4期)2015-07-07 12:06:05
现代医药卫生(2014年18期)2014-03-11 19:33:16
食品工业科技(2014年5期)2014-03-11 18:14:18