
Clinical value of oral contrast-enhanced ultrasonography in diagnosis of gastric tumors
2024-01-26 02:19:18ChuanYuWangXiaoJingFanFeiLiangWangYueYueGeZhaoCaiWeiWangXinPingZhouJunDuDeWeiDai
Chuan-Yu Wang,Xiao-Jing Fan,Fei-Liang Wang,Yue-Yue Ge,Zhao Cai,Wei Wang,Xin-Ping Zhou,Jun Du,De-Wei Dai
Abstract BACKGROUND The incidence of gastric cancer remains high,and it is the sixth most common cancer and the fourth leading cause of cancer deaths worldwide.Oral contrastenhanced ultrasonography is a simple,non-invasive,and painless method for the diagnosis of gastric tumors.AIM To explore the diagnostic value of oral contrast-enhanced ultrasonography for the detection of gastric tumors.METHODS The screening results based on oral contrast-enhanced ultrasonography and electronic gastroscopy were compared with those of the postoperative pathological examination.RESULTS Among 42 patients with gastric tumors enrolled in the study,the diagnostic accordance rate was 95.2% for oral contrast-enhanced ultrasonography (n=40) and 90.5% for electronic gastroscopy (n=38) compared with postoperative pathological examination.The Kappa value of consistency test with pathological findings was 0.812 for oral contrast-enhanced ultrasonography and 0.718 for electronic gastroscopy,and there was no significant difference between them (P=0.397).For the TNM staging of gastric tumors,the accuracy rate of oral contrastenhanced ultrasonography was 81.9% for the overall T staging and 50%,77.8%,100%,and 100% for T1,T2,T3,and T4 staging,respectively.The sensitivity and specificity were both 100% for stages T3 and T4.The diagnostic accuracy rate of oral contrast-enhanced ultrasonography was 93.8%,80%,100%,and 100% for stages N0,N1-N3,M0,and M1,respectively.CONCLUSION The accordance rate of qualitative diagnosis by oral contrast-enhanced ultrasonography is comparable to that of gastroscopy,and it could be used as the preferred method for the early screening of gastric tumors.
Key Words: Oral contrast-enhanced ultrasonography;Gastric tumor;Electronic gastroscopy;Controlled study;Pathological examination;Diagnosis
INTRODUCTION
Gastric tumors,especially gastric cancer,is one of the most common gastrointestinal tumors worldwide[1].The incidence of gastric cancer remains high,and it is the sixth most common cancer and the fourth leading cause of cancer deaths worldwide[2],posing a great disease burden.Despite the high incidence of gastric cancer,the diagnosis of gastric tumors mainly depends on gastroscopy,and there are no suitable methods for large-scale screening[3].As gastroscopy is invasive and may cause discomfort,it is refused by some patients[4].Moreover,the efficacy of gastroscopy is relatively unsatisfactory,and it cannot meet the requirements of early screening of gastric cancer[5].With the advancements of highresolution color Doppler sonography and techniques of ultrasonography,oral contrast-enhanced ultrasonography has addressed the challenges associated with gastroscopy[6-9].Between March 2020 and July 2022,a total of 42 gastric tumor patients undergoing oral contrast-enhanced ultrasonography and gastroscopy at Beijing Hospital were enrolled in this study.The diagnostic findings and postoperative pathological examination results were compared to evaluate the diagnostic value of oral contrast-enhanced ultrasonography for gastric tumors.
MATERIALS AND METHODS
Subjects
In this study,data of 42 patients (25 males and 17 females) diagnosed with gastric tumors during clinic visits or hospitalization at Beijing Hospital between March 2020 and July 2022 were retrospectively analyzed.The mean age of these patients was 53.1 ± 17.2 years (range,38 to 75 years).All the patients were admitted to the hospital for symptoms such as abdominal discomfort,weight loss,and abdominal dull pain.Patients incapable of food intake and those with gastrointestinal tract obstruction were excluded.The diagnosis in all the patients was performed using electronic gastroscopy and postoperative pathological findings were reported.
Methods
Diagnostic medical devices:Siemens Sequoia color Doppler ultrasound system was used in this study with frequencies of probe ranging from 3.5 to 5.0 MHz.The gastrointestinal contrast agent “Tianxia” was used,which has a sound velocity of 1545 m/s and pH of 6.24.Ultrasound can clearly reveal the structure of the stomach due to the difference in echogenicity between the agent and the surrounding tissue[10].After the gastric cavity is filled with the contrast agent,there will be homogeneously distributed interface of medium echo on the ultrasonogram,similar to the echoes of solid tissues,which eliminates the interferences of gas and mucus in the gastric cavity,and clearly displays the structural layers of the gastric wall.Therefore,this technique has the best acoustic imaging effects for the stomach without inducing enhancement effect in the gastric cavity or posterior to the gastric wall,reverberation effect,or attenuation.
Examination method:The patients were asked to avoid greasy food for 2 d before the examination and barium enema for 3 d before the examination,and have semi-liquid low-residue diet or light liquid diet the day before the examination.Thereafter,the patients were fasting after dinner the day before the examination to the morning of the day of the examination,and did not drink water for 12 h.The contrast agent was prepared in suspension according to the manufacturer’s instructions,thoroughly mixed and orally administered at a dose of 500 to 600 mL.The patients were placed in the supine position,and the solid organs in the abdominal cavity (including the liver,gallbladder,pancreas,spleen,and bilateral kidneys) were routinely scanned.Then the patients were placed in the sitting position,the contrast agent was orally taken again,and ultrasound scanning was simultaneously performed.The patients were mainly placed in the sitting,supine,and right lateral positions,and the ultrasound probe was used for continuous scanning at the body surface along the gastric anatomical positions at the vertical and transverse sections.The gastric fundus was scanned in the left lateral position,while the gastric cardia,fundus,body,and antrum were scanned in the right lateral position.After a mass was detected,the position,size,morphology,mobility,and thickness of the gastric wall were carefully evaluated.The relationship of the mass with surrounding tissues,as well as other abnormalities such as the presence of obstruction,was observed,and color Doppler ultrasound was used to explore the blood flow in the mass.The lymphocyte expansion in the abdominal cavity and retroperitoneal area,metastases in organs,and presence of seroperitoneum were also observed,and computer image workstation was used to record the images.
Criteria for evaluation:After the gastric cavity is filled,the normal gastric wall shows five layers of structures of “highlow-high-low-high” echoes,respectively,which represents the echo of interface between the mucosal surface and gastric cavity,muscularis mucosa,submucosal layer,muscularis propria,serosal layer,and organs outside the mucosal layer.Gastric wall thickness is an important parameter for ultrasound diagnosis of gastric cancer[11].In patients with gastric cancer,the manifestations mainly include thickening of low echo of the gastric wall,ulceration,mass formation,disturbance of the five layers,and interruption of the continuity[12].In contrast,gastric ulcers usually show localized hypoechoic wall thickening,uneven or depressed mucosal surface,and hyperechoic lines on the mucosal surface,along with air retention at the bottom[13].
TNM represents the depth of tumor invasion to gastric wall,lymph node metastases,and distal metastases (UICC,5thedition).Specifically,T1 indicates the tumor invading the mucus or submucosal layer;T2 indicates the tumor invading the muscular layer or subserosal layer;T3 indicates the tumor invading through the serosal layer but not invading the adjacent organs;and T4 indicates the tumor invading through the serosal layer into the adjacent organs.N0 indicates no lymph node metastasis;N1 indicates that the number of lymph nodes with metastases is 1 to 6;N2 indicates that the number of lymph nodes with metastases is 7 to 15;and N3 indicates that the number of lymph nodes with metastases is >16.M0 indicates no distal metastasis,and M1 indicates the presence of distal metastases[14].
Evaluation method:Postoperative pathological findings were used as the gold standard for diagnosing gastric tumors.The accuracy of qualitative and quantitative evaluation of gastric tumors by oral contrast-enhanced ultrasonography and gastroscopy were compared.The accuracy,sensitivity,specificity,positive predictive value (PPV),and negative predictive value (NPV) of oral contrast-enhanced ultrasonography for the TNM staging of gastric tumors were investigated,using postoperative pathological findings as the reference standard.
Statistical analysis
SPSS 25 software was used for statistical analyses.Measurement data,described as the mean and standard deviation,were compared by the pairedt-test.P<0.05 was considered statistically significant.The sensitivity of diagnosis refers to the percentage of patients with positive results of examination,and specificity of diagnosis refers to the percentage of patients with negative results of examination.Sign test was used for the statistical analysis of sensitivity,specificity,PPV,and NPV of the diagnostic indicators.PPV is calcuclated as the number of true positive cases of certain indicator/total number of positive cases of the indicator.NPV is calcuclated as the number of true negative cases of certain indicator/total number of negative cases of the indicator.
RESULTS
Characteristics of lesions at oral contrast-enhanced ultrasonography
In this study,the size of lesions detected by oral contrast-enhanced ultrasonography was 1.0 to 7.2 cm.The increase of gastric wall thickness was 0.7 to 2.6 cm.The normal gastric wall structures disappeared.Most of the plica mucosa disappeared or became rigid,and the gastric cavity decreased.The lesions invaded the surrounding tissues along the layers of the gastric wall and the full-thickness of the gastric wall in some cases.The blood flow signal was relatively high in large gastric tumors,and the circuitous blood vessels could be easily displayed.The blood flow signals in stromal tumors were low and disperse.
Oral contrast-enhanced ultrasonography vs electronic gastroscopy and postoperative pathological findings
Gastric cancer was diagnosed in 40 patients (Figure 1),stromal tumors in two (Figure 2),and leiomyosarcoma in two using oral contrast-enhanced ultrasonography.Compared with the postoperative pathological findings,the diagnosis accordance rate of oral contrast-enhanced ultrasonography for gastric cancer was 95.2% (40/42),and Kappa value was 0.812 (P<0.05).The accordance rate of electronic gastroscopy was 90.5% (38/42),and Kappa value was 0.718 (P<0.05).The lesions in four patients were below the mucosa on gastroscopy and could not be displayed.

Figure 1 Oral contrast-enhanced ultrasonography showed localized thickening of the gastric wall at the greater curvature that suggested a diagnosis of gastric cancer,which was proven by postoperative pathological examination.
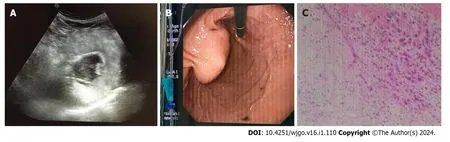
Figure 2 In a solid mass at the lesser curvature originating from the muscularis propria,oral contrast-enhanced ultrasonography indicated gastric stromal tumor,which was proven by postoperative pathological examination. A: Oral contrast-enhanced ultrasonography;B:Endoscopy image;C: Pathological examination.
Diagnostic efficiency of oral contrast-enhanced ultrasonography for gastric cancer stages in elderly patients
Compared with the postoperative pathological diagnostic results,the accordance rate of oral contrast-enhanced ultrasonography for TNM staging (accuracy rate) was 95.0% (38/40),95.0% (38/40),100.0% (40/40),and 100.0% (40/40) for T1,T2,T3,and T4 tumors,respectively.The sensitivity,specificity,PPV,and NPV were 100.0% (2/2),94.7% (36/38),50.0% (2/4),and 100.0% (36/36) for T1 stage,77.8% (7/9),100.0% (31/31),100.0% (7/7),and 93.9% (31/33) for T2 stage,100.0% (20/20),100.0% (20/20),100.0% (20/20),and 100.0% (20/20) for T3 stage,and 100.0% (9/9),100.0% (31/31),100.0% (9/9),and 100.0% (31/31) for T4 stage,respectively (Table 1).The accordance rate of oral contrast-enhanced ultrasonography for NM staging was 95.0% (38/40) for N0 stage,95.0% (38/40) for N1-N3 stages,100.0% (40/40) for M0 stage,and 100.0% (40/40) for M1 stage (Table 2).Totally,oral contrast-enhanced ultrasonography detected 8 Lymph nodes with metastases (N1) in two patients,41 Lymph nodes with metastases (N2) in four patients,and 37 Lymph nodes with metastases (N3) in two patients,most of which were at the gastric fundus or around the liver and great abdominal vessels.In addition,distal metastases (M1) were detected in the liver in four patients.

Table 1 Comparison of T staging results between oral contrast-enhanced ultrasonography and pathological findings

Table 2 Comparison of N staging results between oral contrast-enhanced ultrasonography and pathological findings
DISCUSSION
In recent years,the incidence and death rates of stomach cancer have remained high[2].The detection of gastric diseases is a major challenge for doctors.In China,more than 80% of gastric cancer patients are diagnosed at an advanced stage because they have no specific symptoms.Thus,the 5-year survival rate of gastric cancer is low[15].Screening for gastric cancer allows for early diagnosis and treatment,which will improve patient survival rates[16].Conventional gastroscopy is considered as the preferred method for diagnosing gastric tumors,which directly displays the lesions and can alsoperform biopsy under direct vision for pathological examinations[3].The sensitivity and specificity of gastroscopy are relatively high.However,gastroscopy involves major trauma and requires general anesthesia to achieve painlessness,which will cause certain risks[5].Therefore,many patients are unwilling to undergo gastroscopy,even though the disease has already progressed to middle or advanced stage at diagnosis,and thus they missed the best timing for the treatment of gastric tumors.Gastric cancer usually occurs in people over 50 years of age.However,gastroscopy is still poorly tolerated and adhered by the elderly due to objective and psychological factors such as age and physical condition[17].With the advancements in high-resolution color Doppler sonography and techniques of ultrasonography,oral contrastenhanced ultrasonography provides a new alternative for the detection of gastric tumors,which is easy to operate,safe,non-invasive,minimally invasive,and capable of displaying the size,morphology,internal structures,relationships with surrounding organs,and blood flow of gastric tumors from multiple aspects,angles,and layers.Previous studies have shown its value in gastric diseases[18-20].Especially,it can help asymptomatic patients to detect gastric cancer and improve the early diagnosis and treatment[21].For the tumor positioning in this study,the accordance rate was 95.2% (n=40) for oral contrast-enhanced ultrasonography and 90.5% (n=38) for electronic gastroscopy.However,oral contrastenhanced ultrasonography cannot allow biopsy of lesion tissues,and is influenced by gastric emptying and contrast agent.Therefore,the differentiation between benign and malignant gastric tumors <1 cm is relatively difficult in ultrasound examination.Although the diagnostic value of oral contrast-enhanced ultrasonography for gastric tumors has been established[22],the most commonly used method in clinical practice is electronic gastroscopy,indicating clinicians’ insufficient understanding of the advantages of oral contrast-enhanced ultrasonography for the diagnosis of gastric tumors.Previous studies also have shown that oral ultrasonography is more accurate than conventional ultrasonography in detecting the site,size,number,and extent of gastric lesions,and is almost comparable to upper gastrointestinal endoscopy in detecting small gastric lesions[23].
The normal gastric wall shows five layers of structures of “high-low-high-low-high” echoes on ultrasonogram,and the thickness of the gastric wall >5 mm is considered abnormal.A gastric tumor originates from the mucosal layer and gradually spreads to the submucosal layer,muscular layer,and serosal layer,and finally leads to abnormal thickening of the gastric wall or grows toward the intra-or extra-gastric cavity,which provides a good basis for the T staging of tumors by sonography[12].
For the evaluation of gastric wall invasion depth,the accuracy rate of oral contrast-enhanced ultrasonography was 95.0%,95.0%,100.0%,and 100.0% for stage T1,T2,T3,and T4 gastric tumors,respectively.The accuracy rate for stages T1 and T2 tumors was the lowest,which could be associated with the non-specific lesion characteristics,and the unclear boundary between the mucosal layer and muscular layer induced by uneven gastric wall thickening.Ultrasound contrast agent could provide good acoustic window but could not eliminate the near field artifacts.The greater curvature in coronal oblique view is in the near field,and thus the evaluation of gastric wall invasion depth is difficult.However,oral contrast-enhanced ultrasonography has high accuracy for diagnosing stages T3 and T4 gastric tumors,and could be used as a reference by doctors for identifying suitable operation methods.
Due to the insidious onset of gastric tumors,their symptoms are atypical.Some of the patients have peripheral lymph node metastases,celiac and pelvic lymph node metastases,and liver metastases at diagnosis.The detection of metastatic lesions could influence the selection of treatment strategy and outcomes of operation.Oral contrast-enhanced ultrasonography has specific manifestations for the diagnosis of gastric tumors,which could detect the damages of gastric wall structures early,evaluate the degree of invasion,and detect liver,celiac,and pelvic lymph node metastases more easily,and it has high diagnostic accordance rate with the qualitative diagnosis by postoperative pathological examinations[24].In this study,the accuracy of oral contrast-enhanced ultrasonography was 95.0% for preoperative diagnosis of stage N0 gastric tumor,95.0% for stages N1-N3 gastric tumor,and 100% for stages M0 and M1 gastric tumors.Gastroscopy could not evaluate the submucosal lesions,exophytic tumors,and metastases in organs in the abdominal cavity,while oral contrast-enhanced ultrasonography has unique advantages,which could effectively overcome the limitations of gastroscopy[25].Of the 42 patients with gastric tumors in this study,two had stromal tumors and two had gastric leiomyosarcoma that could not be visualized by gastroscopy,while oral contrast-enhanced ultrasonography could clearly display and diagnose these tumors.
CONCLUSION
In summary,oral contrast-enhanced ultrasonography has several advantages compared to gastroscopy.It is simple,safe,and minimally invasive for detecting gastric tumors,and is suitable for feeble and sick patients who cannot tolerate gastroscopy.For patients with anemia or abdominal dull pain,as well as thin patients,oral contrast-enhanced ultrasonography can be the preferred method for screening gastric tumors.In addition to the staging of middle or advanced stage gastric cancer,oral contrast-enhanced ultrasonography can also detect the metastases in peripheral and distal organs,which cannot be achieved by gastroscopy.Therefore,oral contrast-enhanced ultrasonography can avoid unnecessary exploratory surgical laparotomy,and provide reliable evidence for diagnosis and treatment of gastric tumors in clinical practice.The combined application of oral contrast-enhanced ultrasonography and electronic gastroscopy could improve the accuracy rate of the diagnosis of gastric tumors,provide more reliable evidence for the diagnosis,treatment,and outcome prediction of gastric tumors,and has guiding significance in clinical practice.
ARTICLE HIGHLIGHTS
Research background
The incidence of gastric cancer remains high,and it is the sixth most common cancer and the fourth leading cause of cancer deaths worldwide.Oral contrast-enhanced ultrasonography is a simple,non-invasive,and painless method for the diagnosis of gastric tumors.
Research motivation
The authors found that oral contrast-enhanced ultrasonography can avoid unnecessary exploratory surgical laparotomy,and provide reliable evidence for diagnosis and treatment of gastric tumors in clinical practice.
Research objectives
This study aimed to explore the diagnostic value of oral contrast-enhanced ultrasonography for the detection of gastric tumors.
Research methods
In this study,a total of 42 gastric tumor patients underwent both oral contrast-enhanced ultrasonography and gastroscopy.The screening results based on oral contrast-enhanced ultrasonography and electronic gastroscopy were compared with those of the postoperative pathological examination.
Research results
Among 42 patients with gastric tumors enrolled in the study,the diagnostic accordance rate was 95.2% for oral contrastenhanced ultrasonography,and 90.5% for electronic gastroscopy compared with postoperative pathological examination.The Kappa value of consistency test with pathological findings was 0.812 for oral contrast-enhanced ultrasonography and 0.718 for electronic gastroscopy,and there was no significant difference between them.
Research conclusions
In summary,oral contrast-enhanced ultrasonography has several advantages compared to gastroscopy.It is simple,safe,and minimally invasive for detecting gastric tumors,and is suitable for feeble and sick patients who cannot tolerate gastroscopy.The accordance rate of qualitative diagnosis by oral contrast-enhanced ultrasonography was comparable to that of gastroscopy,and it could be used as the preferred method for the early screening of gastric tumors.
Research perspectives
The combined application of oral contrast-enhanced ultrasonography and electronic gastroscopy could improve the accuracy rate of the diagnosis of gastric tumors,provide more reliable evidence for the diagnosis,treatment,and outcome prediction of gastric tumors,and has guiding significance in clinical practice.
FOOTNOTES
Author contributions:Wang CY and Dai DW designed the research study;Wang CY,Fan XJ,and Wang FL performed the research;Wang CY,Fan XJ,Wang FL,Ge YY,Cai Z,Wang W,Zhou XP,Du J,and Dai DW analyzed the data and wrote the manuscript;all authors have read and approved the final manuscript.
Institutional review board statement:The study was reviewed and approved by the Beijing Hospital Institutional Review Board.
Informed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:There is no conflict of interest to disclose.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Chuan-Yu Wang 0009-0007-8789-966X;De-Wei Dai 0009-0007-5528-0678.
S-Editor:Yan JP
L-Editor:Wang TQ
P-Editor:Zhao S
 World Journal of Gastrointestinal Oncology2024年1期
World Journal of Gastrointestinal Oncology2024年1期
- World Journal of Gastrointestinal Oncology的其它文章
- Early gastric cancer recurrence after endoscopic submucosal dissection: Not to be ignored!
- Present situation and prospect of immunotherapy for unresectable locally advanced esophageal cancer during peri-radiotherapy
- Comprehensive evaluation of rare case: From diagnosis to treatment of a sigmoid Schwannoma: A case report
- Emerging role of liquid biopsy in rat sarcoma virus mutated metastatic colorectal cancer: A case report
- Application of neoadjuvant chemoradiotherapy and neoadjuvant chemotherapy in curative surgery for esophageal cancer: A metaanalysis
- Comprehensive analysis of the role of ubiquitin-specific peptidases in colorectal cancer: A systematic review