
胎盘标志物对单绒双羊双胎妊娠合并双胎输血综合征的预测:深部动静脉吻合的形态学分析 点评
2010-01-22 01:10赵德鹏
中国产前诊断杂志(电子版) 2010年2期
赵德鹏
(同济大学附属第一妇婴保健院,上海 200040)
1 原文摘要
ObjectivesThe aim of this study w as to perform a detailed p rospective m orphometric analysis of a large consecutive series of m onochorionic tw in placentas in order to determine the frequency of candidate p lacental markers in TTTS p lacentas and,in particular,to determ ine the potential role of unbalanced deep AV anastom oses.
DesignA cohort of 284 consecutive monochorionic p lacentas was exam ined betw een 2001 and 2008.T riplet and quadrup let placentas,monochorionic-m onoamniotic placentas,p lacentas of gestations comp licated by tw in reversed arterial perfusion(TRAP)sequenceand placentas w ith remote(>48 h prior to delivery)fetal demise of one tw inwere excluded.Of the remaining 253 diamniotic-monochorionic tw in p lacentas,53 were com plicated by TTTS, based on clinical and ultrasound evidence.O f the 53 TTTS cases,29 were treated by laser coagu lation of communicating vessels.These laser-coagulated TTTS p lacentas were excluded from this study.Thus 24 TTTS placentas w ere compared w ith 200 placentas of non-TTTS diamniotic-m onochorionic tw in gestations.Results
1)clinical data
The gestational age at delivery and the birth weights of the TTTS tw ins w ere lower than those of non-TTTS tw ins(Table 1).
2)General p lacental anatomy
The p lacental weights of TTTS tw ins were significantly low er than those of non-TTTS contro l tw ins. The p lacental markers, including velamentous insertion,frequency ofmarginal cord insertion,magistral or m ixed magistral/disperse vascular distribution patterns,>25%difference in p lacental territory between twins and a single umbilical artery,were compared between non-TTTS control placentas and TTTS placentas(Table 2).
3) Choriovascular anatomy: superficial anastomoses(AA and VV)
The total number o f anastom oses visualized in the chorionic plate varied w idely between cases and reached amaximum of 23 in both TTTS and non-TTTS controlgroups.Superficial AA anastomoses were significantly more frequent in non-TTTS p lacentas than in TTTS.None of the TTTS p lacentas had m ore than one AA anastom osis.Among the non-TTTS cases,two p lacentas had 2 and one had 3 AA anastom oses.The diameter of AA anastomoses ranged from 0.05 to 0.4 cm in TTTS p lacentasand from 0.05 to 0.6 cm in non-TTTS controls.
VV anastomoses were more than tw ice as frequent in TTTS p lacentas as in non-TTTS controls.None of the TTTS p lacentas had m ore than one VV anastomosis,whereas six non-TTTS control placentas had 2 VV anastomoses.The maxim al diam eter o f VV anastom oseswas 0.6 cm in TTTS placentas and 0.4 cm in non-TTTS controls.
4)Choriovascular anatomy:deep AV anastom oses
AV anastomoses were seen in95% TTTS placentas and 96%of non-TTTS placentas.The median net number of AV anastom oses w as 2 in both groups,with values ranging from 0 to 7 in TTTS and from 0 to 15 in non-TTTS p lacentas(Table 2).The NCSA was significantly sm aller in TTTS placentas than in non-TTTS controls.Sensitivity and specificity of key p lacentalmarkers as post-hoc predictors of TTTS are shown in Tab le 3. None of the individual candidate p lacental variables,how ever are reliable post-hoc predictors of TTTS.
2 论文核心内容及点评
该文发表在 Placenta 2010年第31卷269-276页上。该文对双胎输血综合征(TTTS)病因的传统观点作一深入的直接的研究和分析。主要内容如下:
传统观点认为双胎间存在动静脉(AV)吻合,而AV吻合中的血流是单向的,因此正是AV吻合中的单向血流造成双胎间血液分配不平衡,进而发生TTTS。尽管认为AV吻合是TTTS的主要病因,但以往的研究大多集中在胎盘表面的动动脉(AA)和静静脉(VV)吻合,对AV吻合的直接研究很少。因此可以说AV吻合是TTTS的主要病因还只是1种观察实验的推测。并无直接实验验证。这可能与AV吻合在胎盘深部,无法直接观察,且研究费时有关。
因此在2001~2008年之间,该研究以200例未合并TTTS的单绒双羊双胎妊娠和24例合并TTTS的单绒双羊双胎妊娠为样本,采用分娩后胎盘灌注技术,对两者的胎盘进行了分析比较。为了对2组胎盘进行尽可能准确的比较,该研究应用净AV吻合数、净AV吻合横截面积,即考虑到AV吻合内血流既有供血儿流向受血儿也有受血儿流向供血儿,因此可相互抵消,最终转化为实际的AV吻合数和AV吻合面积。
该研究结果显示:首先,non-TTTS胎盘AV吻合(96%)较TTTS胎盘AV 吻合(95%)更常见,non-TTTS胎盘无论净AV吻合数还是AV吻合净横截面积都较TTTS多。而且non-TTTS极值情况更易见。甚至在本研究中有1例TTTS胎盘并无AV吻合(表1和表2)。因此传统观点认为 AV吻合是TTTS的病因可能不合理。其次,该研究通过分娩后胎盘灌注比较后,对TTTS胎盘特征进行了总结并深入分析了这些胎盘特征预测TTTS的特异性和敏感性。研究发现TTTS胎盘特征包括胎盘不均衡分配(双胎间胎盘面积差异>25%)、缺乏AA吻合、VV吻合较多、脐带帆状附着等。各胎盘特征的特异性和敏感性见下(表3)。最后,该研究还发现AV吻合内血流方向与供血儿 受血儿的鉴别并无肯定的联系。因为AV吻合中的血流既可以从 供血儿 流向 受血儿 ,亦可从受血儿 流向 供血儿 。

表1 胎盘数据

表2a 胎盘
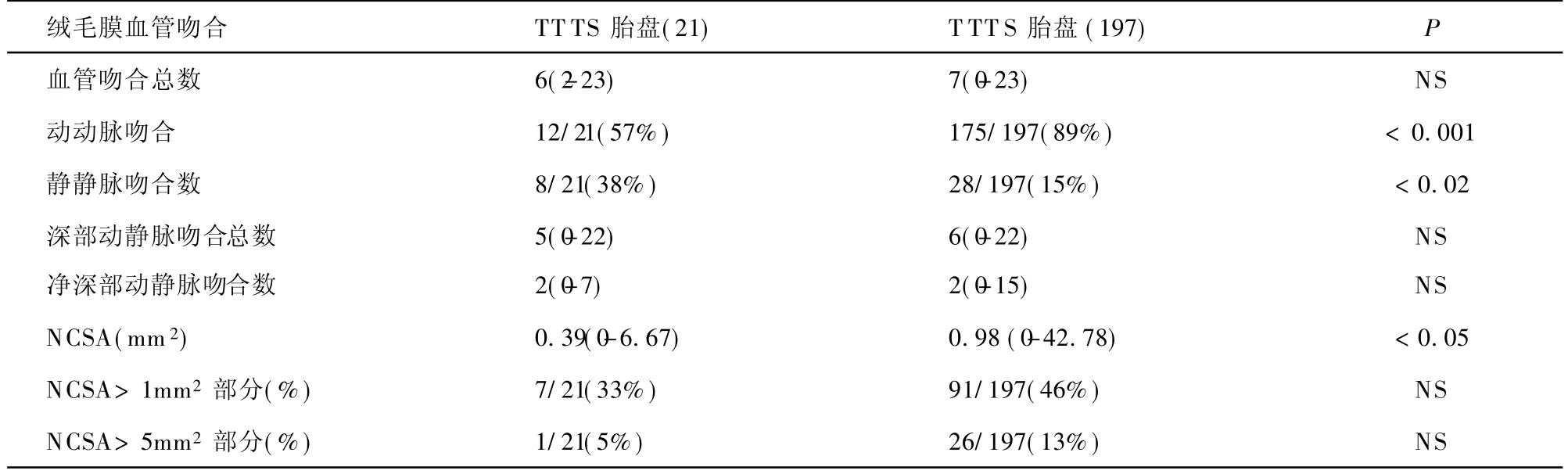
表2b 绒毛膜血管吻合

表3 胎盘检查确诊TTTS的准确性
血液在血管中的流动受许多因素的影响包括:血管直径、血液压力、血液黏度、血管活性因子及各种感受器等。而以往研究(包括该研究),主要针对血管形态学。因此以往从形态学研究得出的结论最终又被形态学研究否定。但这也提示TTTS病因可能并非形态学异常,而是各种非形态学因素。现在已经有一些研究证实这一观点。Bajoria R等和Sooranna SR等分别发现TTTS供血儿体内胰岛素样生长因子-II及瘦素水平较受血儿低,这与胎盘的生长紊乱有关,而与血流无关。Bajoria R、Galea P、Mahieu-Caputo D等还发现血管活性因子脑钠钛(BNP)、内皮素-1及肾素-血管紧张素(RAS)系统异常可能是导致、维持并促使TTTS恶化的原因。
该研究发现双胎间胎盘面积差异>25%及胎盘血管单支分布是TTTS特异性较高的标志。可做如下推论,假设双胎所占胎盘面积分别为A和B。若发生TTTS的风险较小(考虑胎盘共享)应满足:A+B>100%且 A-B<25%。可以得出 B>37.5%。据上述推论单绒双羊双胎时,每个胎儿所占胎盘面积可能应大于37.5%。TTTS胎盘标志为胎盘不均衡分配(双胎间胎盘面积差异>25%)、缺乏AA吻合、脐带帆状附着、血管单支分布等似乎都与胎盘面积有关。这也提示在对于MCDA的双胎胎盘的病理学检查中,要将以上几个指标纳入常规的病理解剖报告中。
胎盘是胎儿-母体进行物质交换的场所。TTTS实质是胎盘异常,包括胎盘血管的构建和功能异常。而正常胎盘的形成需要细胞增殖与新生血管形成两者之间密切协调。而且有多种细胞(如巨噬细胞)和细胞因子(如有血管内皮生长因子(VEGF)、酸性碱性成纤维细胞生长因子(FGF)、转化生长因子(TGF)、血小板源生长因子(PDGF)、胎盘生长因子(PIGF)、肿瘤坏死因子(TNF)、血管生成素(angiopoietins)等共同参与胎盘血管形成的调节。而且胎盘形成是动态变化的过程,不同孕周胎盘血管生成的形态及调节因素是不同的。因此TTTS胎盘异常应该包括形态学异常和非形态学异常。甚至非形态学的异常,包括各种细胞因子和血管活性因子,在TTTS发生发展中可能起决定作用。TTTS胎盘特征也提示TTTS胎盘中可能存在着抗血管生成的因素。
近9%~15%的单绒双羊双胎妊娠并发TTTS,胎儿发病率和死亡率高达70%以上。而至今尚无预测TTTS的理想指标和方法。综合这几年文献,各种血管活性因子和促进血管形成的细胞因子可能是TTTS病因和预测进一步的研究方向。
猜你喜欢
宝藏(2020年4期)2020-11-05
中国生殖健康(2020年6期)2020-02-01
中国生殖健康(2019年2期)2019-08-23
中国临床医学影像杂志(2019年2期)2019-04-25
中国生殖健康(2018年6期)2018-11-06
中国中西医结合皮肤性病学杂志(2016年4期)2016-07-18
中国继续医学教育(2015年2期)2016-01-06
中国医药生物技术(2015年4期)2015-12-26
中国现代医学杂志(2015年26期)2015-12-23
中国当代医药(2015年36期)2015-03-11