
Association of age at diagnosis of diabetes with subsequent risk of age-related ocular diseases and vision acuity
2024-04-22 00:59SiTingYeXianWenShangYuHuangSusanZhuZhuoTingZhuXueLiZhangWeiWangShuLinTangZongYuanGeXiaoHongYangMingGuangHe
World Journal of Diabetes 2024年4期
Si-Ting Ye,Xian-Wen Shang,Yu Huang,Susan Zhu,Zhuo-Ting Zhu,Xue-Li Zhang,Wei Wang,Shu-Lin Tang,Zong-Yuan Ge,Xiao-Hong Yang,Ming-Guang He
Abstract BACKGROUND The importance of age on the development of ocular conditions has been reported by numerous studies.Diabetes may have different associations with different stages of ocular conditions,and the duration of diabetes may affect the development of diabetic eye disease.While there is a dose-response relationship between the age at diagnosis of diabetes and the risk of cardiovascular disease and mortality,whether the age at diagnosis of diabetes is associated with incident ocular conditions remains to be explored.It is unclear which types of diabetes are more predictive of ocular conditions.AIM To examine associations between the age of diabetes diagnosis and the incidence of cataract,glaucoma,age-related macular degeneration (AMD),and vision acuity.METHODS Our analysis was using the UK Biobank.The cohort included 8709 diabetic participants and 17418 controls for ocular condition analysis,and 6689 diabetic participants and 13378 controls for vision analysis.Ocular diseases were identified using inpatient records until January 2021.Vision acuity was assessed using a chart.RESULTS During a median follow-up of 11.0 years,3874,665,and 616 new cases of cataract,glaucoma,and AMD,respectively,were identified.A stronger association between diabetes and incident ocular conditions was observed where diabetes was diagnosed at a younger age.Individuals with type 2 diabetes (T2D) diagnosed at < 45 years [HR (95%CI): 2.71 (1.49-4.93)],45-49 years [2.57 (1.17-5.65)],50-54 years [1.85 (1.13-3.04)],or 50-59 years of age [1.53 (1.00-2.34)] had a higher risk of AMD independent of glycated haemoglobin.T2D diagnosed < 45 years [HR (95%CI): 2.18 (1.71-2.79)],45-49 years [1.54 (1.19-2.01)],50-54 years [1.60 (1.31-1.96)],or 55-59 years of age [1.21 (1.02-1.43)] was associated with an increased cataract risk.T2D diagnosed < 45 years of age only was associated with an increased risk of glaucoma [HR (95%CI): 1.76 (1.00-3.12)].HRs (95%CIs) for AMD,cataract,and glaucoma associated with type 1 diabetes (T1D) were 4.12 (1.99-8.53),2.95 (2.17-4.02),and 2.40 (1.09-5.31),respectively.In multivariable-adjusted analysis,individuals with T2D diagnosed < 45 years of age [β 95%CI: 0.025 (0.009,0.040)] had a larger increase in LogMAR.The β (95%CI) for LogMAR associated with T1D was 0.044 (0.014,0.073).CONCLUSION The younger age at the diagnosis of diabetes is associated with a larger relative risk of incident ocular diseases and greater vision loss.
Key Words: Diabetes;Age at diagnosis;Cataract;Glaucoma;Age-related macular disease;Vision acuity
INTRODUCTION
Although the age-standardised prevalence of avoidable vision impairment did not change,the global number of cases increased substantially due to the increasing aging population[1].Cataract,glaucoma,and age-related macular degeneration (AMD) are the first,second,and fourth leading global causes of blindness in individuals aged 50 years and older,which accounted for 15.2 million,3.6 million and 1.8 million cases,respectively[1,2].Therefore,it is imperative to identify the important determinants for these ocular conditions.
Previous evidence has highlighted the importance of diabetes in the development of ocular conditions[3,4].Diabetes has been linked to numerous ocular conditions,including cataract[5],glaucoma[6],and AMD[7].The United Kingdom Million Women Study,involving 1312051 postmenopausal women,demonstrated that diabetes was an important risk factor for cataract surgery[8].In contrast,evidence suggests diabetes is not among the leading predictors for glaucoma[9,10],and other studies did not find a significant association between diabetes and glaucoma[11].Previous studies have been inconsistent regarding the association of diabetes with AMD[7].Several studies have demonstrated a positive relationship between diabetes and AMD[12,13],but more studies did not find a significant association[14-18].
The importance of age on the development of ocular conditions has been reported by numerous studies[5,7,9,10].Diabetes may have different associations with different stages of ocular conditions[19],and the duration of diabetes may affect the development of diabetic eye disease[3].While there is a dose-response relationship between the age at diagnosis of diabetes and the risk of cardiovascular disease and mortality[20,21],whether the age at diagnosis of diabetes is associated with incident ocular conditions remains to be explored.It is unclear which types of diabetes are more predictive of ocular conditions.
It is important to identify the life stage at which a diagnosis of diabetes is associated with the highest risk of major ocular conditions for the prevention or screening of these conditions.Using the UK Biobank,we sought to examine the association between age at the diagnosis of diabetes and the incidence of cataract,glaucoma,and AMD.
MATERlALS AND METHODS
Study population
The UK Biobank is a population-based cohort of more than 500000 participants aged 40-73 years at baseline,recruited between 2006 and 2010 from one of the 22 assessment centres across England,Wales,and Scotland[22].The design and population of the UK Biobank study have been described in detail elsewhere[22].The UK Biobank Study’s ethical approval had been granted by the National Information Governance Board for Health and Social Care and the NHS North West Multicenter Research Ethics Committee.All participants provided informed consent through electronic signature at the baseline assessment.The data used in this study is available in the UK Biobank database under the application number of 62443.
Population selection for eye disease analysis
Individuals with missing data on self-reported eye health (n=327891),or those with ocular diseases (n=26320) at baseline were excluded from the analysis.After the exclusion of individuals with missing values on the age at the diagnosis of diabetes or with other type of diabetes rather than type 1 diabetes (T1D) and type 2 diabetes (T2D,n=264),7917 participants with T2D were divided into six groups according to the age at diagnosis: < 45,45-49,50-54,55-59,60-64,and ≥ 65 years.For each diabetic participant,two controls were randomly selected from those without diabetes at baseline using propensity scores matched by age,gender,ethnicity,education,household income,physical activity,smoking,alcohol consumption,sleep duration,depression,hypertension,heart disease,stroke,body mass index (BMI),highdensity lipoprotein cholesterol (HDL-C),low-density lipoprotein cholesterol (LDL-C),and triglycerides.This analysis was conducted for each diabetes diagnosis age group.The same method was used to randomly select controls for T1D patients (n=792,Figure 1).

Figure 1 Flowchart for population selection for analysis of ocular conditions from the UK Biobank. Propensity score matching was to select two controls for each diabetic participant.The analysis was conducted for age groups of diabetes diagnosis separately.The median age at diagnosis type 1 was 17 years.Propensity score accounted for age,gender,ethnicity,education,household income,physical activity,smoking,alcohol consumption,sleep duration,depression,hypertension,heart disease,stroke,body mass index,high-density lipoprotein cholesterol,low-density lipoprotein cholesterol,and triglyceride.AMD: Age-related macular degeneration;T1D: Type 1 diabetes;T2D: Type 2 diabetes.
Population selection for vision impairment analysis
Among 117252 individuals who had their vision acuity assessed,7274 had diabetes at baseline.After excluding individuals with missing values on diabetes diagnosis age or with other type of diabetes rather than T1D/T2D (n=585),6192 with T2D were divided into six groups according to the diagnosis age: < 45,45-49,50-54,55-59,60-64,and ≥ 65 years.The same method was used to select controls for individuals with T1D (Supplementary Figure 1).
Age at diagnosis of diabetes
First,participants were classified as diabetic if they reported that a doctor had ever told them that they had diabetes (Field code: 2443).For those with a self-reported diagnosis of diabetes,they were asked a follow-up question “What was your age when diabetes was first diagnosed?” Participants with a potentially abnormal age at the diagnosis of diabetes were asked to confirm.Algorithms based on self-reported medical history and medication were used to identify T1D and T2D[23].Furthermore,the codes for international classification diseases (ICD) were used to define T1D/T2D (Supplementary Table 1).The age at the diagnosis of diabetes (years) was then computed by subtracting the birth date from the initial diagnosed date divided by 365.25.
Ascertainment of ocular conditions
Individuals were classified as having AMD (Field code: 1528),cataract (1278),or glaucoma (1277) if they reported a diagnosis of the corresponding conditions.Cases of ocular conditions were also identified using hospital inpatient records based on ICD codes (Supplementary Table 1).Furthermore,we used surgical procedures by OPCS4 to identify cataract events (codes: C71.2 or C75.1)[24].The onset date of ocular condition was defined as the earliest recorded code date regardless of source.Person-years were calculated from the date of baseline assessment to the date of onset ocular condition,date of death,or the end of follow-up (December 31,2020 for England and Wales and January 31,2021 for Scotland),whichever came first.
Vision acuity test
The baseline vision acuity examination was performed among a sub-cohort of the UK Biobank from June 2009 to July 2010.The procedure for the vision acuity test has been described in detail elsewhere[25].Presenting distance vision acuity was measured at 4 m or at 1 m (if a participant was unable to read) using the logarithm of the minimum angle of resolution (LogMAR) chart on a computer screen.Vision was defined as the presenting vision acuity in the better-seeing eye in the analysis.
Covariates
BMI was calculated as weight in kilograms divided by the square of height in meters.A touchscreen computer was used to collect information,including age,gender,education,income,smoking,alcohol consumption,and sleep duration.Metabolic equivalent-hours/week of physical activity during work and leisure time was estimated using specific questions[26].Sleep duration was categorized into three groups: < 7,7-9,and > 9 h[27].
Hypertension,depression,stroke,and heart disease at baseline were defined based on self-reported data.Glycated haemoglobin (HbA1c) was measured using high-performance liquid chromatography on a Bio-Rad Variant II Turbo.Lipids,including total cholesterol,HDL-C,LDL-C,and triglycerides,were measured by direct enzymatic methods (Konelab,Thermo Fisher Scientific,Waltham,Massachusetts).
Statistical analysis
T-test was used to test the difference in continuous variables and Chi-square test in categorical variables between diabetic participants and controls in each diabetes diagnosis age group.
The HR with 95%CIs for incident ocular condition associated with T1D and age at diagnosis of T2D was estimated using Cox proportional hazard regression models.The multivariable analysis included adjustment for matching factors (propensity score) and the full model further incorporated concurrent HbA1c.This analysis was separately conducted for incidence of cataract,cataract surgery,glaucoma,and AMD.The analysis was not performed for types of glaucoma or AMD due to their low incidence.
General linear regression models were used to test the difference in LogMAR between diabetic participants and controls for each diagnosis age group.The multivariable analysis included adjustments for matching factors (propensity score).The association between age at the diagnosis of diabetes and intraocular pressure (IOP) was examined using general linear regression models.
A sensitivity analysis was conducted to examine whether the association between age at the diagnosis of T2D and ocular conditions and vision acuity was independent of duration of diabetes.In this analysis,two controls for each T2D patient were randomly selected using propensity score matching based on the same factors as depicted in Figure 1 and Supplementary Figure 1,without stratification by the age at the diagnosis of diabetes.The age at the diagnosis of T2D,treated as a categorical variable (< 45,45-49,50-54,55-59,60-64,and ≥ 65 years),was analysed to assess the association between the age at the diagnosis of diabetes and ocular conditions and vision acuity.
Missing values for categorical variables were assigned as a single category.Missing values for continuous covariates were imputed with the mean.
Data analyses were conducted using SAS 9.4 for Windows (SAS Institute Inc.),and allPvalues were two-sided,with statistical significance set at < 0.05.
RESULTS
Baseline characteristics
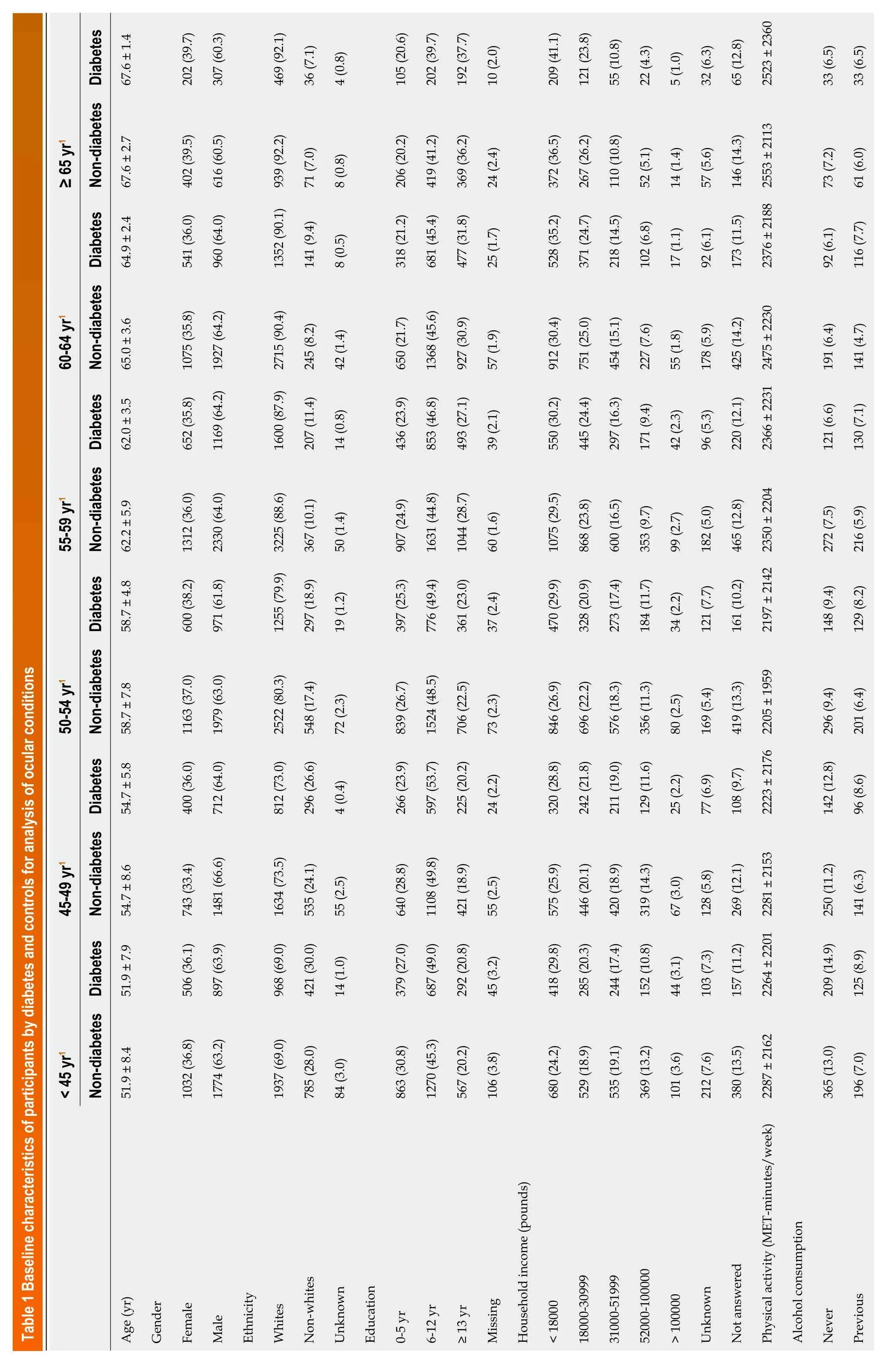
For ocular condition analysis,26127 participants (36.9% females) aged 40-70 (mean ± SD: 59.1 ± 8.2) years old were included in the analysis.Diabetic participants had higher HbA1c,and education levels compared to the controls.No significant difference in other characteristics between the two groups were observed (Table 1).Individuals with T1D had higher HbA1c but did not differ in other characteristics compared to the controls (Supplementary Table 2).
For vision acuity analysis,20067 participants (37.8% females) aged 40-70 years (mean ±S D: 59.9 ± 7.9),were included.Diabetic participants across all age groups of diabetes diagnosis had higher HbA1c than the controls (Table 2).Individuals with T1D were more likely to have a normal sleep duration and higher HbA1c compared to the controls (Supplementary Table 3).
Incidence of ocular conditions
Over a median follow-up of 11.0 years (interquartile range: 10.7-11.5),3874 new cases of cataract,665 new cases of glaucoma,and 616 new cases of AMD were identified.
Age at diagnosis of diabetes and incident AMD,cataract,and glaucoma
As shown in Figure 2,the relative risk for incident AMD associated with diabetes decreased with the increasing age at diagnosis of diabetes.In the multivariable-adjusted analysis,T2D diagnosed at age of < 45 [HR (95%CI): 2.71 (1.49-4.93)],45-49 [2.57 (1.17-5.65)],50-54 [1.85 (1.13-3.04)],or 55-59 years [1.53 (1.00-2.34)] was associated with a higher risk of incident AMD.T1D [HR (95%CI): 4.12 (1.99-8.53)] was associated with an increased risk of AMD independent of concurrent HbA1c.
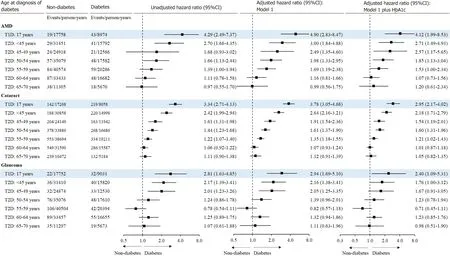
Figure 2 Risk for ocular conditions associated with age at diagnosis of diabetes. Cox proportional hazard regression models were used to examine the association between diabetes and incident ocular condition for each group of diabetes diagnosis age.Model 1 was adjusted for age,gender,ethnicity,income,education,alcohol consumption,physical activity,sleep duration,smoking,body mass index,depression,hypertension,heart disease,stroke,high-density lipoprotein cholesterol,low-density lipoprotein cholesterol,and triglyceride.Central squares of each horizontal line represent the hazard ratio for each subgroup.Horizontal lines indicate the range of the 95%CI.The vertical dash lines indicate the hazard ratio of 1.0.AMD: Age-related macular degeneration;T1D: Type 1 diabetes;T2D: Type 2 diabetes;HbA1C: Glycated haemoglobin.
Similarly,the association between diabetes and glaucoma was dependent on the age at diagnosis of diabetes.After adjustment for HbA1c and other covariates,only diabetes diagnosed at age of < 45 years only [HR (95%CI): 1.76 (1.00-3.12)] was associated with an increased risk of glaucoma.The multivariable-adjusted HR (95%CI) for glaucoma associated with T1D was 2.40 (1.09-5.31).
In the multivariable-adjusted model,the HRs (95%CIs) for incident cataract associated with diabetes diagnosed at < 45,45-49,50-54,and 55-59 years of age were 2.18 (1.71-2.79),1.54 (1.19-2.01),1.60 (1.31-1.96),and 1.21 (1.02-1.43),respectively.T1D was independently associated with an increased risk of incident cataract [2.95 (2.17-4.02)].
As shown in Supplementary Figure 2,T2D diagnosed at < 45,45-49,50-54,and 55-59,but not 60-64 or ≥ 65 years of age was associated with an increased risk of cataract surgery,where individuals with T2D diagnosed < 45 years had the highest excess risk of cataract surgery [HR (95%CI): 2.67 (1.88-3.79)].The multivariable-adjusted HR (95%CI) for cataract surgery associated with T1D was 4.63 (3.10-6.93).
Age at diagnosis of diabetes and vision acuity
After adjustment for covariates and HbA1c,individuals with T2D diagnosed at age of < 45 [β 95%CI: 0.025 (0.009,0.040)],and 50-54 years [0.016 (0.002,0.029)] had higher LogMAR compared to the corresponding controls.T1D was associated with a larger LogMAR [0.044 (0.015,0.073),Figure 3].
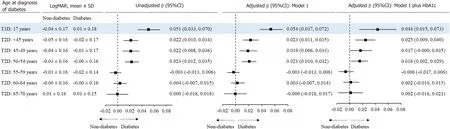
Figure 3 Vision acuity associated with age at diagnosis of diabetes. General linear regression models were used to test the difference in LogMAR between diabetic participants and controls for each group of diabetes diagnosis age.Model 1 was adjusted for age,gender,ethnicity,income,education,alcohol consumption,physical activity,sleep duration,smoking,BMI,depression,hypertension,heart disease,stroke,high-density lipoprotein cholesterol,low-density lipoprotein cholesterol,and triglyceride.Central squares of each horizontal line represent the β for each subgroup.Horizontal lines indicate the range of the 95%CI.The vertical dash lines represent the β of 0.T1D: Type 1 diabetes;T2D: Type 2 diabetes;HbA1C: Glycated haemoglobin.
Age at diagnosis of diabetes and IOP
As shown in Figure 4,individuals with T2D diagnosed at < 45 [β (95%CI): 0.88 (0.59,1.18) mmHg],45-49 [0.86 (0.53,1.18) mmHg],and 50-54 years of age [0.78 (0.52,1.05) mmHg] had higher IOP compared with the controls.The β (95%CI) for IOP associated with T1D was larger [1.15 (0.73,1.56) mmHg].

Figure 4 lntraocular pressure associated with age at diagnosis of diabetes. General linear regression models were used to test the difference in intraocular pressure between diabetic participants and controls for each group of diabetes diagnosis age.Model 1 was adjusted for age,gender,ethnicity,income,education,alcohol consumption,physical activity,sleep duration,smoking,body mass index,depression,hypertension,heart disease,stroke,high-density lipoprotein cholesterol,low-density lipoprotein cholesterol,and triglyceride.T2D: Type 2 diabetes;IOP: Intraocular pressure.
Sensitivity analysis
Individuals with diabetes diagnosed at < 50 years of age were younger but had a higher incidence of ocular diseases compared with controls (Supplementary Figure 3).A larger HR was observed for those with diabetes diagnosed at older age.After adjustment for covariates,the association was reversed with diabetes diagnosed at younger age associated with a larger HR.This trend remained consistent after further adjustment for diabetes duration (Figure 5).Individuals with diabetes diagnosed at < 45,45-49,or 50-54 years of age were younger and had higher LogMAR compared with controls (Supplementary Figure 4).Older age at the diagnosis of diabetes was associated with a larger increase in LogMAR compared with controls.However,after adjustment for covariates,diabetes diagnosed at a younger age was associated with a larger increase in LogMAR (Supplementary Figure 5).
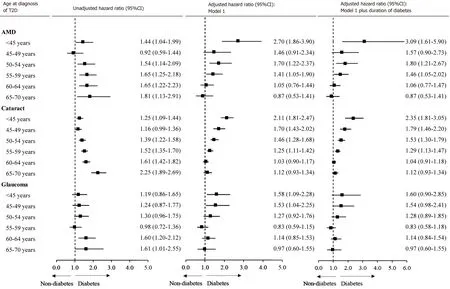
Figure 5 Risk for ocular conditions associated with age at diagnosis of diabetes with the same reference. Sensitivity analysis was conducted to randomly select controls for each individual with type 2 diabetes with all diabetic patients as a whole.Cox proportional hazard regression models were used to estimate hazard ratios for ocular conditions associated with age at diagnosis of diabetes with controls as the reference for each group of diabetes diagnosed age.The multivariable model was adjusted for age,gender,ethnicity,income,education,alcohol consumption,physical activity,sleep duration,smoking,body mass index,depression,hypertension,heart disease,high-density lipoprotein cholesterol,low-density lipoprotein cholesterol,triglyceride,and glycated haemoglobin.Central squares of each horizontal line represent the hazard ratio for each subgroup.Horizontal lines indicate the range of the 95%CI.The vertical dash lines indicate the hazard ratio of 1.0.T2D: Type 2 diabetes;AMD: Age-related macular degeneration.
DISCUSSION
This large prospective cohort study demonstrated that younger age at diagnosis of diabetes was associated with a larger relative risk for cataract, glaucoma, and AMD independent of concurrent HbA1c levels. Individuals with T2D diagnosed before the age of 45 years were more than twice as likely to develop these ocular conditions, while those with T1D exhibited a more pronounced relative risk. Similarly, T2D diagnosed before the age of 55 years and T1D were associated with an increased LogMAR. Sensitivity analysis suggests these associations are independent of duration of diabetes.
Diabetes is one of the most important determinants for cataract[8,28,29]. We found that diabetes was associated with an increased risk of incident cataract, and in particular diabetes diagnosed at < 45 years of age had larger excessive risk of cataract. To our knowledge, no previous study has investigated the impact of age at diagnosis of diabetes on the association between diabetes and cataract. However, several studies have shown that the association between diabetes and cataract was stronger among younger than older adults[28-30]. In a cross-sectional analysis, longer duration of diabetes was associated with a higher prevalence of cataract[28]. These studies provide indirect evidence for the rationale of our findings that younger age at diagnosis of diabetes was associated with a larger excess risk of cataract.
Previous studies have been inconsistent on the association between diabetes and glaucoma.Although a meta-analysis showed that diabetes was associated with a higher risk of glaucoma [relative risk (95%CI): 1.36 (1.25-1.50)],only three out of seven prospective studies included in the meta-analysis found a significant association between diabetes and glaucoma[11].The lack of significance in some studies may be attributed to a relatively short duration of diabetes[31].We found individuals with T1D or T2D diagnosed before the age of 45 years but not at 45 years or older had a higher risk of glaucoma.This is consistent with previous studies showing controversial associations between diabetes and glaucoma.It is possible that cumulative exposure to hyperglycemia from an early life may contribute to increased IOP[32],thus elevating the risk of glaucoma.This is supportive by further analysis demonstrating that diabetes diagnosed at a younger age was associated with a larger increase in IOP.
A meta-analysis showed that diabetes was associated with an increased risk of incident AMD [relative risk (95%CI): 1.05 (1.00-1.11)],although the effect size is small[19].Among 7 cohort studies in this meta-analysis,only one study reported a significant association[33].Another prospective study (not included in this meta-analysis) of 71904 patients with diabetes and 270213 patients without diabetes found no significant association between diabetes and incident AMD[34].A recent prospective study even found that diabetes was associated with a decreased progression of AMD[35].However,we found that diabetes diagnosed at a younger age but not at an older age was associated with an increased risk of AMD.This finding may offer an explanation for the lack of significant associations reported in most previous studies.Notably,previous studies often combined individuals with diabetes diagnosed at both younger and older ages,which may introduce a bias towards a null association.
Whether the association between diabetes and incident cataract,glaucoma,or AMD is moderated by the age at diagnosis of diabetes has not been reported in previous studies.However,our study is consistent with a cross-sectional study of 3322 individuals demonstrating that early-onset T2D was associated with a higher prevalence of diabetic retinopathy[36].Likewise,diabetes diagnosed at a younger age was associated with a larger excess risk of cardiovascular disease and mortality[20].Our further analysis showed that diabetes diagnosed at < 50 years,but not ≥ 50 years of age was associated with decreased vision.The potential effect of diabetes on the development of ocular conditions and vision loss is independent of HbA1c,highlighting the importance of the age at diabetes diagnosis rather than management of diabetes in this association.T1D was associated with a larger effect size for ocular conditions compared with T2D,even when diagnosed at a younger age.The more potentially harmful effect of T1D may stem from its longer duration of hyperglycaemia and insulin dependency,leading to more extensive damage to blood vessels and nervous system.
The mechanisms undelying the association between a younger age at the diagnosis of diabetes and ocular conditions and vision loss remain largely unknown.A prospective study has shown that T2D developed at a younger age was associated with a higher risk of obesity,worse lipid profiles and higher HbA1c,and a faster deterioration in glycaemic control compared to those with diabetes onset at an older age[37].These markers have been shown to be important determinants for cataract[38] and glaucoma[31,39] among diabetic patients.This may indicate that early-onset diabetes may represent a more pathogenic condition than late-onset disease for the development of ocular conditions[37].Furthermore,cumulative exposure to diabetes from early to middle adulthood may exert substantial adverse effects on the development of ocular conditions[40].The stronger association between early-onset diabetes and ocular conditions may also be attributed to the shared genetics between diabetes and ocular conditions[41-43].However,the clear pathogenesis of ocular conditions,especially AMD due to diabetes,needs further exploration in research.
To the best of our knowledge,this is the first prospective cohort study to examine the association of age at the diagnosis of diabetes with main ocular conditions.There are several potential limitations in our study.Firstly,some cases of incident ocular conditions may not be captured using inpatient data.Secondly,it is possible that some controls may have developed diabetes during follow-up,which is more likely to bias the associations towards the null.Thirdly,a large proportion of the individuals without eye health data in the UK biobank cohort were excluded from the analysis.This may limit the generalizability of our findings to the whole population.
CONCLUSlON
In conclusion,our findings suggest the age at the diagnosis of diabetes plays an important role in the association between diabetes and incident cataract,glaucoma,and AMD as well as vision.A younger age at the diagnosis of diabetes was associated with larger excessive relative risk for ocular conditions and larger vision loss.T1D appears to have potentially more harmful effects.
ARTlCLE HlGHLlGHTS
Research background
Diabetes has been linked to numerous ocular conditions,including cataract,glaucomaand age-related macular degeneration (AMD).Several studies have demonstrated a positive relationship between diabetes and AMD,but more studies did not find a significant association.Diabetes may have different associations with different stages of ocular conditions,and the duration of diabetes may affect the development of diabetic eye disease.It is important to identify the life stage at which a diagnosis of diabetes is associated with the highest risk of najor ocular conditions for the prevention or screening of these conditions.
Research motivation
To examine associations between the age of diabetes diagnosis and the incidence of cataract,glaucoma,AMD,and vision acuity.It is important to identify the life stage at which a diagnosis of diabetes is associated with the highest risk of najor ocular conditions for the prevention or screening of these conditions.
Research objectives
To examine associations between the age of diabetes diagnosis and the incidence of cataract,glaucoma,AMD,and vision acuity.A stronger association between diabetes and incident ocular conditions was observed where diabetes was diagnosed at a younger age.It is important to identify the life stage at which a diagnosis of diabetes is associated with the highest risk of major ocular conditions for the prevention or screening of these conditions,and the clear pathogenesis of ocular conditions,needs further exploration in research.
Research methods
This is the first prospective cohort study to examine the association of age at the diagnosis of diabetes with main ocular conditions.Our analysis was using the UK Biobank.The cohort included 8709 diabetic participants and 17418 controls for ocular condition analysis,and 6689 diabetic participants and 13378 controls for vision analysis.Ocular diseases were identified using inpatient records until January 2021.Vision acuity was assessed using a chart.
Research results
This large prospective cohort study demonstrated that younger age at diagnosis of diabetes was associated with a larger relative risk for cataract,glaucoma,and AMD independent of concurrent glycated haemoglobin levels.Individuals with type 2 diabetes (T2D) diagnosed before the age of 45 years were more than twice as likely to develop these ocular conditions,while those with type 1 diabetes (T1D) exhibited a more pronounced relative risk.Similarly,T2D diagnosed before the age of 55 years and T1D were associated with an increased LogMAR.However,the clear pathogenesis of ocular conditions,especially AMD due to diabetes,needs further exploration in research.
Research conclusions
Our findings suggest the age at the diagnosis of diabetes plays an important role in the association between diabetes and incident cataract,glaucoma,and AMD as well as vision.A younger age at the diagnosis of diabetes was associated with larger excessive relative risk for ocular conditions and larger vision loss.T1D appears to have potentially more harmful effects.
Research perspectives
Investigated the impact of age at diagnosis of diabetes on the association between diabetes and cataract,glaucoma,AMD,and vision acuity,by the more detailed breakdown of factors.To analyse more about the shared genetics between diabetes and ocular conditions.
ACKNOWLEDGEMENTS
This research has been conducted using the UK Biobank Resource under Application Number (62443,62525,62491,94372,105658).We thank the participants of the UK Biobank.We thank the language proofreading by Shahin Alam.
FOOTNOTES
Co-first authors:Si-Ting Ye and Xian-Wen Shang.
Co-corresponding authors:Xiao-Hong Yang and Ming-Guang He.
Author contributions:Shang XW,Yang XH,and He MG conceived the study;Shang XW did the literature search and analysed the data;Ye ST,Shang XW,Huang Y,Zhu S,Zhu ZT,and He MG contributed to key data interpretation;Ye ST and Shang XW wrote the manuscript;Ye ST,Shang XW,Huang Y,Zhu S,Zhu ZT,Zhang XL,Wang W,Tang SL,Ge ZY,Yang XH,and He MG critically revised the manuscript.Ye ST is a clinician who identified the clinical problem,provided clinical background,and facilitated the discussion.Shang XW is a statistician who conducted the analysis.Additionally,Ye ST and Shang XW collaborated on drafting the manuscript.Therefore,Ye ST and Shang XW made equal contributions to this work and are co-first authors.He MG provided the funding and the data source,while Yang XH established the research team for this project.They jointly supervised this work.Therefore,they are both considered co-corresponding authors.
Supported byNational Natural Science Foundation of China,No.32 200545;The GDPH Supporting Fund for Talent Program,No.KJ012020633 and KJ012 019530;Science and Technology Research Project of Guangdong Provincial Hospital of Chinese Medicine,No.YN2022GK04.
lnstitutional review board statement:The UK Biobank Study’s ethical approval had been granted by the National Information Governance Board for Health and Social Care and the NHS North West Multicenter Research Ethics Committee.The data used in this study is available in the UK Biobank database under the application number of 62443.
lnformed consent statement:All participants provided informed consent through electronic signature at the baseline assessment.
Conflict-of-interest statement:The authors have no conflicts of interest to declare that are relevant to the content of this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Si-Ting Ye 0009-0004-2882-5298;Ming-Guang He 0000-0002-6912-2810.
S-Editor:Lin C
L-Editor:A
P-Editor:Zhang YL
 World Journal of Diabetes2024年4期
World Journal of Diabetes2024年4期
- World Journal of Diabetes的其它文章
- Nε-carboxymethyl-lysine and inflammatory cytokines,markers and mediators of coronary artery disease progression in diabetes
- Non-pharmacological interventions for diabetic peripheral neuropathy: Are we winning the battle?
- Application and management of continuous glucose monitoring in diabetic kidney disease
- Role of renin-angiotensin system/angiotensin converting enzyme-2 mechanism and enhanced COVlD-19 susceptibility in type 2 diabetes mellitus
- Are treatment options used for adult-onset type 2 diabetes mellitus (equally) available and effective for children and adolescents?
- Prevalence and risk factors of wound complications after transtibial amputation in patients with diabetic foot