
Sternal Insufficiency Fractures of Post-menopausal Women:Retrospective Analysis of 17 Cases
2012-11-18 13:33:36ZheyuanHuangBilongYiandHaoyuanLiu
Chinese Medical Sciences Journal 2012年2期
Zhe-yuan Huang,Bi-long Yi,and Hao-yuan Liu*
Department of Orthopaedics,Chenggong Hospital Affiliated to Xiamen University,Xiamen 361000,China
INSUFFICIENCY fractures tend to occur in the elderly with the decreased mechanical strength of bone,particularly post-menopausal women with underlying diseases.The spine,pelvis,and long bones of the lower extremities are common sites of insufficiency fractures.1,2The insufficiency fracture of the sternum is rare.In older women,the sternum is an anatomic site predisposed to the development of insufficiency fractures.In this study,we investigated the clinical presentation,associated diseases,and radiographic findings of postmenopausal women with sternal insufficiency fractures(SIFs) to investigate the clinical characteristics of them.
PATIENTS AND METHODS
A retrospective review of the medical records of 17 post-menopausal women admitted to Chenggong Hospital Affiliated to Xiamen University for treatment of SIFs between February 1999 and January 2009 was carried out.In the absence of any other cause,SIF was diagnosed when fracture spontaneously occurred or as a result of moderate pressure,and when it was confirmed by standard radiography and/or scintigraphy,computed tomography (CT) or magnetic resonance imaging (MRI).Medical records provided the following information∶age,previous medical history,clinical manifestations,the site and type of fracture,associated fractures,and risk factors for bone loss (endocrinopathy,corticosteroid treatment,thoracic kyphosis).Details of the patients’ histories (presenting clinical manifestations) and clinical features of the observations were presented.Results of complementary examinations were reviewed—namely,standard radiography,bone scintigraphy,CT,and MRI.Osteodensitometry was performed,and osteoporosis was diagnosed if the T-score was <﹣2.5 standard deviations.
RESULTS
Their mean age was 73.8 years,ranging from 63 to 89 years.
Clinical symptoms,signs and associated diseases
Table 1 presents details of the clinical symptoms,signs and associated diseases of the patients.
None of the patients were aware of any trauma that might have been responsible for the sternal fracture.The most common complaint was chest pain (12 cases).Twelve patients reported severe anterior chest pain which did not change with position or on inspiration.The syndrome mimicked myocardial infarction or angina pectoris,but electrocardiography showed no definite abnormality.Further medical examinations,including chest radiography,repeated electrocardiography,and cardiac enzyme examination,were normal.Other symptoms included cough(5 cases),dyspnoea (3 cases),breathlessness (3 cases),and wheeze (2 cases).Four patients had no discomfort.
Examination showed that the sternums of 10 cases were tender on palpation.No crepitus was seen.Some patients were also tender over the lower ribs (6 cases) and thoracic spine (5 cases).Auscultation of the chest revealed normal breath sounds in most cases (14 cases),with only 3 patients showing diffuse bilateral wheezes and basal crackles.
Five of seven patients with chronic obstructive pulmonary disease (COPD) and two of three patients with rheumatoid arthritis (RA) were taking corticosteroids at the time of the diagnosis of SIFs.For the past 5-10 years they had received 5-10 mg prednisolone daily,and frequent courses of high-dose systemic corticosteroids.One patient had systemic lupus erythematosus and had been treated with oral prednisolone (5-15 mg/d) for the past 9 years.The oldest patient had received long-term treatment with high-dose prednisolone (15 mg/d) and bronchodilator drugs for asthma for the previous 13 years.
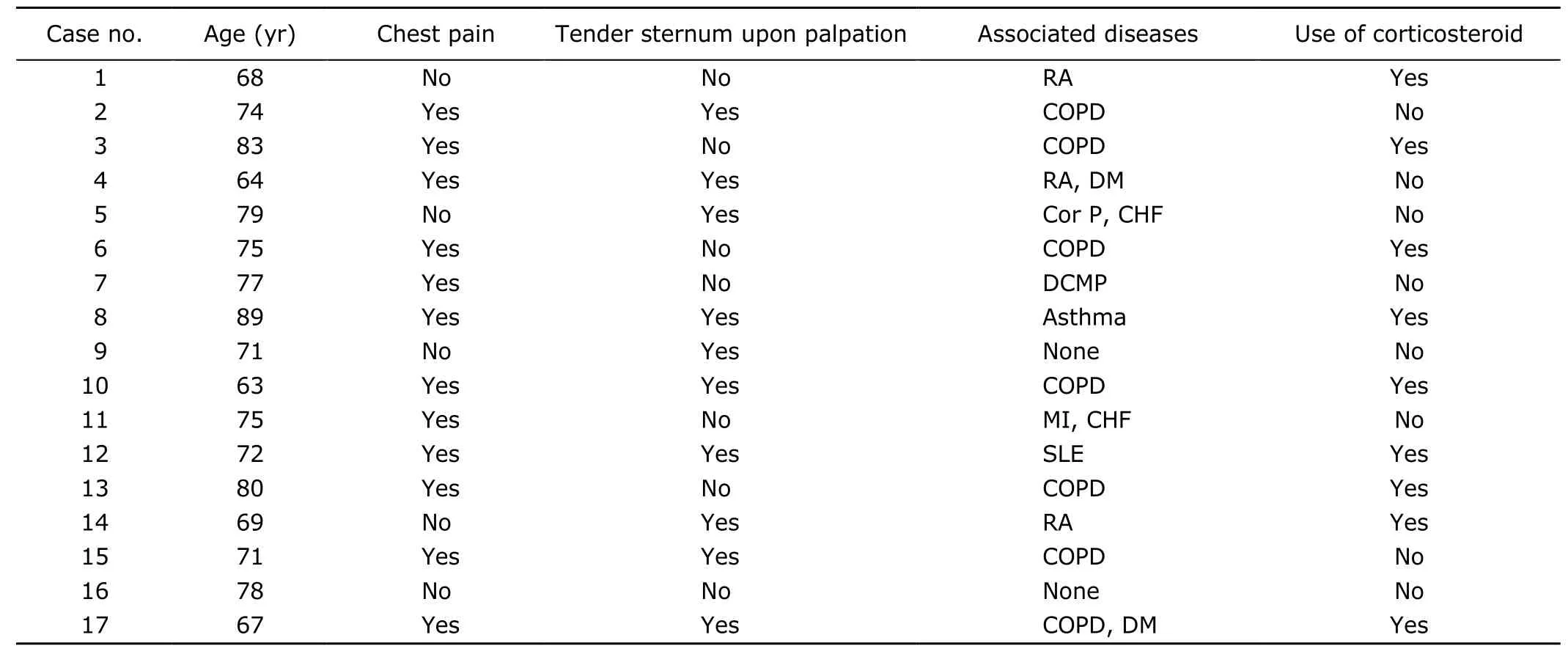
Table 1.Clinical symptoms,signs and associated diseases of the 17 patients with sternal insufficiency fracture
Complementary examinations
The main features of SIFs and associated fractures of the patients are described in Table 2.
Plain radiographs were available in all cases,radionuclide bone scans in 12,computed tomography (CT) scans in 10,and MRI results for 3 patients.The fracture site was categorized according to the anatomic sites of the sternum,xiphoid,body,and manubrium (Table 2).The fractures of 15 (88%) patients were located at the sternal body,1 patient in the manubrium,and 1 patient in the manubriosternal junction.Displaced fracture occurred in 13 cases.Lateral radiography of the sternum showed a fracture line in 14 patients.For the remaining 3 cases,radiologic imagings were normal,and the diagnosis was established by CT scan and MRI.Osteodensitometry revealed 17 patients had osteoporosis.Radiographs of the spine showed advanced osteoporosis with collapse of thoracic vertebral bodies in 13 patients (Table 2).The bone CT scans performed in 10 cases were positive.MRI,performed in 3 patients,showed the fracture by low-signal intensity on T1-and T2-weighted images.Scintigraphy showed increased tracer uptake in 12 cases.
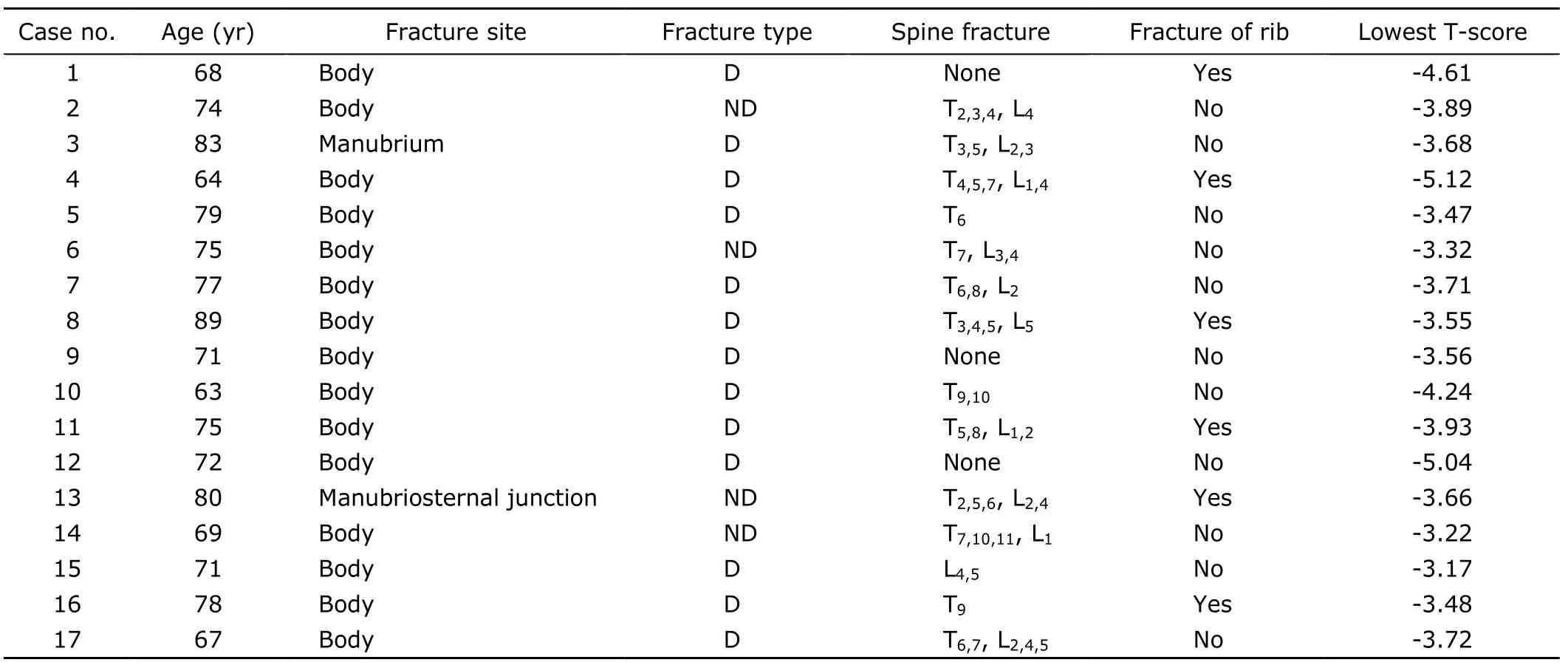
Table 2.Main features of sternal insufficiency fractures and associated fractures of the 17 patients
DISCUSSION
Stress fractures can be classified into fatigue fractures caused by repetitive subthreshold trauma,insufficiency fractures occurring in bones with reduced mechanical strength,and pathological fractures that occur in diseased bones.3Insufficiency fractures,as seen in the women described here,occur in weakened bones unable to withstand even the stresses of normal daily activities.Osteoporosis is the most common predisposing condition.Insufficiency fractures,therefore,are more frequently seen in older women.These fractures occur at a great variety of sites,including the spine,sacrum,4-7pubis,8ilium,9long bones of the lower extremities,10,11and foot.The sternum is yet another site of insufficiency-type stress fractures.
Insufficiency fractures of the sternum are rare.In a retrospective survey by Soubrieret al12on all insufficiency fractures except for spinal fractures,only one (1.1%)sternal fracture was identified among 91 insufficiency fractures.
In most cases,SIFs occur at the junction between the superior third and the two inferior thirds of the sternal body,13while fracture of the manubrium (upper part of sternum) is rare.Of our 17 patients,only 2 had fractures that were not located in the body of the sternum—1 was located in the manubrium,and the other at the manubriosternal junction.
Osteoporosis is thought to be a possible predisposing factor for SIF14and plain radiography or osteodensitometry showed varying degrees of osteoporosis in all our patients.COPD was a commonly associated disease in a study of 15 patients with SIF described by Min and Sung,15and 7/17 patients in our study had COPD.In addition,inflammatory joint disease such as RA,16-18systemic lupus erythematosus,19post-menopausal state,16,18,20short-or long-term corticosteroid therapy,16,18,21,22fluoride therapy without proper vitamin D supplements18and limited mobility were considered to be predisposing factors.
Stress fractures typically present as localized pain that develops without a history of a specific acute injury.The two common symptoms in patients who develop SIF are chest pain of sudden onset23and dyspnoea24.Moderately severe mechanical pain in the anterior chest wall exacerbated by coughing and deep breathing occurs in some patients.18Pain localised to the sternum may be so intense that it may simulate myocardial infarction13,25-28or pulmonary embolism29.Therefore,SIF should be considered in the differential diagnosis of acute chest pain in the elderly together with myocardial infarction or pulmonary embolism.Cardiopulmonary disorders as a possible cause of chest pain were ruled out by electrocardiography,laboratory findings,and the clinical course in our patients.Dyspnoea,induced by paradoxical movement of the upper fragment,can worsen respiratory distress in patients with chronic airflow obstruction and aggravate respiratory failure.Clinically,sternal fractures can be silent,18,21,30,31as in 2 patients in our study.The symptoms of some patients are trivial or go unnoticed,and this fact is in keeping with the relatively high incidence of sternal fractures (34/839)noted at necropsy by Urovitzet al.32Palpation of the sternal bone reveals marked tenderness,but in some cases this procedure is overlooked,at least during the acute episode.A physical examination may show edema,local swelling,or even sternal deformity.16,18,20
A lateral radiograph of the sternum is most useful in providing an accurate diagnosis.23The diagnosis is confirmed by lateral chest radiographs which,in addition to location of the fracture,provide information about the stability of the fragments,the stage reached in the process of callus formation,additional thoracic vertebral fractures and thoracic kyphosis.16-18,20,21,30The lateral chest radiograph can disclose a break in the bone,sometimes with a rim of osteosclerosis.18In those cases where plain radiographs demonstrate changes consistent with a fracture,including a fracture line or fracture callus,no other studies are needed.In other cases,plain radiographs will be normal or non-diagnostic and the diagnosis may be delayed.In these instances,more sensitive tests,such as bone scans,CT or MRI,will usually demonstrate abnormalities consistent with a fracture.CT provides information on the location,extent,and stage of repair and helps to exclude the possibility of infection and malignancy.6
Bone scintigraphy is a useful diagnostic tool for a SIF,5showing an intense horizontal or oblique tracer uptake,contributing to early diagnosis.In most cases,increased tracer uptake on the bone scan is seen within 72 hours at the fracture sites,but an insufficiency fracture may be detected as early as 1 day after its occurrence.Optimal use of these tests requires an understanding of the specific advantages,indications,and approach to the interpretation of each imaging modality.Bone biopsy should be considered only when malignancy18and infection are suspected.Abundant granulation tissue with reactive bone and hyaline cartilage are the main histological features in bone biopsy specimens from an insufficiency fracture.33
An association between thoracic kyphosis and sternal fracture has been reported.21Berg34suggested that the sternal-rib complex represents a fourth column of structural thoracic spine support.Muldoonet al35described the ribs,sternum,and vertebrae as three structures stabilizing the thoracic cavity;failure of one will result in additional stress being placed on the others.They reported a case of multiple rib fractures in association with a thoracic vertebral body compression fracture and a sternum fracture.Biomechanical evidence with cadavers also supports this view because the sternum provides 11.2% of compressive stiffness (inverse of the flexibility) of the thoracic spine in axial compression.36Excessive bone loss results in osteoporosis with the risk of vertebral compression fractures.This,in turn,can lead to progressive thoracic kyphosis and a deforming stress to the sternum,which is also thought to add to the risk of sternal fractures.20,21In our study,13 patients with SIFs had associated fractures of thoracic vertebrae.But the relationship between SIF and accentuated dorsal kyphosis is still controversial.15,16,30SIFs may occur with or without exaggerated thoracic kyphosis,so we still cannot reach a definite conclusion about the association.However,it is undeniable that exaggerated thoracic kyphosis is one of the risk factors for SIF.
In conclusion,SIFs of post-menopausal women,although rare,should be considered in patients who present with acute chest pain.Osteoporosis,glucocorticoid therapy,COPD,and RA might be risk factors.Chest pain in this patient cohort is a serious symptom.So SIF should be considered in the differential diagnosis with myocardial infarction or pulmonary embolism.
1.Cooper KL.Insufficiency stress fractures.Curr Probl Diagn Radiol 1994;23∶29-68.
2.Verwimp W.Sternal insufficiency fracture.JBR-BTR 2008;91∶174.
3.Pentecost RL,Murray RA,Brindley HH.Fatigue,insufficiency,and pathologic fractures.JAMA 1964;187∶1001-4.
4.Lourie H.Spontaneous osteoporotic fracture of the sacrum.An unrecognized syndrome of the elderly.JAMA 1982;248∶715-7.
5.Ries T.Detection of osteoporotic sacral fractures with radionuclides.Radiology 1983;146∶783-5.
6.Cooper KL,Beabout JW,Swee RG.Insufficiency fractures of the sacrum.Radiology 1985;156∶15-20.
7.De Smet AA,Neff JR.Pubic and sacral insufficiency fractures∶clinical course and radiologic findings.AJR 1985;145∶601-6.
8.Casey D,Mirra J,Staple TW.Parasymphyseal insufficiency fractures of the os pubis.AJR 1984;142∶581-6.
9.Cooper KL,Beabout JW,McLeod RA.Supraacetabular insufficiency fractures.Radiology 1985;157∶15-7.
10.Schneider R,Kaye JJ.Insufficiency and stress fractures of the long bones occurring in patients with rheumatoid arthritis.Radiology 1975;116∶595-9.
11.Manco LG,Schneider R,Pavlov H.Insufficiency fractures of the tibial plateau.AJR 1983;140∶1211-5.
12.Soubrier M,Dubost JJ,Boisgard S,et al.Insufficiency fracture.A survey of 60 cases and review of the literature.Joint Bone Spine 2003;70∶209-18.
13.Schapira D,Nachtigal A,Scharf Y.Spontaneous fracture of the sternum simulating myocardial infarction.Clin Rheumatol 1995;14∶478-80.
14.Maenpaa HM,Soini I,Lehto MU,et al.Insufficiency fractures in patients with chronic inflammatory joint diseases.Clin Exp Rheumatol 2002;20∶77-9.
15.Min JK,Sung MS.Insufficiency fractures of the sternum.Scand J Rheumatol 2003;32∶179-80.
16.Itani M,Evans GA,Park WM.Spontaneous sternal collapse.J Bone Joint Surg Br 1982;64∶432-4.
17.Aymard A,Chevrot A,Wybier M,et al.Spontaneous fracture of the sternum.J Radiol 1987;68∶593-5.
18.Pere P,Bannwarth B,Gillet P,et al.Fractures due to bone insufficiency of the sternum.Rev Rhum Mal Osteoartic 1989;56∶843-6.
19.Sen D,Keen RW.Osteoporosis in systemic lupus erythematosus∶prevention and treatment.Lupus 2001;10∶227-32.
20.Sapherson DA,Mitchell SC.Atraumatic sternal fractures secondary to osteoporosis.Clin Radiol 1990;42∶250-1.
21.Cooper KL.Insufficiency fractures of the sternum∶a consequence of thoracic kyphosis? Radiology 1988;167∶471-2.
22.Hameed K,Packe GE,Legge JS,et al.Spontaneous sternal fractures in four patients with chronic airflow obstruction taking corticosteroids.Thorax 1993;48∶1183-4.
23.Buckman R,Trooskin SZ,Flancbaum L,et al.The significance of stable patients with sternal fractures.Surg Gynecol Obstet 1987;164∶261-5.
24.Breederveld RS,Patka P,van Mourik JC.Fractures of the sternum.Neth J Surg 1988;40∶133-5.
25.Rutledge DI.Spontaneous fracture of the sternum simulating myocardial infarction.Postgrad Med 1962;32∶502-4.
26.Horikawa A,Miyakoshi N,Kodama H,et al.Insufficiency fracture of the sternum simulating myocardial infarction∶case report and review of the literature.Tohoku J Exp Med 2007;211∶89-93.
27.Lin KH,Ponampalam R.Sternum insufficiency fracture presenting as acute chest pain∶a case report and review of the literature.Eur J Emerg Med 2006;13∶122-4.
28.Min JK,Joo HJ,Kim TH,et al.A case of sternal insufficiency fracture.Korean J Intern Med 1999;14∶94-7.
29.Vassallo L.Spontaneous fracture of the sternum simulating pulmonary embolism.Br J Clin Pract 1969;23∶388-9.
30.Chen C,Chandnani V,Kang HS,et al.Insufficiency fracture of the sternum caused by osteopenia∶plain film findings in seven patients.AJR 1990;154∶1025-7.
31.Soubrier M,Dubost JJ,Urosevic Z,et al.Stress fracture of the sternum.Apropos of a case.Rev Rhum Ed Fr 1994;61∶559-60.
32.Urovitz EP,Fornasier VL,Czitrom AA.Sternal metastases and associated pathological fractures.Thorax 1977;32∶444-8.
33.Schapira D,Militeanu D,Israel O,et al.Insufficiency fractures of the pubic ramus.Semin Arthritis Rheum 1996;25∶373-82.
34.Berg EE.The sternal-rib complex.A possible fourth column in thoracic spine fractures.Spine 1993;18∶1916-9.
35.Muldoon K,Chu P,Pathria M,et al.Association of posterior rib fractures with exaggerated kyphosis and sternal collapse.Clin Imag 1999;23∶311-3.
36.Watkins R 4th,Watkins R 3rd,Williams L,et al.Stability provided by the sternum and rib cage in the thoracic spine.Spine (Phila Pa 1976) 2005;30∶1283-6.
 Chinese Medical Sciences Journal2012年2期
Chinese Medical Sciences Journal2012年2期
- Chinese Medical Sciences Journal的其它文章
- Hemi-semi Laminectomy Approach for the Microsurgical Treatment of Spinal Schwannomas
- Correlations Between Serum Uric Acid Level and Disease Activity,Intrathecal Inflammation Reactivity in Patients with Multiple Sclerosis
- Primary Meningeal Melanocytoma Located in Foramen Magnum:a Case Report and Review of the Literatures
- Fresh Frozen Plasma for the Treatment of Hereditary Angioedema Acute Attacks
- Function of microRNA-346 and its Roles in Human Diseases
- Multiple Coatings can Improve the Bond Durability of One-step Self-etching Adhesive to Primary Dentin