
Hemi-semi Laminectomy Approach for the Microsurgical Treatment of Spinal Schwannomas
2012-11-22 02:36:42XingSuWeiShiQingfengHuangJianhongShenandJianChen
Chinese Medical Sciences Journal 2012年2期
Xing Su,Wei Shi,Qing-feng Huang,Jian-hong Shen,and Jian Chen*
Department of Neurosurgery,Affiliated Hospital of Nantong University,Nantong 226001,China
SCHWANNOMAS are relatively common in neurosurgical practice,accounting for approximately 25% of all primary spinal tumors.1Because conventional laminectomy may be related to postoperative spinal instability and deformity,2,3hemilaminectomy approach to access intradural pathology were developed in part to reduce the risk of postlaminectomy complications since 1980s.4,5To minimize iatrogenic trauma and postoperative instability,hemilaminectomy for the resection of spinal tumors or vascular malformations has been shown to have some merits.6-8Now that our goal is minimally invasive surgery,hemi-semi laminectomy can further spare the mechanically relevant bone structures and we used hemi-semi laminectomy fenestration as an approach to the removal of spinal schwannomas.We described our experiences in the use of this technique,discussed its advantages and drawbacks,and detailed the technical aspects and perioperative complications of this approach to spinal tumors.
PATIENTS AND METHODS
Between April 2009 and August 2011,22 spinal schwannomas patients who underwent hemi-semi laminectomy in Affiliated Hospital of Nantong University were included in this retrospective study.The patients ranged from 16 to 69 years of age (median 44 years).The study consisted of 14 female and 8 male patients.We analyzed the clinical presentations,imaging examination,surgical technique,and outcomes of these patients.
RESULTS
Clinical presentations
All patients suffered from local or radicular pain and sensory or motor disturbance of the extremities.Preoperative neurological examination showed weakness of the extremities in 12 cases,sensory disturbances in 14 cases,and sphincter dysfunction in 4 cases.Detailed clinical manifestations are summarized in Table 1.The course of the disease ranged from 2 to 72 months,with the mean being 18 months.
Results of imaging examination
Every patient was diagnosed as having spinal schwannomas by plain and enhanced magnetic resonance imaging(MRI).T1-weighted MRI showed the lesions were isointense in 14 patients and hypointense in 8 patients,whereas T2-weighted MRI demonstrated the lesions were hyperintense in 16 patients and isointense in 6 patients.The tumors were observed in the following regions:cervical in 5 cases,thoracic in 9,and lumbar in 8.Postoperative CT-scan and MRI were obtained to evaluate the spinal stability and whether there was any remnant tumor or recurrence respectively.

Table 1.Clinical summary of 22 spinal schwannomas patients
Surgical technique
All patients were operated on in a prone position after general anesthesia and hemi-semi laminectomy was performed through a midline incision.C-armed roentgenogram was usually undertaken to precisely localize incision intraoperatively.We performed a longitudinal paramedian dural incision.Subperiosteal detachment of the paravertebral muscle was performed on the affected side,preserving the spinous processes and supra/interspinal ligaments.High-speed grinding drill was used to unilateral partial laminae fenestration (Figs.1 and 2)and partial vertebral arches bony structures were retained (Fig.3).The dissection of the arachnoid compartments and the release of cerebrospinal fluid provided a larger space for surgical manipulation intraoperatively.One-piece removal was performed for small tumors under microscope (Fig.1D),but patients with larger or tough lesions underwent internal debulking and piecemeal resection.
Outcomes
The mean surgical time was 2.2 hours (range,1.5-3.0 hours) and the mean blood loss was 150 mL (range,50 to 400 mL).All the patients were mobilized on second day postoperatively.Postoperative MRI within 72 hours for all patients revealed complete removal of the tumor (Fig.3B).In 2 cases of dumbbell schwannomas,we applied this approach to remove tumors completely.Conversion to conventional laminectomy was not required in any of the cases in our study.
All patients were followed up from 6 to 36 months.In all the treated cases,the pain and neurological deficit were improved compared to their preoperative neurological status.No incision cerebrospinal fluid leak was noted.There were 2 cases experiencing wound infection and 1 case with urinary infection,which were cured after antibiotic therapy (Table 1).At follow-up evaluation none of the patients showed signs of spinal instability or deformity(Fig.3F).
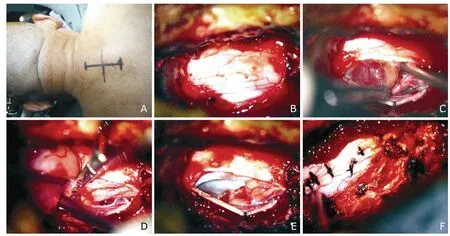
Figure 1.Intraoperative photographs of resection of schwannoma at the C5-6by hemi-semi laminectomy (Case 4).
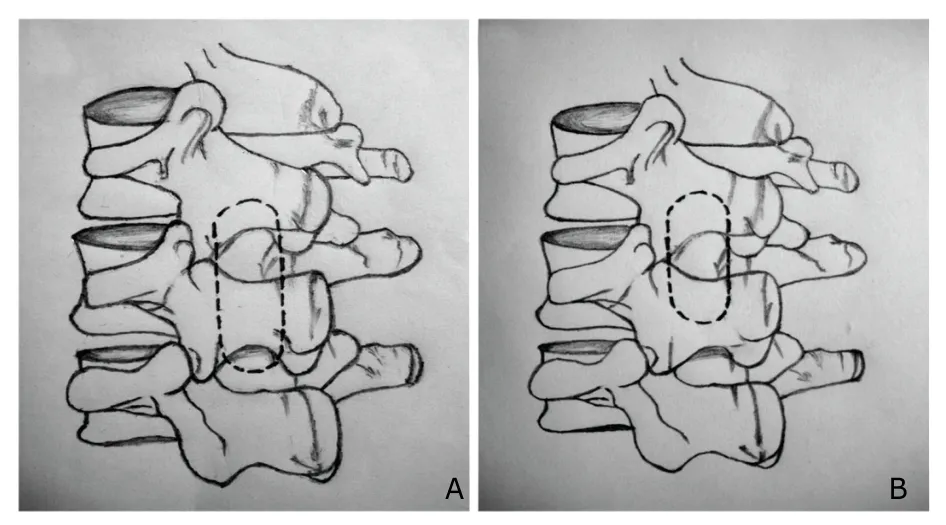
Figure 2.Artist’s illustrations show the extent of bone removal by traditional hemilaminectomy (A) and hemi-semi laminectomy (B),respectively.
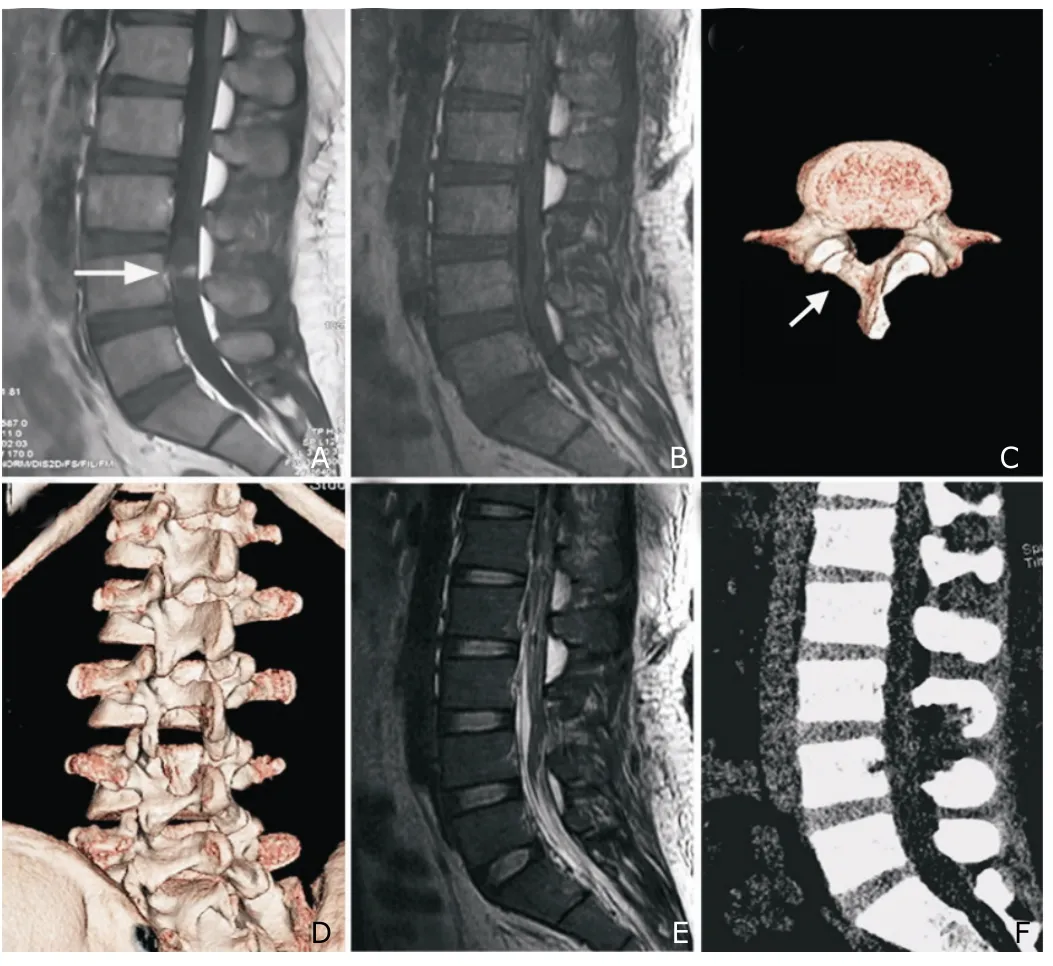
Figure 3.Pre-and postoperative imaging results of Case 22.
DISCUSSION
In 1983,Denis firstly described the concept of the three-column theory.Numerous studies confirmed that the intact middle and posterior column structures were very critical to spinal stability.9,10Taking into account the functional importance of posterior column structures,it is possible that surgical approaches to the vertebral column that resect bone structures or ligaments increase the risk of early or late spinal instability.11,12
Conventional laminectomy continues to be commonly used for removal of spinal tumors,but it may be associated with a number of postoperative complications.Both clinical data and biomechanical studies have demonstrated that bilateral damage to paravertebral muscles and ligaments,together with removal of the spinous process,might entail postoperative instability and/or deformity.13,14With the development of minimally invasive technique,numerous investigators have reported their experience using hemilaminectomy to resect spinal tumors.5,15However,we perceived that hemi-semi laminectomy can achieve a further reduction in iatrogenic trauma because except for the contralateral laminae and supra/interspinal ligaments,the partial vertebral arches bony structures are preserved as much as possible and the original form of the spine can be better preserved compared with hemilaminectomy.as much as possible and the original form of the spine can be better preserved compared with hemilaminectomy.
The modified hemilaminectomy approach has been used in the surgical treatment of degenerative spinal stenosis,in patients with tumors and hematomas.16-18In our series,hemi-semi laminectomy can acquire excellent visualization and sufficient working space for the removal of spinal schwannomas.Most importantly,the tumors were able to be completely resected without adverse neurological complications.18,19The necessary considerations preoperatively in using this technique for spinal schwannomas are the accurate location and size of the lesion.In addition,arachnoidal openings and the release of cerebrospinal fluid and combination with surgical bed tilted angles intraoperatively help to obtain larger operative field.We believed that hemi-semi laminectomy was suit for the resection of one or two level spinal schwannomas.If the tumor is larger than 2.5 cm,especially in the cervical or thoracic levels,we recommend piecemeal removal,and aggressive removal should be avoided.20,21In this paper,hemi-semi laminectomy was selected for resection of tumors located at dorsal spinal cord.We should note that this approach also has its limitations and drawbacks.Because of the relatively limited exposure,we suggested that the tumors located in ventral spinal cord or adhered to spinal
The modified hemilaminectomy approach has been used in the surgical treatment of degenerative spinal stenosis,in patients with tumors and hematomas.16-18In our series,hemi-semi laminectomy can acquire excellent visualization and sufficient working space for the removal of spinal schwannomas.Most importantly,the tumors were able to be completely resected without adverse neurological complications.18,19The necessary considerations preoperatively in using this technique for spinal schwannomas are the accurate location and size of the lesion.In addition,arachnoidal openings and the release of cerebrospinal fluid and combination with surgical bed tilted angles intraoperatively help to obtain larger operative field.We believed that hemi-semi laminectomy was suit for the resection of one or two level spinal schwannomas.If the tumor is larger than 2.5 cm,especially in the cervical or thoracic levels,we recommend piecemeal removal,and aggressive removal should be avoided.20,21In this paper,hemi-semi laminectomy was selected for resection of tumors located at dorsal spinal cord.We should note that this approach also has its limitations and drawbacks.Because of the relatively limited exposure,we suggested that the tumors located in ventral spinal cord or adhered to spinal cord tightly intraoperatively were removed by laminectomy.15Maybe the lesions being resected in this study were relatively small,we did not find a need to expand to hemilaminectomy or converted into a conventional laminectomy approach intraoperatively.
Although this is a small series of consecutive patients with a short period of follow-up,we have demonstrated that it is feasible to completely resect most spinal schwannomas safely with the advantages of less operative invasion and postoperative complications.However,it should be noted that this approach should be reproduced by practitioners familiar with minimally invasive techniques.
In conclusion,we believe that the hemi-semi laminectomy can achieve less invasion than hemilaminectomy and is a safe and effective approach for the microsurgical treatment of spinal schwannomas.
1.Louis DN,Ohqaki H,Wiestler OD,et al.The 2007 WHO classification of tumours of the central nervous system.Acta Neuropathol 2007;114:97-109.
2.Mikawa Y,Shikata J,Yamamuro T.Spinal deformity and instability after multilevel cervical laminectomy.Spine 1987;12:6-11.
3.Yasargil MG,Pait TG.Exposureversusinstability.J Neurosurg1996;84:891-2.
4.Chiou SM,Eggert HR,Laborde G,et al.Microsurgical unilateral approaches for spinal tumour surgery.Acta Neurochir 1989;100:127-33.
5.Oktem IS,Akdemir H,Kurtsoy A,et al.Hemilaminectomy for the removal of the spinal lesions.Spinal Cord 2000;38:92-6.
6.Asazuma T,Nakamura M,Matsumoto M,et al.Postoperative changes of spinal curvature and range of motion in adult patients with cervical spinal cord tumors:analysis of 51 cases and review of the literature.J Spinal Disord Tech 2004;17:178-82.
7.Sridhar K,Ramamurthi R,Vasudevan MC,et al.Limited unilateral approach for extramedullary spinal tumours.Br J Neurosurg 1998;12:430-3.
8.Kanemoto Y,Ohnishi H,Koshimae N,et al.Ventral T-1 neurinoma removedviahemilaminectomy without costotransversectomy—case report.Neurol Med Chir (Tokyo)1999;39:685-8.
9.Denis F.The three column spine and its significance in the classification of acute thoracolumbar injuries spinal.Spine 1983;8:817.
10.Ogden AT,Bresnahan L,Smith JS,et al.Biomechanical comparison of traditional and minimally invasive intradural tumor exposures using finite element analysis.Clin Biomech (Bristol Avon) 2009;24:143-7.
11.Hosono N,Sakaura H,Mukai Y,et al.En bloc laminoplasty without dissection of paraspinal muscles.J Neurosurg Spine 2005;3:29-33.
12.de Jonge T,Slullitel H,Dubousset J,et al.Late-onset spinal deformities in children treated by laminectomy and radiation therapy for malignant tumours.Eur Spine J 2005;14:765-71.
13.Ozgur BM,Florman JE,Lew SM,et al.Laminectomy contributes to cervical spine deformity demonstrated byholographic interferometry.J Spinal Disord Tech 2003;16:51-4.
14.McLaughlin MR,Wahlig JB,Pollack IF.Incidence of postlaminectomy kyphosis after Chiari decompression.Spine(Phila Pa 1976)1997;22:613-7.
15.Pompili A,Caroli F,Cattani F,et al.Unilateral limited laminectomy as the approach of choice for the removal of thoracolumbar neurofibromas.Spine (Phila Pa 1976) 2004;29:1698-702.
16.Börm W,Mohr K,Hassepass U,et al.Spinal hematoma unrelated to previous surgery:analysis of 15 consecutive cases treated in a single institution within a 10-year period.Spine 2004;29:555-61.
17.Schillberg B,Nyström B.Quality of life before and after microsurgical decompression in lumbar spinal stenosis.J Spinal Disord 2000;13:237-41.
18.Balak N.Unilateral partial hemilaminectomy in the removal of a large spinal ependymoma.Spine J2008;8:1030-6.
19.Takamura Y,Uede T,Igarashi K,et al.Thoracic dumbbell-shaped neurinoma treated by unilateral hemilaminectomy with partial costotransversectomy—case report.Neurol Med Chir (Tokyo) 1997;37:354-7.
20.Koch-Wiewrodt D,Wagner W,Perneczky A.Unilateral multilevel interlaminar fenestration instead of laminectomy or hemilaminectomy:an alternative surgical approach to intraspinal space-occupying lesions.Technical note.J Neurosurg Spine2007;6:485-92.
21.Schick U,Marquardt G,Lorenz R.Recurrence of benign spinal neoplasms.Neurosurg Rev2001;24:20-5.
 Chinese Medical Sciences Journal2012年2期
Chinese Medical Sciences Journal2012年2期
- Chinese Medical Sciences Journal的其它文章
- Correlations Between Serum Uric Acid Level and Disease Activity,Intrathecal Inflammation Reactivity in Patients with Multiple Sclerosis
- Primary Meningeal Melanocytoma Located in Foramen Magnum:a Case Report and Review of the Literatures
- Sternal Insufficiency Fractures of Post-menopausal Women:Retrospective Analysis of 17 Cases
- Fresh Frozen Plasma for the Treatment of Hereditary Angioedema Acute Attacks
- Function of microRNA-346 and its Roles in Human Diseases
- Multiple Coatings can Improve the Bond Durability of One-step Self-etching Adhesive to Primary Dentin