
The influence of resistance exercise training prescription variables on skeletal muscle mass,strength,and physical function in healthy adults:An umbrella review
2024-01-25 09:36JonathanMcleodBradCurrierCarolineLowiszStuartPhillips
Jonathan C.Mcleod,Brad S.Currier,Caroline V.Lowisz,Stuart M.Phillips
Department of Kinesiology,Faculty of Science,McMaster University,Hamilton L8S4L8,Canada
Abstract Purpose: The aim of this umbrella review was to determine the impact of resistance training (RT) and individual RT prescription variables on muscle mass,strength,and physical function in healthy adults.Methods: Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,we systematically searched and screened eligible systematic reviews reporting the effects of differing RT prescription variables on muscle mass (or its proxies),strength,and/or physical function in healthy adults aged>18 years.Results:We identified 44 systematic reviews that met our inclusion criteria.The methodological quality of these reviews was assessed using A Measurement Tool to Assess Systematic Reviews;standardized effectiveness statements were generated.We found that RT was consistently a potent stimulus for increasing skeletal muscle mass (4/4 reviews provide some or sufficient evidence),strength (4/6 reviews provided some or sufficient evidence),and physical function (1/1 review provided some evidence).RT load (6/8 reviews provided some or sufficient evidence),weekly frequency(2/4 reviews provided some or sufficient evidence),volume(3/7 reviews provided some or sufficient evidence),and exercise order(1/1 review provided some evidence)impacted RT-induced increases in muscular strength.We discovered that 2/3 reviews provided some or sufficient evidence that RT volume and contraction velocity influenced skeletal muscle mass,while 4/7 reviews provided insufficient evidence in favor of RT load impacting skeletal muscle mass.There was insufficient evidence to conclude that time of day,periodization,inter-set rest,set configuration,set end point,contraction velocity/time under tension,or exercise order (only pertaining to hypertrophy) influenced skeletal muscle adaptations.A paucity of data limited insights into the impact of RT prescription variables on physical function.Conclusion: Overall,RT increased muscle mass,strength,and physical function compared to no exercise.RT intensity (load) and weekly frequency impacted RT-induced increases in muscular strength but not muscle hypertrophy.RT volume (number of sets) influenced muscular strength and hypertrophy.
Keywords: Hypertrophy;Resistance training;Resistance training prescription variables;Strength;Umbrella review
1.Introduction
Skeletal muscle is integral to many locomotive and metabolic processes critical for good health.Performing regular resistance training (RT)—muscle contraction against external resistance—improves muscular health;1in particular,RT increases skeletal muscle mass (i.e.,hypertrophy),strength,and physical function (gait speed,timed up-and-go,chair sit-to-stand,etc.).RT prescription (RTx) involves multiple programming variables,such as load,sets,frequency,rest intervals,muscle action type,and velocity.2Understanding how RTx variables impact muscular adaptations to RT is critical for effective exercise programming.
RTx has been a longstanding focus of exercise science;however,the contribution of many manipulatable RTx variables to muscular adaptations remains to be established.Systematic reviews have aimed to determine how individual RTx variables influence the development of strength and hypertrophy.These reports contributed to the development of advice by the World Health Organization for healthy adults to engage in moderate-tovigorous RT at least twice weekly.3Furthermore,the American College of Sports Medicine and National Strength and Conditioning Association have offered prescriptive position statements that advise adults to consider few (load and frequency3,4)or several RTx variables (load,frequency,sets,muscle action type/velocity,and rest intervals5,6).Systematic reviews provide high-quality evidence by collating and evaluating data with replicable search strategies and synthesis methods;7however,a synthesis of systematic reviews integrating multiple RTx variables is lacking.
Umbrella reviews extend upon systematic reviews by identifying,synthesizing,and evaluating evidence from multiple systematic reviews and meta-analyses on a common topic.We sought to summate the evidence from existing systematic reviews and meta-analyses investigating RTx variables and muscular adaptations to aid RT programming and guideline development for healthy adults.Thus,the purpose of the current umbrella review was two-fold: (a) to determine the influence of RT on skeletal muscle mass,strength,and physical function,compared with a non-exercise control group,and (b) to determine the impact individual RTx variables may have on RT-induced increases in muscle mass,muscle strength,and physical function.
2.Methods
2.1.Protocol and registration
This review was prospectively registered on the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY202 220028;https://inplasy.com/) and conducted under the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA).8
2.2.Information sources
A systematic search of Ovid MEDLINE,SPORTDiscus,and Web of Science was conducted from inception to December 9,2021.No publication status,language,nor study design limits were used when conducting each search,and references from relevant systematic reviews were screened manually.The complete search strategy for Ovid MEDLINE is provided in Supplementary Table 1.

Table 1 Population,intervention,comparator,outcomes,and study design(PICOS)criteria
2.3.Eligibility criteria
Eligibility was assessed by the predetermined Population,Intervention,Comparator,Outcomes,and Study Design(PICOS) criteria detailed in Table 1.Eligible reviews were published in English and investigated how muscle mass,strength,and/or physical function were impacted by RT,compared to a non-exercising control,and/or the manipulation of individual RTx variables in healthy adults.
2.4.Study selection and data extraction
Per PICOS criteria,2 reviewers (SMP and BSC) independently screened records at the title/abstract and full text stages,and any discrepancies were resolved by consensus with a third reviewer (JCM).Two reviewers (BSC and CVL) independently extracted information regarding the methods,results,and quality of all included articles,and any discrepancies were resolved by consensus with a third reviewer (JCM).Article screening and data extraction was completed using the Covidence systematic review software(Veritas Health Innovation,Melbourne,VIC,Australia;available at www.covidence.org).
2.5.Methodological quality assessment and evidence synthesis
The methodological quality of all included reviews was determined in duplicate using A Measurement Tool to Assess Systematic Reviews (AMSTAR),9as previously described,10,11to yield a score ranging from 1 to 11.Three authors (BSC,CVL,and JCM) systematically synthesized the evidence from each review to produce a standardized effectiveness statement(sufficient evidence,some evidence,insufficient evidence,insufficient evidence to determine;see Supplementary Table 2) for each outcome.10,11Two authors(BSC and JCM) then considered each standardized effectiveness statement to generate a bottom-line statement for the impact of each RTx variable on muscle mass,strength,and function.The quality of evidence (QoE) derived from each article was determined by a method based on the Grading of Recommendations Assessment,Development and Evaluation12approach for primary evidence (1=very low,2=low,3=moderate,or 4=high).This method incorporates the review design (meta-analysis: yes/no) and methodological quality (AMSTAR score) of included reviews10,11(Supplementary Table 3).RT and RTx variables were judged on the strength of evidence and number of participants with increased muscle mass,strength,and/or function.13

Table 2 Summary of included studies.
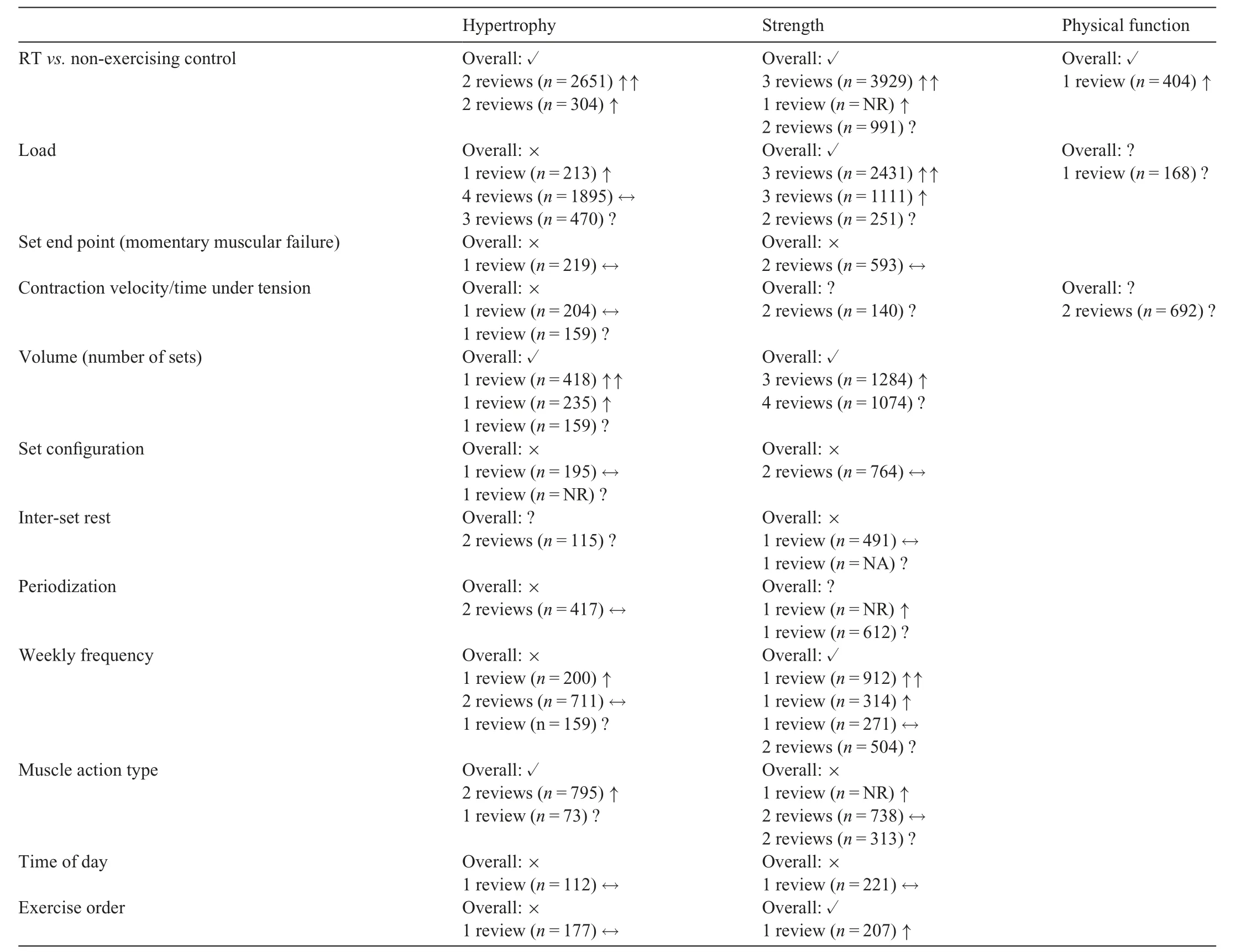
Table 3 Effects of resistance training and resistance training prescription variables on muscle hypertrophy,strength,and physical function.
3.Results
3.1.Included reviews
The literature search identified 837 records,and 362 were removed as duplicates.There were 407 records removed on title/abstract screening,2 records could not be retrieved,and 23 records were excluded on full-text screening.Fourtyfour14-57reviews (5 systematic reviews,2 meta-regressions,35 meta-analyses,1 network meta-analysis,and 1 umbrella review) met the eligibility criteria and were included (Fig.1).The AMSTAR scores and QoE for the included systematic reviews range from 2 to 10 and 1 to 4,respectively (Supplementary Fig.1,Table 2).The average RT duration within the included reviews ranged from 6 weeks to 24 weeks.For details of the 44 systematic reviews included in the umbrella review,see Supplementary Table 4.

Fig.1.PRISMA flowchart of reviews identified,screened,removed,and included in the review.PRISMA=Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
3.2.Muscle hypertrophy
3.2.1.RT vs.non-exercising control
Four reviews15,16,18,31ranging from low QoE (Level 2) to high QoE (Level 4) provided some16,18or sufficient15,31evidence that RT increases skeletal muscle mass compared to non-exercising controls (Table 3).In a high-quality metaanalysis (QoE: Level 4) comprising 15 original studies,Hagstrom and colleagues31found that RT resulted in a significant increase in skeletal muscle mass (standardized mean difference (SMD)=0.52;95% confidence interval (95%CI):0.20-0.78;p=0.002) compared with non-exercising controls in young women.Csapo and colleagues18conducted a metaanalysis including 5 original studies and found that,compared to non-exercising controls,gains in muscle size were small following higher-intensity RT (SMD=0.199;95%CI:0.046-0.343;p=0.011),and lower-intensity RT(SMD=0.108;95%CI:0.050 to 0.261;p=0.179)in healthy older adults.
3.2.2.Load
One low-quality review (QoE: Level 2),362 moderatequality reviews (QoE: Level 3),44,48and 1 high-quality review (QoE: Level 4)37provided evidence that RT load does not impact RT-induced skeletal muscle hypertrophy(Table 3).In a high-quality network meta-analysis (QoE:Level 4;24 studies andn=747 participants),Lopez and colleagues37compared 3 load prescriptions (high load,80%of 1-repetition maximum(1RM)or8 RM;moderate load,60%79% of 1RM or 9-15 RM;low load,<60% of 1RM or >15 RM) and found no significant difference in muscle hypertrophy between high-load RT and low-load RT(SMD=0.12;95%CI:0.06 to 0.29;p=0.241);moderateload RT and low-load RT (SMD=0.20;95%CI:0.04 to 0.44;p=0.113);high-load RT and moderate-load RT(SMD=0.09;95%CI:0.33 to 0.16;p=0.469).A moderate-quality meta-analysis(QoE:Level 3)conducted by Schoenfeld et al.48reported similar hypertrophic adaptations between high-load RT (>60% 1RM or <15 RM) and lowload RT (60% 1RM or15 RM;SMD=0.03;95%CI:0.08 to 0.14;p=0.56).Lacio et al.36highlighted that 14/16 randomized studies included in their review found no differences across low-load RT (<67% 1RM or >12RM),moderate-load RT(67%85%1RM or 6-12 RM),and highload RT (>85% 1RM or <6 RM) performed to volitional fatigue in muscle cross-sectional area or muscle thickness(QoE:Level 2)in young adults.
In contrast,a meta-analysis of moderate-quality (QoE:Level 3;7 studies andn=213 participants)18provided some evidence suggesting that high-load RT(80%1RM)provoked larger gains in muscle size than low-load RT (60% 1RM),although the difference in hypertrophy was trivial(SMD=0.136;95%CI: 0.009-0.259;p=0.036).Three reviews16,22,53provided insufficient evidence to form a conclusion on the effects of RT load on skeletal muscle hypertrophy due to a limited number of studies16,53and imprecise effect estimates.22
3.2.3.Set end point(momentary muscular failure)
One high-quality meta-analysis (QoE: Level 4;comprising 7 studies (n=219 participants)28concluded that performing RT to volitional fatigue had no impact on skeletal muscle hypertrophy (SMD=0.22;95%CI:0.11 to 0.55;p=0.152)(Table 3).
3.2.4.Contraction velocity/time under tension
A moderate-quality meta-analysis (QoE: Level 3)51found no significant differences(p=0.94)when training with repetition durations ranging from 0.5 s to 8.0 s (Table 3).One review16contained insufficient evidence to determine the effect of time under tension on muscle hypertrophy in older adults.
3.2.5.Volume(number of sets)
A moderate-quality meta-analysis (QoE: Level 3;15 studies) by Schoenfeld and colleagues50found that RT with a higher number of weekly sets promoted greater skeletal muscle mass gains than RT with a lower number of weekly sets (SMD=0.2410.100;95%CI: 0.026-0.457;p=0.03).Using meta-regression,the authors found there was a significant effect of the number of weekly sets on changes in skeletal muscle mass such that performing RT with 10+sets per muscle group per week (SMD=0.5200.130;95%CI:0.226-0.813;equivalent percent gain: 9.8%) elicited larger increases in skeletal muscle hypertrophy than performing RT with <5 sets per muscle group per week (SMD=0.3070.07;95%CI: 0.152-0.462;equivalent percent gain=5.4%).Krieger and colleagues35found that performing RT with multiple sets per exercise were associated with significantly larger increases in skeletal muscle than performing RT with a single set per exercise (SMD=0.110.40;95%CI:0.02-0.19;p=0.016),with no difference in performing 4-6 sets per exercisevs.2-3 sets per exercise (SMD=0.100.10;95%CI:0.09 to 0.30;p=0.29).One meta-regression16provided insufficient evidence to form a conclusion on the effect of RT volume on skeletal muscle hypertrophy in older adults(QoE:Level 3).
3.2.6.Set configuration
Davies and colleagues20found similar improvements in skeletal muscle hypertrophy between cluster-set RT and traditional-set RT (SMD=0.050.14;95%CI:0.32 to 0.23;p=0.73).Another meta-analysis32investigating cluster sets contained insufficient information to determine the impact of set configuration on skeletal muscle hypertrophy due to high heterogeneity (I2: 52%87%) and a small number of studies synthesized for analysis(<3 studies).
3.2.7.Inter-set rest
Two reviews,1 of moderate quality(QoE:Level 3)16and 1 of low quality (QoE: Level 2),24contained insufficient evidence to determine the impact of inter-set rest on muscle hypertrophy due to the limited number of studies synthesized for analysis(<6 studies)(Table 3).
3.2.8.Periodization
A high-quality meta-analysis (QoE: Level 4) by Grgic and colleagues26found no significant differences between linear periodization and undulating periodization on measures of hypertrophy (SMD=0.02;95%CI:0.25 to 0.21;p=0.848).Similarly,a low-quality systematic review (QoE:Level 2)25concluded that periodized and non-periodized RT programs may yield similar hypertrophic adaptations(Table 3).
3.2.9.Weekly frequency
Two moderate-quality reviews(QoE:Level 3)33,47provided evidence that weekly RT frequency does not impact skeletal muscle hypertrophy (Table 3).In a meta-analysis comprising 13 primary studies,Schoenfeld and colleagues47found that when RT volume was matched,there was no difference between higher-and lower-RT frequency (SMD=0.070.06;95%CI:0.08 to 0.21;p=0.32).Similarly,in healthy older adults,Kneffel et al.33found there to be no significant difference of RT frequency for muscle hypertrophy(p=0.51),with an estimate of 0.02(95%CI:0.04 to 0.07)for each day increase in frequency (QoE: Level 2).In contrast,Schoenfeld et al.49conducted a moderate-quality meta-analysis (QoE:Level 3) and found that higher-frequency RT was associated with a greater effect size than lower-frequency RT(SMD=0.190.03;95%CI: 0.11-0.20;p=0.003) (QoE:Level 3).One meta-regression16provided insufficient evidence to form a conclusion on the effect of RT frequency on skeletal muscle hypertrophy in older adults.
3.2.10.Muscle action type
Two reviews provided some evidence21,52that muscle action type might influence skeletal muscle hypertrophy(Table 3).In a moderate-quality meta-analysis(QoE:Level 3;15 studies),Schoenfeld and colleagues52reported that,compared with concentric RT,eccentric RT modestly increased skeletal muscle hypertrophy (SMD=0.25;95%CI:0.03 to 0.52;p=0.076).One very low-quality systematic review (QoE: Level 1) concluded that “Eccentric training appears to elicit greater increases in muscle CSA (crosssectional area)than concentric or traditional RT....Selective increases in fast-twitch fiber size have been reported and there is evidence to suggest that a shift towards a fast phenotype can occur as a result of chronic eccentric training”.21One moderate-quality meta-analysis (3 studies andn=73 participants)46provided insufficient evidence to determine the effect of muscle action type on skeletal muscle hypertrophy.
3.2.11.Time of day
One high-quality meta-analysis (QoE: Level 4;6 primary studies(n=112 participants))23found no significant difference between morning-RT and evening-RT (SMD=0.20,95%CI:0.40 to 0.40;p=0.958).
3.2.12.Exercise order
One high-quality meta-analysis (QoE: Level 4;7 primary studies;n=177 participants)39found no significant influence of exercise order on skeletal muscle hypertrophy (SMD=0.02;95%CI:0.45 to 0.41;p=0.937;I2=0%).
3.3.Strength
3.3.1.RT vs.non-exercising control
One low-quality review (QoE: Level 2),152 moderatequality reviews(QoE:Level 3),18,30and 1 high-quality review(QoE: Level 4)31provided sufficient evidence15,30,31or some evidence18that RT increases skeletal muscle strength compared to non-exercising controls(Table 3).
In a high-quality meta-analysis (QoE: Level 4),Hagstrom and colleagues31found that compared to non-exercising controls,RT resulted in significant increases in upper body strength (SMD=1.70;95%CI: 1.28-2.13;p<0.001) and lower body strength (SMD=1.40;95%CI: 1.03-1.76;p<0.001) in young women.Similarly,2 other moderate-quality meta-analyses (QoE: Level 3)18,30demonstrated similar benefits in muscular strength with RT,compared to nonexercising control groups,in healthy older adults.A lowquality umbrella review (QoE: Level 2;7 reviews andn=2869 participants) concluded there is a high QoE in support of RT for increasing muscle strength in older adults.15Csapo and colleagues18provided some evidence that high-load RT (SMD=0.778: 95%CI: 0.447-0.921;p<0.001) or low-load RT (SMD=0.663;95%CI: 0.396-0.826:p<0.001) provoked greater increases in muscle strength,compared with non-exercising controls,in healthy older adults.Two moderate-quality reviews (QoE: Level 3)16,54provided insufficient evidence due to high heterogeneity(I2>80%).
3.3.2.Load
One high-quality review (QoE: Level 4),374 moderatequality reviews,18,44,53,55and 1 low-quality review (QoE:Level 2)36provided some18,36,55or sufficient37,44,53evidence that RT load impacts RT-induced muscular strength gains(Table 3).In a high-quality network meta-analysis (QoE:Level 4),Lopez and colleagues37found that compared with low-load RT (<60% of 1RM or >15 RM),high-load RT(80% 1RM or8 RM;SMD=0.60;95%CI: 0.38-0.82)and moderate-load RT (60%79% 1RM or 9-15 RM;SMD=0.34;95%CI: 0.05-0.62) resulted in larger muscular strength improvements(p<0.001 and<0.003,respectively).Refalo and colleagues44found that higher-load RT is superior to lower-load RT for increasing 1RM (QoE: Level 3;36 studies,1187 participants;SMD=0.34;95%CI: 0.15-0.52;p=0.0003;favors high-load)and isometric maximal voluntary contraction (MVC;14 studies,302 participants;SMD=0.41;95%CI: 0.07-0.76;p=0.02) but not isokinetic MVC (10 studies,264 participants;SMD=0.19;95%CI:0.10 to 0.49;p=0.20).In a systematic review,Lacio and colleagues36demonstrated that most studies (11/18 studies for 1RM strength;6/9 studies for isometric MVC) concluded that moderate-and high-load RT were superior to low-load RT for increasing 1RM strength and isometric MVC (QoE: Level 2)in young adults.Meta-analyses by Steib and colleagues55and Csapo and colleagues18provided some evidence that RT with heavier loads may be required to maximize RT-induced skeletal muscle strength gains in older adults.Two reviews16,53provided inconclusive evidence regarding the impact of RT load on muscle strength due to a small number of studies being synthesized for analysis53or high heterogeneity (I2>80%).16
3.3.3.Set end point(momentary muscular failure)
In a meta-analysis of 15 reviews,Grgic and colleagues28showed no significant difference between failure RT or nonfailure RT on skeletal muscle strength(SMD=0.09;95%CI:0.22 to 0.05;p=0.198).Similarly,a high-quality meta-analysis(QoE: Level 4;8 studies)19found similar increases in muscle strength between failure RT (effect size=0.33;95%CI:0.06-0.61) and non-failure RT (effect size=0.34;95%CI:0.06-0.62)(Table 3).
3.3.4.Contraction velocity/time under tension
Two moderate-quality reviews(QoE:Level 3)16,55provided insufficient evidence to determine an effect in older adults due to highly heterogenous effects(I2>80%;Table 3).
3.3.5.Volume(number of sets)
A moderate-quality meta-analysis(QoE:Level 3;14 studies andn=440 participants)34found that performing multiple sets/exercise was associated with significantly greater strength gains compared with performing a single set/exercise(SMD=0.260.05;95%CI: 0.15-0.37;p=0.0001).The same review34found that performing 2-3 sets/exercise was associated with a significantly greater effect size than performing 1 set/exercise (SMD=0.250.06;95%CI:0.14-0.37;p=0.0001),but performing 4-6 sets/exercise was not superior to performing 1 set/exercise(SMD=0.35-0.25;95%CI:0.05 to 0.74;p=0.17)or 2-3 sets/exercise (0.09-0.20;95%CI:0.31 to 0.50;p=0.64).In a moderate-quality meta-analysis (QoE: Level 3;16 studies andn=621 participants),Wolfe and colleagues57found that multiple sets were superior to single sets for trained individuals(p<0.001)and RT programs with an extended duration(p<0.05).
Four additional reviews,ranging from low quality (QoE:Level 2)14to moderate quality(QoE:Level 3)16,43,55provided insufficient evidence to determine an effect due to systematic reviews containing high heterogeneity (I2>80%),16,43a low number of studies synthesized for review,55and 1 review14reporting inconclusive results with no effect present in 3 of the 6 studies included(Table 3).
3.3.6.Set configuration
In a high-quality meta-analysis(QoE:Level 4),Davies and colleagues20showed no difference in muscular strength gains between cluster-set RT and traditional-set RT (SMD=0.05-0.08;95%CI:0.21 to 0.11;p=0.56).Similarly,Jukic and colleagues32found that neither cluster(SMD=0.07;95%CI:0.21 to 0.07;p=0.300;I2=0%) nor rest redistribution(SMD=0.04;95%CI:0.20 to 0.12;p=0.641;I2=51%)set structures were more effective than traditional set structures in promoting muscular strength adaptations.
3.3.7.Inter-set rest
One low-quality systematic review (QoE: Level 2;23 studies;n=491 participants)29concluded that rest interval duration does not impact skeletal muscle strength.Another review16provided insufficient evidence to determine an effect in older adults due to considerably large heterogeneity(I2>80%;Table 3).
3.3.8.Periodization
In a low-quality meta-analysis (QoE: Level 2),Rhea and colleagues45found that periodized RT programs improved muscle strength over non-periodized RT programs.A moderate-quality review (QoE: Level 3)56provided insufficient evidence to determine an effect due to highly heterogenous effects(Q=213.56;p<0.001;I2=62.5%;Table 3).
3.3.9.Weekly frequency
In a moderate-quality meta-analysis (QoE: Level 3;22 studies;n=912 participants),Grgic et al.27found a significant(p=0.003) effect of weekly training frequency on muscular strength gains.Specifically,the authors concluded that higher RT frequencies (e.g.,4 days/week) resulted in larger strength gains than lower RT frequencies(e.g.,1 day/week).Similarly,a low-quality meta-regression (QoE: Level 2;9 studies andn=314 participants)33found a significant impact of weekly training frequency,such that for every daily increase in training frequency there was an 0.14 increase in effect size for muscular strength(Table 3).
In contrast,a high-quality meta-analysis(QoE:Level 4;12 studies;n=299 participants)done by Ralston and colleagues42concluded there was no significant impact of weekly frequency on muscular strength,regardless of whether RT volume was equated or not.Two moderate-quality reviews(QoE:Level 3)provided insufficient evidence to determine the impact of RT frequency on muscular strength gains in older adults.16,55
3.3.10.Muscle action type
In a very low-quality systematic review (QoE: Level 1),Douglas and colleagues21concluded that “Eccentric training may improve overall strength to a greater extent than concentric and traditional modalities,although there is a mode-specificity(i.e.,muscle action type and velocity)of improvements”.In contrast,a moderate-quality meta-analysis(QoE:Level 3)46found no differences between eccentric-or concentric-RT for improvement in peak torque (weighted mean difference: 3.71 N¢m;95%CI:0.27 to 7.70;p=0.07;n=333) or 1RM(weighted mean difference: 1.07 kg;95%CI:0.22 to 2.37;p=0.10;n=72).Two moderate-quality reviews(QoE:Level 3)17,38provided insufficient evidence to determine an effect due to the low number of studies synthesized for the analysis (<5 studies)(Table 3).
3.3.11.Time of day
One high-quality meta-analysis (QoE: Level 4;11 primary studies;n=221 participants)23found no significant differences between morning-RT and evening-RT,regardless of whether strength was assessed in the morning (SMD=0.08;95%CI:0.40 to 0.25;I2=1%;p=0.643) or in the evening(SMD=0.19,95%CI:0.11 to0.50;I2=0%;p=0.220)(Table 3).
3.3.12.Exercise order
One high-quality meta-analysis (QoE: Level 4;8 primary studies;n=207 participants)39found no significant influence of exercise order on dynamic strength(SMD=0.02;95%CI:0.45 to 0.41;p=0.937;I2=0%)when all performed strength tests were considered (i.e.,multi-joint (MJ) and single-joint(SJ)).However,exercise order did influence MJ dynamic strength (SMD=0.32;95%CI: 0.02-0.62;p=0.034;I2=0%;favors performing MJ exercises first)and SJ dynamic strength(SMD=0.58;95%CI:1.11 to0.05;p=0.032;I2=0%;favors performing SJ exercises first).
3.4.Physical function
Evidence was available for the influence of RT compared to no exercise and for the impact of RTx variables “load” and“contraction velocity/time under tension”.No evidence was available for the influence of other RTx variables on physical function.
3.4.1.RT vs.non-exercising control
A low-quality systematic review (QoE: Level 2;3 studies andn=404 participants)15concluded that there is high-quality evidence to support the role of RT in improving physical function in older adults compared to non-exercising controls(Table 3).
3.4.2.Load
One moderate-quality meta-analysis (QoE: Level 3)55contained insufficient evidence to determine an effect due to the low number of studies synthesized for analysis(<2 studies).
3.4.3.Contraction velocity/time under tension
One moderate-quality review (QoE:Level 3)55and 1 highquality review(QoE:Level 4)40contained insufficient evidence to determine an effect in older adults due to the limited number of studies synthesized for analysis(<3 studies)55or due to high heterogeneity and small-study publication bias.40
4.Discussion
This umbrella review incorporated evidence from 44 systematic reviews and meta-analyses to determine the impact of RT and individual RTx variables on skeletal muscle mass,strength,and physical function in healthy adults.RT was consistently found to be a potent stimulus for increasing skeletal muscle mass,strength,and physical function compared to non-exercising controls.RT load,weekly frequency,volume(number of sets),and muscle action type were the most studied RTx variables.Load,weekly frequency,and exercise order impacted RT-induced increases in muscular strength but not muscle hypertrophy.RT volume (number of sets) influenced muscular strength and hypertrophy.Muscle action type also impacted skeletal muscle hypertrophy (eccentric favored).In contrast,several other RTx variables—including inter-set rest,periodization,set end point,contraction velocity/time under tension,and set configuration—did not appear to affect muscle hypertrophy and strength gains.In many cases,a paucity of data limited our ability to shed insight into the impact of several RTx variables on physical function.
RT load was the most investigated RTx variable (17/44 systematic reviews) across all outcomes.Traditionally,training with higher loads has been a key strategy to optimize neuromuscular adaptations.Six out of 8 systematic reviews contained some18,36,55or sufficient37,44,48evidence supporting the notion that higher-load RT is pertinent for maximizing muscular strength gains.The superiority of higher-load RT for muscular strength gains can be attributed to the principle of specificity (i.e.,participants in higher-load groups regularly train using loads that are closer to the test of maximal (1RM)strength)48and neural adaptations that come with exercising at higher relative loads.58In contrast to muscular strength gains,muscle hypertrophy occurred independent of RT load(Table 3).Only 1 review examined the impact of RT load on physical function,and the low number of studies synthesized(<3 studies)prevented critical appraisal.However,the authors reported no differences between higher-and lower-load RT for improving stair climbing,timed up-and-go,chair rise,and walking speed in healthy older adults.55Further work is needed to clarify the impact—or lack thereof—of RT load on physical function.While the reviews included in our umbrella review provided important insight into the effects of RT load on skeletal muscle adaptations,RT load is primarily classified in binary terms (e.g.,heavy loadvs.light load),yet during an RT program,individuals may employ a spectrum of RT loading zones.It has been hypothesized that the amalgamation of a variety of RT loading zones may have synergistic effects on skeletal muscle adaptions;59however,future studies are needed to draw stronger inferences.
RT volume is the total amount of work performed in a resistance exercise session(or sometimes summed per week),and it is often defined by the number of sets performed.Our results herein suggest that RT volume impacts skeletal muscular strength and hypertrophic gains (Table 3).It has been suggested that the doseesponse relationship between RT volume and skeletal muscle hypertrophy follows an inverted-U shape.59Krieger34showed that performing 2-3 sets/exercise and 46 sets/exercise was superior to performing 1 set/exercise,but there was no difference in hypertrophy adaptations when comparing 2-3 sets/exercise and 4-6 sets/exercise.The results from Krieger34suggest that higher volume RT confers an increasingly additive hypertrophic advantage but then plateaus,after which there are diminishing returns (less gain per volume increase) for hypertrophy and possibly detrimental outcomes.59A recent umbrella review by Bernrdez-Vzquez et al.60also observed a doseesponse relationship between RT volume and hypertrophy and suggested that at least 10 sets per muscle group is optimal to increase muscle mass.Without considering blood flow restriction (excluded herein),our review strengthens this observation by including 32 (as opposed to 1260) systematic reviews on RTx variables and hypertrophy.Bernrdez-Vzquez et al.60included 1 review not captured by our search strategy that showed exercise order might influence strength (favoring exercises performed at the beginning of a training session) but not hypertrophy.60Overall,our finding that RT volume is critical for hypertrophy supports and expands upon the findings from Bernrdez-Vzquez et al.60
RT frequency was found to have a negligible impact on muscle hypertrophy but a potential influence on muscle strength.The discrepancy between muscle mass and strength outcomes might be attributed to including systematic reviews regardless of whether volume-equated studies were included.For instance,a meta-analysis of 22 studies27found a doseesponse relationship between RT frequency and muscular strength gains;however,a subgroup analysis of volumeequated studies suggested that RT frequency negligibly impacted muscular strength gains.Furthermore,Schoenfeld et al.49demonstrated that when RT volume wasnotequated across protocols,higher training frequencies (e.g.,3 days per week)were consistently superior to lower training frequencies(e.g.,1 day per week).The same group conducted another meta-analysis47on only volume-equated studies and found no effect of RT frequency on muscular hypertrophy.The effect of weekly training frequency is difficult to discern because training frequency is related to RT volume.Therefore,we propose that weekly training frequency does not independently influence skeletal muscle adaptations,but that increasing training frequency can be manipulated to permit higher total weekly volume (with equal,or even reduced,within-session volume) and subsequent muscle mass and strength accrual.We also propose that,as with RT volume,at some point frequency becomes redundant and increases in strength and hypertrophy plateau.However,future studies are needed to determine whether splitting weekly RT volume across additional weekly training sessions can maximize skeletal muscle adaptations.
Muscle action type(eccentric RTvs.concentric RT)was an impactful RT variable for muscle hypertrophy (Table 3).However,a limitation of the current umbrella review is that we did not consider limiting our inclusion to reviews that matched muscle action type for total work or maximum load,an oversight that could lead to divergent effects.Greater forces can be generated with eccentric contractions than concentric contractions,so utilizing eccentric loads (greater than concentric 1RM) could yield different workloads and subsequent adaptations;21on the other hand,adaptations are similar when the 2 muscle action types are matched for total work or maximum load.61Performing isolated,supramaximal,eccentric contractions is pragmatically complex and may require special equipment(e.g.,isokinetic dynamometers,iso-inertial devices)or external assistance(e.g.,a spotter).52,62However,flywheel training has emerged as a RT modality that is particularly effective for implementing high eccentric loads,which are difficult to achieve with traditional RT equipment.63Nonetheless,combining eccentric and concentric contractions(i.e.,conventional RT)is more practical for practitioners.
There was either no impact or insufficient evidence to determine the impact of contraction-velocity/time-under tension on muscle hypertrophy,strength,and physical function.Diverse ranges of repetition durations are practical for promoting skeletal muscle adaptations,though very slow repetition durations(~10 s) appear to be detrimental.Considering that preserving muscle power appears to be important for maintaining physical function and the activities of daily living,6,64older adults may benefit from high concentric-velocity RT(i.e.,power training).High-quality studies must be conducted to provide more evidence clarifying the role of contraction velocity on skeletal muscle adaptations.
Non-periodized RT programs with adequate volume and progressive overload are sufficient to elicit muscular adaptations.59However,per session (or weekly) volume does not have to remain consistent throughout a training program,and periodizing volume has been hypothesized as a viable strategy for maximizing the doseesponse relationship between volume and muscular adaptations.An RT program may be periodized using 1 or more conventional methods,such as linear periodization,daily undulating periodization,or block periodization.Overall,periodized and non-periodized RT programs elicit similar increases in hypertrophy.Furthermore,linear and undulating periodization approaches will yield similar skeletal muscle adaptations.26Early work from Rhea and colleagues45suggested that periodized RT is superior to non-periodized RT for strength development.The mechanisms behind augmented strength gains with periodized RT remain unclear,but periodization may aid with augmenting recovery and preventing overtraining.6,59It has been suggested that superior strength gains with periodized RT are not due to the systematic variation of training,but could be attributed to the principle of specificity;participants may be training with heavier loads in the last mesocycle (i.e.,near post-testing).65In the current study,none of the included reviews controlled for the principle of specificity,and future studies should attempt to control for this phenomenon to properly determine whether periodized RT is an important variable to consider for maximizing strength gains.
Set configuration methods (traditional set distribution,rest redistribution,cluster sets) and rest intervals represent advanced techniques to disperse training volume within a resistance exercise session.However,we found less evidence supporting these variables than volume for optimizing skeletal muscle adaptations.Therefore,periodized or non-periodized training approaches,including various set configurations and rest intervals,appear to induce similar adaptations,provided adequate volume is employed.
Performing resistance exercises to momentary muscular failure has been posited as important for increasing muscular strength and mass.In contrast to this hypothesis,the current umbrella review suggests that RT-induced increases in muscle mass can be achieved without going to a set end point of momentary muscular failure.Training to muscular failure does not appear to have detrimental effects on training-induced adaptationsper se,but studies on the chronic(i.e.,>3 months)impact of momentary failure training are lacking.Training to momentary muscular failure may also elicit discomfort,pose safety risks,and lead to neuromuscular fatigue,particularly for older adults.6Indeed,training to muscular fatigue is not required for older adults to observe training-induced neuromuscular adaptations.66,67Training to momentary muscular failure may become increasingly important for trained individuals,28,59but the findings here should be translated to athletic populations with caution and diligence to avoid excess fatigue and overtraining.
Human exercise performance68and strength69appear to peak in the evening(~18:00 h),and preclinical studies suggest the timing of exercise over the day can influence the beneficial effects of training.70However,the results presented herein demonstrate that morning or evening produces similar increases in muscle strength and mass (Table 3).Only 2 systematic reviews were identified on this topic;so,additional research is needed to determine whether there are differences between morning and evening training.Time of day for training does not appear to impact muscular adaptations and is best selected by personal preference.
We found that exercise order impacted RT-induced increases in muscular strength.Specifically,Nunes and colleagues39found that increases in dynamic strength were greater in exercises performed at the beginning of a resistance exercise session,which relates back to the principle of specificity.When exercises are performed at the beginning of a resistance exercise session,individuals are less fatigued and able to utilize higher relative loads and effort.To augment RT-induced increases in skeletal muscle hypertrophy,it has been hypothesized that individuals should prioritize performing MJ as opposed to SJ exercises at the beginning of a resistance exercise session as this allows for the accumulation of greater training volume.71In contrast,to augment sitespecific skeletal muscle hypertrophy(e.g.,triceps)others have suggested that it is better to perform SJ exercises(e.g.,triceps extension) prior to MJ exercises (e.g.,bench press).72The results of the current umbrella review suggest that RT-induced increases in skeletal muscle hypertrophy are similar regardless of exercise order.Therefore,exercise order impacted RTinduced increases in muscular strength but not muscle hypertrophy.Individuals wanting to improve their maximal strength for a given exercise should perform that exercise at the beginning of the resistance exercise session.39
The strengths of this umbrella review include the comprehensive search strategy utilized and the large number of systematic reviews included.Several limitations require acknowledgement and consideration when interpreting the results of this umbrella review.Potentially relevant reviews published since the last search (December 9,2021 to current)60,73-77were not captured by our search strategy,which prevented us from determining the impact of additional RT-variables,such as exercise selection,73,76exercise variation,74and range of motion.75,77Future work should be aimed at characterizing the influence of the aforementioned RTx variables on hypertrophy,strength,and physical function.We identified limited evidence from which we could draw conclusions on the impact of different RT variables on physical function,which may be attributed to including systematic reviews with only healthy older adults (e.g.,not frail).Additionally,well-trained elite athletes/military persons were excluded because these populations commonly perform RT in addition to their sport-specific training,which would make it difficult to discern the influence of RTx variables from alternative modalities of exercise training.The current study also excluded individuals with chronic disease.To provide additional insight,future work is required to determine the impact of different RTx variables on these populations.The average range for RT duration was 6-24 weeks,and any interpretations of the results for longer durations should be viewed with caution.About 1/3 of the systematic reviews in the current study contained either high levels of heterogeneity or included a limited number of studies;thus,we were unable to draw satisfactory conclusions from these reviews.We also acknowledge that additional RT program variables not investigated in the current review (e.g.,blood flow restriction) may influence outcomes.Nonetheless,based on observations from the current review,we propose that the impact of these other variables is likely limited in terms of effects on strength and hypertrophy.Directions for future research are apparent when we note the limited data for physical function and specific RTx variables(e.g.,time of day,set configurations,and inter-set rest intervals).Additionally,not presenting a list of included and excluded studies (40 reviews),not includinga prioridesign(38 reviews),and the use of publication status as an inclusion criterion (if the search included grey literature;33 reviews)were the most common factors detracting from the quality of included reviews.Researchers may wish to consider these points before embarking on future systematic reviews.
5.Conclusion
This umbrella review found that RT promotes increased muscle hypertrophy,strength,and physical function in healthy adults compared to no exercise.RT volume appears to be important for both muscular strength and hypertrophic gains.RT load and weekly frequency appeared to be important for muscle strength.Muscle action type seems to be important for hypertrophy but not strength.Inter-set rest,periodization,set end point,contraction velocity/time under tension,and set configuration were not important to RT-induced adaptations.Less is known regarding which RT variables are important for optimizing improvements in physical function.We conclude that RT largely increases muscle hypertrophy,strength,and physical function compared to no exercise,and that very few RTx variables impact muscular adaptations.
Acknowledgments
No funding was received for this review.BSC is supported by an Alexander Graham Bell Canada Graduate Scholarship-Doctoral.JCM is supported by an Ontario Graduate Scholarship.SMP is supported by the Canada Research Chairs programme.
Authors’contributions
JCM and BSC contributed equally to this paper,designed and executed the systematic search,with the assistance of CVL screened articles,extracted data,evaluated articles using standardized effectiveness statements and AMSTAR and,along with SMP,conceived the review and drafted the manuscript.All authors critically revised the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
SMP reports grants or research contracts from the U.S.National Dairy Council,Canadian Institutes for Health Research,Dairy Farmers of Canada,Roquette Freres,Ontario Centre of Innovation,Nestle Health Sciences,Myos,National Science and Engineering Research Council,and the U.S.NIH during the conduct of the study;personal fees from Nestle Health Sciences and non-financial support from Enhanced Recovery,outside the submitted work.SMP has patents licensed to Exerkine,but reports no financial gains from any patent or related work.All the support had no involvement in the study design and writing of the manuscript or the decision to submit it for publication.The remaining authors report no competing interests.
Supplementary materials
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2023.06.005.
 Journal of Sport and Health Science2024年1期
Journal of Sport and Health Science2024年1期
- Journal of Sport and Health Science的其它文章
- 2024 Adult Compendium of Physical Activities:A third update of the energy costs of human activities
- Older Adult Compendium of Physical Activities:Energy costs of human activities in adults aged 60 and older
- 2024 Wheelchair Compendium of Physical Activities:An update of activity codes and energy expenditure values
- Alexa,let’s train now!—A systematic review and classification approach to digital and home-based physical training interventions aiming to support healthy cognitive aging
- A systematic scoping review of study methodology for randomized controlled trials investigating probiotics in athletic and physically active populations
- Associations of daily sedentary behavior,physical activity,and sleep with irritable bowel syndrome:A prospective analysis of 362,193 participants