DSA与TEE引导经皮PFO封堵术安全性与有效性比较
2024-10-17 00:00孙冲时培轩宋文慧武力舟王海燕
青岛大学学报(医学版) 2024年4期


[摘要]目的比较血管造影(DSA)与经食管超声心动图(TEE)引导下行经皮卵圆孔未闭(PFO)封堵术的可行性、安全性和有效性。
方法2018年1月—2022年12月,山东第一医科大学第一附属医院住院治疗的不明原因脑卒中和药物治疗无效的PFO相关性偏头痛332例,所有病人均接受经皮PFO封堵术治疗。根据其引导方式分为TEE组 101例, DSA组231例;根据病因分为偏头痛组151例和隐匿性脑卒中组181例。回顾性分析病人的临床特征、超声心动图、术中及术后1年随访等临床资料。
结果DSA组和TEE组的手术成功率与手术并发症发生率无显著差异,但TEE组的手术时间更长、住院费用更高(t=5.125,Z=8.265,P<0.001)。偏头痛组和隐匿性脑卒中组的手术成功率和并发症发生率与总体结果相一致。随访1年偏头痛亚组DSA和TEE病人的HIT-6评分差异无统计学意义;隐匿性脑卒中亚组DSA病人复发脑卒中3例(2.2%),而TEE病人无脑卒中复发者,但差异无统计学意义。
结论TEE和DSA引导下经皮PFO封堵术,在手术成功率、并发症发生及术后1年疗效等方面无明显差异,但在手术时长和住院费用方面DSA病人更具优势。
[关键词]卵圆孔,未闭;心血管造影术;超声心动描记术,经食管;偏头痛;卒中;治疗结果
[中图分类号]R541.1;R540.45
[文献标志码]A
[文章编号]2096-5532(2024)04-0528-05doi:10.11712/jms.2096-5532.2024.60.111
[开放科学(资源服务)标识码(OSID)]
[网络出版]https://link.cnki.net/urlid/37.1517.R.20240829.1342.004;2024-08-3017:34:43
Safety and efficacy of digital subtraction angiography versus transesophageal echocardiography in guiding percutaneous patent foramen ovale occlusion
SUN Chong, SHI Peixuan, SONG Wenhui, WU Lizhou, WANG Haiyan
(Department of Medical Ultrasound, The First Affiliated Hospital of Shangdong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Medicine and Health Key Laboratory of Abdominal Medical Imaging, Jinan 250013, China)
; [Abstract]ObjectiveTo investigate the feasibility, safety, and efficacy of digital subtraction angiography (DSA) versus transesophageal echocardiography (TEE) in guiding percutaneous patent foramen ovale (PFO) occlusion.
MethodsA total of 332 patients with PFO-related migraine due to unexplained stroke or no response to pharmacotherapy who were hospitalized in The First Affiliated Hospital of Shandong First Medical University from January 2018 to December 2022 were enrolled, and all patients underwent percutaneous PFO occlusion. According to the guidance method, they were divided into TEE group with 101 patients and DSA group with 231 patients, and according to the etiology, they were divided into migraine group with 151 patients and occult stroke group with 181 patients. A retrospective analysis was performed for the clinical data including clinical features, echocardiog-
raphy, intraoperative data, and one-year postoperative follow-up.
ResultsThere wereno significant differences between the DSA group and the TEE groupin surgical success rate and the incidence rate of surgical complications, but the TEE group had a significantly longer time of operation and significantly higher hospitalcosts (t=5.125,Z=8.265,P<0.001). Surgical success rate and the incidence rate of complications in the migraine group and the occult stroke group were consistent with the overall results. One-year follow-up showed no significant difference in HIT-6 score between the patients undergoing DSA and those undergoing TEE in the migraine subgroup; in the occult stroke subgroup, 3 patients (2.2%) experienced the recurrence of stroke among the patients undergoing DSA, while no patient experienced such recurrence among the patients undergoing TEE, without a significant difference.
ConclusionThere areno significant differences between TEE-and DSA-guided percutaneous PFO occlusion in surgical success rate, the incidence rate of complications, and 1-year postoperative outcome, but patients undergoing DSA tend to have advantages in the time of operation and hospital costs.
[Key words]foramen ovale, patent; angiocardiography; echocardiography, transesophageal; migraine; stroke; treatment outcome
卵圆孔未闭(PFO)是成人中最常见的先天性心脏异常,发生率约25%[1]。在大多数情况下,PFO不需要治疗。但在某些特殊情况下,PFO可能会导致严重并发症,包括卒中和非卒中性疾病,如偏头痛、减压病、斜卧呼吸-直立性低氧血症和系统栓塞等[2-4],这些情况下通常需要治疗。临床上最常见的是PFO相关性脑卒中和偏头痛,目前多个国家制定了PFO相关性卒中治疗指南,推荐对此类病人行PFO封堵治疗[5-8]。对于PFO相关性偏头痛,张玉顺等[9]制定的中国专家共识认为,有心房水平持续性右向左分流、合并房间隔膨出瘤、中大量右向左分流/易栓倾向及先兆性偏头痛病人可能通过PFO封堵治疗获益。血管造影(DSA)和经食管超声心动图(TEE)是目前行经皮PFO封堵术最常用的两种引导方式,但以往对其优劣性研究较少,也未见进行偏头痛、脑卒中的分组研究。本研究旨在评估这两种引导方式的可行性、安全性和有效性,从而为PFO病人选择治疗方式提供依据。
1资料与方法
1.1对象选择
根据现有的指南及专家共识,纳入2018年1月—2022年10月于山东第一医科大学第一附属医院住院治疗的332例接受经皮PFO封堵术病人。纳入标准:①不明原因脑卒中;②药物难治性偏头痛并且未明确其他偏头痛机制;③右心声学造影(c-TTE)为Ⅱ~Ⅲ级。排除标准:①房间隔缺损;②其他原因引起的偏头痛及脑卒中;③心腔内血栓形成,或合并心房颤动(房颤);④合并严重肺动脉高压或者PFO为特殊通道;⑤感染性疾病、妊娠、抗血小板或抗凝治疗禁忌证。其中,DSA引导231例,TEE引导101例。根据病因不同将病人分为偏头痛组151例和隐匿性脑卒中组(脑卒中组)181例。本研究已经完成美国临床注册(clinicaltrials.gov,注册号NCT06192173)。
1.2诊断与评估方法
所有病人经胸超声心动图联合c-TTE检测到Ⅱ~Ⅲ级右向左分流(RLS)[10]。在封堵术前均行TEE检查,观察房间隔解剖结构及心房水平的分流情况。隐源性脑卒中病人均行颅脑CT扫描(或MRI)及脑血管CTA检查、颈动脉和椎动脉超声多普勒检查等,偏头痛病人均行头痛影响测评量表-6(HIT-6)[11]评估偏头痛严重程度。
1.3引导方法及效果评估
DSA组采用表面麻醉穿刺股静脉,选择DSA下经皮经股静脉路径,在右心房内PFO部位进行高压造影确定其位置及大小,选择合适封堵器进行封堵,术前及术后即刻行TTE监测。记录手术时间及透视时间。TEE组在气管插管静脉麻醉下通过TEE二维及彩色多普勒检查明确PFO位置、大小及分流情况,选择合适输送鞘和封堵伞,采用与DSA组相同的手术途径,TEE全程引导封堵过程及术后即刻评估。
这两种引导方式均由高年资及年轻介入科医生各1名和1名超声科医生完成,TEE组额外需要1名麻醉医生。手术即刻成功定义为封堵器顺利置入,超声心动图评估封堵器位置形态良好,对毗邻结构无影响,心房水平无残余分流,无心包积液、无出血、无心律失常。术后常规给予抗血小板治疗,口服阿司匹林(100 mg,每天2次)或阿司匹林(100 mg,每天1次)联合氯吡格雷(75 mg,每天1次)6个月。出院前行TTE及心电图检查。所有病人接受术后12个月的门诊随访,主要内容包括临床表现、TTE及c-TTE、心电图检查等项目,对偏头痛病人记录HIT-6及△HIT-6评分,脑梗死病人是否有卒中复发。手术短中期成功率定义为术后12月封堵器位置形态良好,c-TTE检查显示左心腔微气泡数量<10个/帧,无新发心律失常等。
1.4统计学分析
采用SPSS 22.0软件进行统计学处理。计量资料数据正态分布者采用±s表示,非正态分布者用M(P25~P75)表示,分类变量用频率(占总数的百分比)表示,运用两独立样本t检验、卡方检验、Fisher确切概率法和非参数Mann-Whitney U检验等进行组间比较。所有检验均为双尾检验,以P< 0.05为差异有统计学意义。
2结果
2.1病人基线临床特征及其分组比较
PFO封堵术病人(总样本组)332例,按照病因分为PFO相关脑卒中(脑卒中组)181例,PFO相关性偏头痛(偏头痛组)151例;按照封堵术诱导方式分为DSA组231例,TEE组101例。总样本组、脑卒中组和偏头痛组基线临床特征在不同封堵术诱导方式之间比较,差异均无统计学意义。见表1。所选用的PFO封堵器均为国产封堵器,DSA组84%病人选择最常用的18/25 mm 和25/25 mm封堵器,TEE组93%病人选择这两个型号。
2.2DSA组和TEE组围手术期相关资料比较
DSA组4例病人心房造影未能发现确切PFO而终止手术,TEE组则有2例导管导丝未能通过PFO,但两组手术即刻成功率无统计学差异。TEE组中有2例是DSA引导封堵失败转为TEE引导封堵成功。TEE组病人较DSA组的手术时间更长且住院费用更高,差异均有统计学意义(Z=4.693~8.265,t=3.759~5.125,P<0.001)。两组病人均未出现围手术期房颤、脑缺血及心包积液等并发症。两组病人住院天数无差异。脑卒中亚组和偏头痛亚组围手术期相关指标与总体结果相近。见表2。
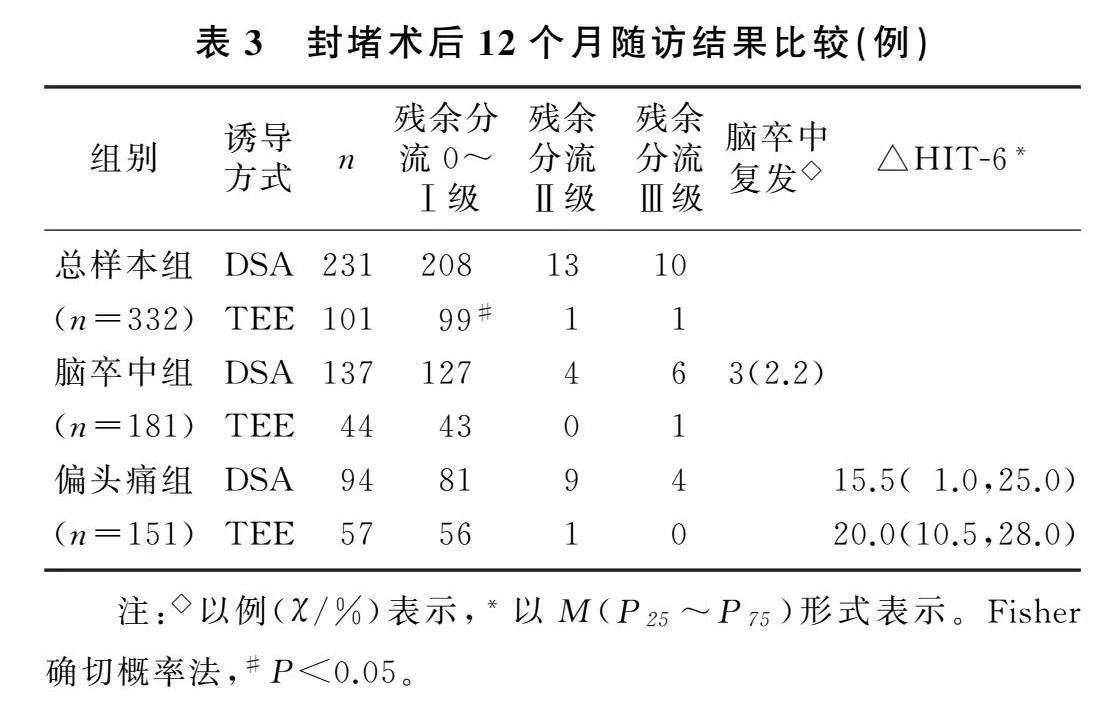
2.3封堵术后12个月随访结果比较
随访12个月结果显示,总体上DSA组病人较TEE组遗留更多Ⅱ级或以上残余右向左分流,差异有统计学意义(Fisher确切概率法,P<0.05)。在偏头痛亚组中,尽管DSA组较TEE组遗留更多Ⅱ级或以上残余右向左分流病人、△HIT-6评分较低,但二者差异均无统计学意义。在隐匿性脑卒中亚组中,尽管DSA引导封堵的病人似乎有较TEE引导者更多出现Ⅱ级或以上残余右向左分流的趋势,以及更高的复发性脑卒中发生率,但二者差异均无统计学意义。见表3。
3讨论
多个国家的PFO封堵指南或专家共识或者多项临床研究均认为,封堵PFO对于预防不明原因脑卒中复发、治疗难治性偏头痛并且不合并其他偏头痛发生机制的病人是有价值的[12-16,9]。本研究对比DSA与TEE的结果显示,DSA组和TEE组手术即刻成功率、短中期成功率与手术并发症发生率无显著差异,但TEE组手术时间更长、住院费用更高。随访12月结果显示,接受两种不同引导方式的偏头痛亚组病人偏头痛改善程度、隐匿性脑卒中亚组复发脑卒中发生率均无明显差异。
本研究所有病人中DSA组与TEE组的手术即刻成功率比较,差异无统计学意义。但TEE相比于DSA可能具有以下优势。①TEE空间分辨率高,可以更直观准确地观察卵圆孔大小、形态、原发隔活动度以及PFO毗邻结构,并可根据3D-TEE测量的卵圆窝大小来选择合适型号的封堵器[17-18]。②在封堵术中TEE可以实时监控并指引导丝、导管精准通过PFO[19-21]。对于通过困难的病人,将输送鞘顶在PFO的右房侧开口处使用导丝反复尝试,成功率更高。本研究中有2例病人在DSA引导下导管无法通过PFO,随后在TEE引导下封堵成功。③TEE可直视观察病人在封堵器置入即刻的形态、位置及残余分流,可及时发现术中并发症,比如卵圆孔内膜夹层、心包积液、封堵器表面血栓形成等[22]。尽管术中TEE引导具有诸多优势,但它也存在局限性,因为TEE引导术中需全身麻醉[23],并且需TEE全程进行术中引导。
本研究中TEE和DSA引导下PFO封堵术的术中及术后短期并发症无显著差异,表明这两种引导方式都是安全可靠的。尽管TEE探头在术中长时间操作可能导致病人咽喉或食管不适,全麻也存在麻醉相关风险,且其总手术时间也会更长,但本研究显示DSA组与TEE组术后住院时间并无明显差异,表明无术中或术后并发症需要额外处理。虽然TEE引导下PFO封堵术的精准度似乎更高,但因DSA具备安全、快速与高效等特点[24],DSA引导仍是目前主流手段。然而,对某些形态特殊PFO、预计手术操作难度大、有放射线禁忌证等病人,仍建议行TEE引导下封堵术。
以往研究将PFO封堵成功定义为封堵器与房间隔贴合良好,术后6个月c-TCD或c-TTE显示左心微气泡<10个/帧[25]。本研究考虑到封堵治疗后6个月内病人持续抗血小板治疗会影响临床疗效评估,故最终将封堵术后12个月获得的超声复查结果作为评判依据。本研究结果表明,所有病人封堵器位置形态良好,对毗邻结构无挤压或磨损,彩色多普勒超声检查提示心房水平无分流,并且在所有病人及偏头痛亚组病人中,TEE引导封堵病人c-TTE显示残余分流发生率明显低于DSA组,考虑可能与根据TEE结果选择封堵器更加适合有关。
多国指南指出,对60岁以下PFO相关性卒中病人强烈建议封堵PFO[26-29]。本研究中隐匿性脑卒中亚组有3例(2.2%)病人术后1年内复发脑卒中,均为DSA引导封堵的病人。虽然近年来PFO封堵术治疗偏头痛仍存在争议,但2023年张玉顺等[9]对国内人群长期研究后制定的专家共识指出,对于药物难治性偏头痛,如果未发现其他引起偏头痛的机制并且有先兆、合并房间隔膨出瘤、RLS为中大量的病人,可以行PFO封堵术。本研究偏头痛亚组中PFO封堵治疗获得令人满意的短中期结果,这与先前研究结果一致[30-31]。
本研究尚存在一些局限性。首先,作为一项回顾性研究,课题设计存在一定缺陷;其次,样本量偏小、单中心研究、术后随访时间较短,未来需要纳入更多受试者的多中心研究以获得更可靠的结果。总之,TEE和DSA引导下的PFO封堵术均安全、可行和有效,仅在手术时长和住院费用这两方面,DSA病人更具优势。这两种引导方式对隐匿性脑卒中和药物难治性偏头痛均取得了良好的治疗效果,值得在临床上推广应用。
[参考文献]
[1]HAGEN P T, SCHOLZ D G, EDWARDS W D. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts[J]. Mayo Clinic Proceedings, 1984,59(1):17-20.
[2]徐亮,周畅,李洁,等. 中青年卵圆孔未闭持续性右向左分流与隐源性脑卒中的相关性分析[J]. 中国循环杂志, 2020,35(2):171-174.
[3]GONNAH A R, BHARADWAJ M S, NASSAR H, et al. Patent foramen ovale: diagnostic evaluation and the role of device closure[J]. Clinical Medicine, 2022,22(5):441-448.
[4]LUC F, PINO P G, PARRINI I, et al. Patent foramen ovale and cryptogenic stroke: integrated management[J]. Journal of Clinical Medicine, 2023,12(5):1952.
[5]张玉顺,蒋世良,朱鲜阳. 卵圆孔未闭相关卒中预防中国专家指南[J]. 心脏杂志, 2021,33(1):1-10.
[6]PRISTIPINO C, SIEVERT H, D’ASCENZO F, et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism[J]. European Heart Journal, 2019,40(38):3182-3195.
[7]MESS S R, GRONSETH G S, KENT D M, et al. Practice advisory update summary: patent foramen ovale and secondary stroke prevention: report of the Guideline Subcommittee of the American Academy of Neurology[J]. Neurology, 2020,94(20):876-885.
[8]DIENER H C, AKAGI T, DURONGPISITKUL K, et al.Closure of the patent foramen ovale in patients with embolic stroke of undetermined source: a clinical expert opinion and consensus statement for the Asian-Pacific Region[J]. International Journal of Stroke: Official Journal of the International Stroke Society, 2020,15(9):937-944.
[9]张玉顺,于生元,董钊,等. 卵圆孔未闭相关非卒中性疾病防治中国专家共识[J/OL]. 心脏杂志, 2024(2):1-10[2024-03-22]. http://kns-cnki-net-https.cnki.tsyxy.qfclo.com: 2222/kcms/detail/61.1268.R.20231115.1413.022.html.
[10]YANG X X, WANG H, WEI Y J, et al. Diagnosis of patent foramen ovale: the combination of contrast transcranial Doppler, contrast transthoracic echocardiography, and contrast transesophageal echocardiography[J]. Bio Med Research International, 2020, 2020: 8701759.
[11]李舜伟,李焰生,刘若卓,等. 中国偏头痛诊断治疗指南[J]. 中国疼痛医学杂志, 2011,17(2):65-86.
[12]FAVILLA C G, MESS S R. Patent foramen ovale and stroke: current evidence and treatment options[J]. Current Opinion in Neurology, 2020,33(1):10-16.
[13]YANG J, LEI W R, WANG J W, et al. Transesophageal echocardiography-guided percutaneous closure of the patent foramen ovale only uses the sheath[J]. Cardiovascular Diagnosis and Therapy, 2023,13(4):728-735.
[14]EICHELMANN A, KUBINI R, NACHOSKI D, et al. Patent foramen ovale closure versus drug therapy in patients over 60 years and a follow-up of 5 years[J]. Clinical Cardiology, 2024,47(3):e24251.
[15]MI Z Y, HE G, LI C, et al. Efficacy and safety of transeso-
phageal ultrasound-guided patent foramen ovale closure for migraine in adolescents[J]. Frontiers in Pediatrics, 2023,11: 1296825.
[16]FARJAT-PASOS J I, CHAMORRO A, LANTHIER S, et al. Cerebrovascular events in older patients with patent foramen ovale: current status and future perspectives[J]. Journal of Stroke, 2023,25(3):338-349.
[17]SPERLONGANO S, GIORDANO M, CICCARELLI G, et al. Advances in percutaneous patent foramen ovale closure: from the procedure to the echocardiographic guidance[J]. Journal of Clinical Medicine, 2022,11(14):4001.
[18]王晓静,王岩青. 实时三维经食管超声心动图在卵圆孔未闭封堵术中的独特优势[J]. 医学影像学杂志, 2022,8(8):1281-1284.
[19]BARTEL T, MULLER S. Device closure of interatrial communications: peri-interventional echocardiographic assessment[J]. European Heart Journal Cardiovascular Imaging, 2013,14(7):618-624.
[20]VITARELLI A. Patent foramen ovale: pivotal role of transesophageal echocardiography in the indications for closure, assessment of varying anatomies and post-procedure follow-up[J]. Ultrasound in Medicine & Biology, 2019,45(8):1882-1895.
[21]ZHANG S S, GAO Z Q, CHEN H, et al. Effects of morphological characteristics of patent foramen ovale by transesophageal echocardiography on minimalist transcatheter closure in Southern China[J]. Echocardiography, 2023,40(7):647-656.
[22]RAT N, MUNTEAN I, OPINCARIU D, et al. Cardiovas-
cular imaging for guiding interventional therapy in structural heart diseases[J]. Current Medical Imaging Reviews, 2020,16(2):111-122.
[23]HAHN R T, ABRAHAM T, ADAMS M S, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American society of echocardiography and the society of cardiovascular anesthesiologists[J]. Journal of the American Society of Echocardiography, 2013,26(9):921-964.
[24]YANG T, BUTERA G, OU-YANG W B, et al. Percutaneous closure of patent foramen ovale under transthoracic echocardiog-raphy guidance-midterm results[J]. Journal of Thoracic Di-sease, 2019,11(6):2297-2304.
[25]FURLAN A J, REISMAN M, MASSARO J, et al. Closure or medical therapy for cryptogenic stroke with patent foramen ovale[J]. The New England Journal of Medicine, 2012,366(11):991-999.
[26]CABANES L, MAS J L, COHEN A, et al. Atrial septal aneurysm and patent foramen ovale as risk factors for crypto-
genic stroke in patients less than 55 years of age. A study using transesophageal echocardiography[J]. Stroke, 1993,24(12):1865-1873.
[27]WEIMAR C, HOLLE D N, BENEMANN J, et al. Current management and risk of recurrent stroke in cerebrovascular patients with right-to-left cardiac shunt[J]. Cerebrovascular Di-
seases, 2009,28(4):349-356.
[28]ALBART S A, YUSOF KHAN A H K, WAN ZAIDI W A, et al. Management of patent foramen ovale in embolic stroke of undetermined source patients: Malaysian experts' consensus[J]. The Medical Journal of Malaysia, 2023,78(3):389-403.
[29]KLEINDORFER D O, TOWFIGHI A, CHATURVEDI S, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American heart association/american stroke association[J]. Stroke, 2021,52(7):e364-e467.
[30]付强,赵性泉,曹京波,等. 卵圆孔未闭封堵术对伴卵圆孔未闭的偏头痛患者的疗效[J]. 山西医科大学学报, 2018,49(12):1415-1418.
[31]王云霞,邱恩超,王广义,等. 卵圆孔未闭与偏头痛的关系及其封堵术后的临床疗效观察[J]. 中国疼痛医学杂志, 2019,25(5):344-350.
(本文编辑于国艺)