肾上皮样血管平滑肌脂肪瘤的诊治
2013-06-09 15:37:51
中国癌症杂志 2013年3期
中国医学科学院肿瘤医院,肿瘤研究所,泌尿外科,北京 100021
肾上皮样血管平滑肌脂肪瘤的诊治
石泓哲 李长岭 寿建忠 王栋 管考鹏 韩苏军 温力
中国医学科学院肿瘤医院,肿瘤研究所,泌尿外科,北京 100021
背景与目的:肾上皮样血管平滑肌脂肪瘤自2004年起被WHO单独分类在肾脏肿瘤中,但其真正的生物学行为仍不清楚。本研究探讨肾上皮样血管平滑肌脂肪瘤的临床病理特征、诊断治疗及预后。方法:选择本院诊治的肾上皮样血管平滑肌脂肪瘤患者7例。男性3例,女性4例。中位年龄28(23~55)岁。有首发症状4例,体检发现3例。4例肿物局限于肾内,1例侵犯肾盂并侵犯肾静脉形成静脉瘤栓,1例同时发现腹膜后淋巴结转移,1例侵犯肾盂并同期发现肝多发转移和肺多发转移。术前诊断肾癌5例,诊断少脂肪血管平滑肌脂肪瘤2例。行根治性肾切除术5例,行肾部分切除术2例。结果:肿瘤假包膜均不明显,大体标本测量最大径2.5~14 cm,中位最大径5 cm。肿物切面质硬,多结节状,灰白至灰黄红色,有向肾周脂肪浸润性生长倾向,2例浸润腰大肌,2例浸润肾盂,1例形成肾静脉瘤栓,1例肾周淋巴结转移。7例镜下均见到特征增生的上皮样细胞;病理免疫组化染色后均表现黑色素细胞标志物HMB45、Melan-A强阳性,平滑肌细胞标志物SMA弱阳性,上皮细胞标志物CK阴性。病理诊断为上皮样血管平滑肌脂肪瘤。术后患者随访3~36个月,中位随访12个月,7例患者目前均存活。4例复诊未发现复发及转移征象。2例术后出现远处转移并行手术切除。1例术前发现肝、肺多发转移患者接受舒尼替尼靶向治疗3个月后,疗效评价部分缓解(PR),继续治疗3个月后肿瘤进展,疗效评价为疾病进展(PD)。结论:肾上皮样血管平滑肌脂肪瘤临床和影像学表现不典型,需要和肾癌及少脂肪血管平滑肌脂肪瘤鉴别。病理免疫组化黑色素细胞标志强阳性为特征表现。手术为主要治疗方法,术后有复发和转移可能。手术和靶向治疗可能成为转移灶的有效治疗手段。
肾肿瘤;上皮样血管平滑肌脂肪瘤;靶向治疗
肾上皮样血管平滑肌脂肪瘤来源于肾脏间叶组织,根据2004年WHO的分类,肾上皮样血管平滑肌脂肪瘤被单独分类在肾脏肿瘤中。大约1/3的上皮样血管平滑肌脂肪瘤可以发生局部复发或远处转移[1],但其真正的生物学行为仍不清楚,仅根据临床表现和影像特征容易误诊为肾细胞癌或肾血管平滑肌脂肪瘤。上皮样血管平滑肌脂肪瘤的免疫组化有特征性,表现为如HMB45、melanin等黑素细胞标志和平滑肌标志特征染色呈阳性,而上皮细胞的特征染色为阴性。根据免疫组化染色可以区分肾上皮样血管平滑肌脂肪瘤与肾血管平滑肌脂肪瘤和肾细胞癌。本研究对中国医学科学院肿瘤医院2009年2月—2012年9月收治的7例肾上皮样血管平滑肌脂肪瘤进行病例总结和分析。
1 资料和方法
1.1 临床资料
7例患者中,男性3例,女性4例。中位年龄28(23~55)岁。首发症状表现为血尿2例,上腹部不适2例,2例在首发症状后出现患侧腰痛的伴随症状。无首发症状,常规体检发现3例。7例均没有结节硬化病史。
1.2 方法
1.2.1 影像学诊断
患者术前均接受超声、CT和双肾MRI检查。肿物CT测量最大径3~13 cm,中位最大径4.6 cm。超声为低回声或稍高回声肿物。肿物在CT和MRI中均表现为分叶状或不规则形,增强后中等不均匀强化,静脉期肿物强化略低于肾实质,未测得明确脂肪密度。1例可见粗大钙化,余6例未见明显钙化。4例肿物局限于肾内,1例侵犯肾盂并侵犯肾静脉形成肾静脉瘤栓,1例出现腹膜后淋巴结肿大,1例侵犯肾盂并同期发现肝、肺多发转移。术前根据影像学和临床表现诊断肾癌5例,诊断少脂肪血管平滑肌脂肪瘤2例。
1.2.2 手术治疗
术前诊断为肾癌5例因肿瘤较大均行根治性肾切除术。术前诊断为少脂肪血管平滑肌脂肪瘤2例均行肾部分切除术。术中7例肿瘤均与肾周脂肪粘连紧密,2例术前有腰痛主诉者,肿瘤与腰大肌紧密粘连,部分侵犯腰大肌。1例术中证实有肾门淋巴结转移并完整切除肿大淋巴结。患者住院时间15 d~34 d,中位住院时间18 d。
1.2.3 术后病理诊断
手术切除的标本,经4%甲醛固定。常规石蜡包埋,切片。HE染色,光镜观察。选用HMB45、Melan-A、SMA、S100、Vim、CDl0、EMA、CK、CK7、CK8、CK18和Ki-67等标志物抗体进行免疫组织化学染色。
1.2.4 疗效评价及随访
术后1年内常规每3个月随访1次,之后每6个月复查1次。复查常规行胸片、腹部及泌尿系超声检查,每6~12个月或必要时行胸部或腹部CT检查。对转移患者治疗中应用实体瘤评价标准(RECIST)评价疗效。疗效评价分为完全缓解(CR)、部分缓解(PR)、疾病稳定(SD)和疾病进展(PD)。
2 结 果
2.1 病理诊断结果
肿瘤假包膜均不明显,与肾组织无明显分界,大体标本测量最大径2.5~14 cm,中位最大径5 cm。肿物切面质硬,多结节状,灰白至灰黄红色,有向肾周脂肪浸润性生长倾向,1例侵犯腰大肌及肾盂,1例侵犯腰大肌及肾盂,并形成肾静脉瘤栓,1例肾周淋巴结发现转移。7例镜下均见到特征增生的上皮样细胞,上皮样细胞为多边形,细胞质浓密,呈片巢状或弥漫分布(图1A);病理免疫组化染色后均表现黑色素细胞标志物HMB45、Melan-A强阳性(图1B),平滑肌细胞标志平滑肌肌动蛋白(smooth muscle actin,SMA)弱阳性(图1C),上皮细胞标志细胞角蛋白(cytokeratin,CK)阴性。根据常规染色和免疫组化染色病理均诊断为上皮样血管平滑肌脂肪瘤。
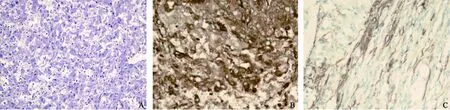
图 1 上皮样血管平滑肌脂肪瘤的HE染色和免疫组化染色Fig. 1 Histopathological and immunohistological characteristics of epithelioid renal angiomyolipoma
2.2 治疗与随访结果
术后患者随访3~36个月,中位随访12个月,7例患者目前均存活。4例复诊未发现复发及转移征象。1例术前发现肝、肺多发转移患者接受舒尼替尼50 mg每日1次,服用4周停2周靶向治疗方案3个月后转移灶明显缩小,疗效评价PR,继续治疗3个月后疾病进展,疗效评价PD。1例术后9个月出现肝转移,行右肝部分切除术,2次术后6个月出现右髂窝转移,行髂窝肿物切除术,第3次手术5个月后出现右盆腔复发,行右盆腔肿物切除术,3次复发及转移病理均为转移性上皮样血管平滑肌脂肪瘤。1例术后1年8个月出现腹腔转移,再次手术切除病理为上皮样血管平滑肌脂肪瘤。
3 讨 论
Martignoni和Delgado等[2-3]最早报道了肾脏上皮样血管平滑肌脂肪瘤。他们分别报道了7例和5例肾脏肿瘤,这些肿瘤术前诊断为肾细胞癌、肾上腺皮质癌、或肾肉瘤。术后发现这类肿瘤在镜下和免疫组化染色后有共同点:都由层状嗜酸的上皮样细胞组成,有大的细胞核和明显的核仁,包含多核巨细胞;对黑素细胞标志如HMB45染色阳性,对actin局灶阳性,对Keratin、Vimentin和Desmin阴性;而肾细胞癌则与之不同,表现为HMB45染色阴性而上皮来源CK标志物染色阳性。这种肿瘤最初被归类为有明显上皮样细胞的肾血管平滑肌脂肪瘤。最初报道的这类肿瘤并没有表现出侵袭性,因此,最初这类肿瘤被认为临床上良性但是在形态上与经典肾血管平滑肌脂肪瘤不同。在随后的时间里,陆续有这类肿瘤的局部复发、远处转移和死亡病例报道。Cibas等[4]报道1例肾部分切除术后3年出现肝转移;Takumi等[5]报道1例活检病理同时发现多发肝转移,其后出现肺转移和骨转移,3个月后患者死于肿瘤进展。之后WHO在2004年的肾脏肿瘤分类中将这类肿瘤归类为上皮样血管平滑肌脂肪瘤。其后大宗病例报道总结了69例上皮样血管平滑肌脂肪瘤,表明其恶性比例为38%[6]。2010年Brimo等[7]回顾了40例上皮样血管平滑肌脂肪瘤,在随访的34例患者中,9例(26%)表现有复发或远处转移,4例死亡,2例在就诊时即伴有远处转移。Brimo等[7]将上皮样血管平滑肌脂肪瘤按有无不典型细胞核分为两类,有不典型细胞核的一类考虑有恶性可能。据此提出了上皮样血管平滑肌脂肪瘤良恶性分辨的预测模型。该模型提出:①≥70%的上皮样细胞可发现不典型的细胞核;②每10个高倍镜视野存在≥2个核分裂像;③发现不典型的分裂像;④发现坏死。78%的恶性上皮样血管平滑肌脂肪瘤可以符合4项中至少3项。Xu等[8]报道Ki-67也可成为肾上皮样血管平滑肌瘤的恶性及预后指标。
与经典肾血管平滑肌脂肪瘤不同,肾上皮样血管平滑肌脂肪瘤具有侵袭性。肾上皮样血管平滑肌脂肪瘤以上皮样细胞为主,缺乏脂肪组织,仅根据临床和影像表现难以同肾癌相区分[9]。本研究报道的7例患者中有5例术前诊断为肾细胞癌。对经典肾血管平滑肌脂肪瘤,手术切除是治愈手段。但是对上皮样血管平滑肌脂肪瘤,根治性肾切除术后肿瘤仍可能有局部复发或远处转移[10]。Tsai等[1]报道约1/3的上皮样血管平滑肌脂肪瘤是恶性表现,需要严密随诊。本研究中,有2例术后出现肿瘤转移,这2例转移灶行手术治疗后的无瘤生存期均较短。但是从文献中没有发现对上皮样血管平滑肌脂肪瘤除手术外的有效治疗方式。Cibas等[4]报道应用多柔比星的化疗对上皮样血管平滑肌脂肪瘤有效。Heidi等[11]报道mTOR通路在上皮样血管平滑肌脂肪瘤的生长及进展中起重要作用,共评价了15例上皮样血管平滑肌脂肪瘤。结果发现,这些肿瘤p70S6K表达提高,AKT表达降低。表明mTOR抑制剂,如雷帕霉素(rapamycin)或其脂化物Temsirolimus可能对上皮样血管平滑肌脂肪瘤有治疗作用。Shitara等[12]报道依维莫司(everolimus)对转移性肾上皮样血管平滑肌瘤有效。本研究中,1例肾上皮样血管平滑肌脂肪瘤同时伴有肝、肺多发转移的患者应用舒尼替尼治疗3个月,疗效评价PR,提示可以尝试将舒尼替尼的靶向治疗用于转移或复发的肾上皮样血管平滑肌脂肪瘤。但是继续治疗3个月后肿瘤进展,疗效评价PD,考虑肾上皮样血管平滑肌脂肪瘤活跃靶点与肾细胞癌可能存在差异,需要更多病例进一步验证疗效。
[1] TSAI C C, WU W J, LI C C, et al. Epithelioid angiomyolipoma of the kidney mimicking renal cell carcinoma: a clinicopathologic analysis of cases and literature review[J]. Kaohsiung J Med Sci, 2009, 25:133-140.
[2] MARTIGNONI G, PEA M, BONETTI F, et al. Renal epithelioid oxyphilic neoplasm (REON): a pleomorphic monophasic variant of renal angiomyolipoma[J]. Int J Surg Pathol, 1994, 2(Suppl): 539.
[3] DELGADO R, DE LEON BOJORGE B, ALBORESSAAVEDRA J. Atypical angiomyolipoma of the kidney: a distinct morphologic variant that is easily confused with a variety of malignant neoplasms[J]. Cancer, 1998, 83: 1581-1592.
[4] CIBAS E S, GOSS G, KULKE M, et al. Malignant epithelioid angiomyolipoma (‘sarcoma ex angiomyolipoma’) of the kidney: a case report and review of the literature[J]. Am J Surg Pathol, 2001, 25: 121-126.
[5] TAKUMI Y, KAZUTO I, KAZUHIRO S, et al. Rapidly progressive malignant epithelioid angiomyolipoma of the kidney[J]. J Urol, 2002, 168: 190-191.
[6] FARAJI H, NGUYEN B N, MAI K T. Renal epithelioid angiomyolipoma: a study of six cases and a meta-analytic study. Development of criteria for screening the entity with prognostic significance[J]. Histopathology, 2009, 55: 525-534.
[7] BRIMO F, ROBINSON B, GUO C, et al. Renal epithelioid angiomyolipoma with atypia: a series of 40 cases with emphasis on clinicopathologic prognostic indicators of malignancy[J]. Am J Surg Pathol, 2010, 34(5): 715-722.
[8] XU C, JIANG X Z, ZHAO H F, et al. The applicability of Ki-67 marker for renal epithelioid angiomyolipoma: experience of ten cases from a single center[J]. Neoplasma, 2012, Nov 25. doi: 10.4149/neo_2013_028.
[9] RAMAN S P, HRUBAN R H, FISHMAN E K. Beyond renal cell carcinoma: rare and unusual renal masses[J]. Abdom Imaging, 2012, 37(5): 873-884.
[10] VARMA S, GUPTA S, TALWAR J, et al. Renal epithelioid angiomyolipoma: a malignant disease[J]. J Nephrol, 2011, 24(1): 18-22.
[11] HEIDI K, FOLPE A, TAKAYAMA T, et al. Activation of the mTOR pathway in sporadic angiomyolipomas and other perivascular epithelioid cell neoplasms[J]. Hum Pathol, 2007, 38: 1361-1371.
[12] SHITARA K, YATABE Y, MIZOTA A, et al. Dramatic tumor response to everolimus for malignant epithelioid angiomyolipoma[J]. Jpn J Clin Oncol, 2011, 41(6): 814-816.
Epithelioid angiomyolipoma of the kidney
SHI Hong-zhe, LI Chang-ling, SHOU Jian-zhong, WANG Dong, GUAN Kao-peng, HAN Su-jun, WEN Li (Department of Urology, Cancer Institute and Cancer Hospital Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing 100021, China)
LI Chang-ling E-mail: changllss@yahoo.com.cn
Background and purpose: The epithelioid angiomyolipoma has been recognized in the 2004 WHO classification of renal tumors, but there is still limited understanding of the true biologic nature of this tumor. This study was to investigate the clinicopathologic features, diagnosis, and treatment of epithelioid angiomyolipoma of the kidney. Methods: Seven cases of epithelioid angiomyolipoma of the kidney were analyzed retrospectively. There were 3 males and 4 females with median age of 28 years (ranging from 23-55 years). Four patients had chief complain and the other 3 cases were found renal masses in routine physical examination. Four tumors localized in the kidney; 1 tumor invaded pelvis and renal vein; 1 tumor accompanied with retroperitoneal lymph node metastases; 1 tumor accompanied with liver and lung metastases. Five cases were diagnosed as renal cell carcinoma and the other 2 cases were diagnosed as minimal fat renal angiomyolipoma. Five cases were
radical nephrectomy and 2 cases were received partial nephrectomy. Results: Tumors were lacking pseudocapsule with renal tissue. The median mass diameter was 5cm (ranging from 2.5-14 cm). Tumors were hard, multinodular, grey to grey yellow or grey red, 2 tumors invaded psoas major; 2 tumors invaded pelvis; 1 tumor invaded renal vein; 1 tumor had local lymph nodes metastases. Tumors were composed of typical epithelioid cells, HMB45 and Melan-A positive, SMA weak positive, and CK negative by immunohistochemcial staining. Pathological diagnosis was epithelioid angiomyolipoma. All cases were followed up for 3 to 36 months. Median follow up was 12 months. All 7 cases were surviving, 4 cases did not recurrence or metastases; 2 cases were suffered metastases and were received surgery; 1 case with liver and lung metastases was receivedsunitinib treatment 6 months. Conclusion: Renal epithelioid angiomyolipoma was atypical in clinical and imaging findings, need differential with renal cell carcinoma and minimal fat renal angiomyolipoma. HMB45 was positive in immunohistochemcial staining. Operation was major method but recurrence or metastases were possible. Surgery and target therapy may be effective treatment for metastases.
Kidney neoplasms; Epithelioid angiomyolipoma; Target therapy
10.3969/j.issn.1007-3969.2013.03.009
R737.11
:A
:1007-3639(2013)03-0207-04
2012-11-20
2013-01-05)
李长岭 E-mail:changllss@yahoo.com.cn
猜你喜欢
世界最新医学信息文摘(2021年12期)2021-06-09 08:35:02
幸福家庭(2021年1期)2021-03-08 12:31:51
中国现代医药杂志(2020年12期)2020-02-06 06:32:56
中国临床医学影像杂志(2019年4期)2019-06-18 10:55:06
浙江中西医结合杂志(2018年12期)2018-12-27 01:51:10
罕少疾病杂志(2016年5期)2016-03-11 16:34:45
中国卫生标准管理(2015年1期)2016-01-14 03:41:22
实用手外科杂志(2015年2期)2015-04-02 15:32:07
郑州大学学报(医学版)(2015年1期)2015-02-27 14:50:36
西南军医(2014年6期)2014-01-22 06:57:57