
Occurrence and Decay of SARS-CoV-2 in Community Sewage Drainage Systems
2024-01-22 10:32QinDongJunXiongCiYnChenLiuHiBoLingQiWngLuoJingXingShoLinYngZhengShengLuYiLiuXiHungJiuHuiQuc
Engineering 2023年7期
Qin Dong,Jun-Xiong Ci,Yn-Chen Liu*,Hi-Bo Ling,Qi Wng,Luo-Jing Xing,Sho-Lin YngZheng-Sheng Lu Yi Liu Xi Hung*, Jiu-Hui Quc
a State Key Joint Laboratory of Environment Simulation and Pollution Control, School of Environment, Tsinghua University, Beijing 100084, China
b Hubei Provincial Academy of Eco-Environmental Sciences, Wuhan 430072, China
c Key Laboratory of Drinking Water Science and Technology, Research Center for Eco-Environmental Sciences, Chinese Academy of Sciences, Beijing 100085, China
Keywords:SARS-CoV-2 Transmission risk Drainage system Sewage Community
ABSTRACT The rapid spread of the coronavirus disease(COVID-19)pandemic in over 200 countries poses a substantial threat to human health.Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes COVID-19, can be discharged with feces into the drainage system.However, a comprehensive understanding of the occurrence, presence, and potential transmission of SARS-CoV-2 in sewers, especially in community sewers, is still lacking.This study investigated the virus occurrence by viral nucleic acid testing in vent stacks, septic tanks, and the main sewer outlets of community where confirmed patients had lived during the early days of the epidemic in Wuhan, China.The results indicated that the risk of long-term emission of SARS-CoV-2 to the environment via vent stacks of buildings was low after confirmed patients were hospitalized.SARS-CoV-2 were mainly detected in the liquid phase, as opposed to being detected in aerosols, and its RNA in the sewage of septic tanks could be detected for only four days after confirmed patients were hospitalized.The surveillance of SARS-CoV-2 in sewage could be a sensitive indicator for the possible presence of asymptomatic patients in the community,though the viral concentration could be diluted more than ten times, depending on the sampling site,as indicated by the Escherichia coli test.The comprehensive investigation of the community sewage drainage system is helpful to understand the occurrence characteristics of SARS-CoV-2 in sewage after excretion with feces and the feasibility of sewage surveillance for COVID-19 pandemic monitoring.
1.Int roduction
The outbreak of coronavirus disease 2019(COVID-19)is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)[1,2].It has rapidly spread throughout 202 countries around the world.As of 5 October 2021, there have been 236 599 025 confirmed cases and 4 831 486 deaths globally,and the number is still increasing rapidly.There is evidence of human-to-human transmission of SARS-CoV-2[3–6].In addition to direct contact and respiratory routes [2,7], fecal transmission might be an alternative route, supported by the occurrence and survival of SARS-CoV-2 in patient feces [8–11].Infected patients can excrete the virus in feces for several days, even after their respiratory symptoms have resolved [12].Although several studies on the decay and persistence of SARS-CoV-2 or SARS-CoV-2 RNA in different matrices have been performed in the laboratory[13–15],the actual persistence in the sewage system of communities with sporadic confirmed cases has rarely been studied.Although the virus can be detected in human feces and urine, the persistence and spread of SARSCoV-2 in the drainage system is unknown.SARS-CoV-2 infection via bioaerosols poses a potential threat to human health.Therefore,it is necessary to study the decay, transmission, and potential infectivity of SARS-CoV-2 in drainage systems.
The sewage plumbing system of a building is a reservoir of pathogenic microorganisms such as SARS-CoV-2,and could potentially be a source that enables transmission of the airborne virus within a housing block.Incomplete disinfection and defects in plumbing systems in indoor environments such as hospitals and residential buildings may increase the chance of viral droplets infecting people.During the severe acute respiratory syndrome(SARS) outbreak in 2003, a super spreading event with a total of 342 confirmed cases within a building in Hong Kong, China raised concern [16].The vent stacks within the building were suspected as a possible route of transmission of water-related disease [17].During COVID-19,some studies proposed that the drainage system may be a plausible source of transmission that could lead to infection and global spread of SARS-CoV-2[18,19].Thus,we should take into consideration both the persistence of viruses and their infectivity in the environment.The detection and retention of SARSCoV-2 in plumbing systems is of great importance for studying its potential spread and infectivity in buildings.
The community drainage system is the beginning of the sewer system,and SARS-CoV-2 may persist in sewage for a relatively long time.There is a risk of contamination of the downstream drainage system if the viruses can survive in the septic tank within the community.Both the temperature and matrix type can influence the microbial decay and persistence of viruses in raw sewage.Ahmed et al.[15] observed that temperature greatly influenced the firstorder decay rate of SARS-CoV-2 RNA in wastewater, and SARSCoV-2 RNA persisted longer in tap water (9.40–58.60 days) than in raw wastewater (8.04–27.80 days) and autoclaved wastewater(5.71–43.20 days).However,a recent study reported that 90%inactivation of viable SARS-CoV-2 in untreated wastewater and tap water at room temperature occurred between 1.5 and 1.7 days[14].SARS-CoV-2 RNA is more persistent than viable SARS-CoV-2 and can remain in wastewater for a longer time [13,14].A risk of transmission still exists in community sewage systems after SARS-CoV-2 discharge from confirmed cases.However, experiments conducted in the laboratory may alter the microbiota that influence the decay of virus particles in wastewater.Thus, a comprehensive analysis of field tests would provide more information.
The sewer is a semi-enclosed system, and researchers have demonstrated that aerosols from sewage containing microorganisms that pose a high risk to human health, including pathogens,fungi, and viruses can escape the system [20–23].Pathogenic transmission may occur via the inhalation of small droplets originating from sewage pipes.These pathogenic microorganisms can infect the operators of sewerage and citizens residing near the drainage system through inhalation,direct contact,and oral intake.Therefore, it is necessary to investigate the occurrence and persistence of SARS-CoV-2 in septic tanks and the related drainage system of the communities with confirmed cases.
We conducted a comprehensive investigation of the occurrence,presence, and potential transmission of SARS-CoV-2 in a community sewage drainage system during the early days of the COVID-19 in Wuhan,China.The transmission risk of SARS-CoV-2 via sanitary plumbing systems was evaluated in select communities after the hospitalization of a confirmed COVID-1 patient.Field tests were conducted to detect the occurrence of SARS-CoV-2 in vent stacks,septic tanks,and manholes within the community drainage system via the SARS-CoV-2 RNA test.This study provides valuable field data to enhance our understanding of the occurrence characteristics of SARS-CoV-2 in sewage after excretion in feces and the feasibility of sewage surveillance for COVID-19 pandemic monitoring.
2.Materials and methods
2.1.Sampling
Sewage plumbing systems in communities with confirmed patients in Wuhan were selected as a case study.In this study, a total of five communities (FG, WD, CF, FD, and DZ) were selected,with 1–3 confirmed patients that were registered and hospitalized.The aerosol, sewage, and sediment samples were collected from septic tanks of buildings, as well as aerosol samples from vent stacks of the buildings of residence of the confirmed cases.Additionally, the sewage, sediment, and aerosol samples in the main drainage outlet of the communities were all tested.The sampling times of all sewage, sediment, and aerosol samples were between 4 and 52 days after the patients were hospitalized.
The aerosol samples were collected by using an aerosol particle liquid concentrator (WA-15; Beijing Dinglan Technology Co., Ltd.,China) at a flow rate of 14.0 L∙min-1for 30 min.This sampler can concentrate the aerosol particles directly into the liquid.Sewage samples were collected from septic tanks of buildings where confirmed patients had lived on February 26, March 1, and March 10, 2020.A stratified plexiglass sampler was used to obtain samples from different layers of the septic tank, designated the top layer (0–50 cm)and bottom layer (50–100 cm).All collected samples were immediately transferred to the laboratory at 4°C for RNA extraction.
2.2.Bacteriological analysis
The bacteriological examination of Escherichia coli(E.coli)(fecal indicator) was conducted using the plate counting method.The collected sewage was concentrated, and the supernatant was removed.Then, the sample was prepared in physiological saline and serially diluted ten-fold.One milliliter of each prepared diluted sample was transferred aseptically into a series of nine test tubes that contained Durham tubes and double strength MacConkey broth (Merck, Germany).The tubes were shaken gently and incubated at 37°C for 24–48 h until gas production and lactose fermentation indicated positive reactions.Finally, the concentration of E.coli was estimated using the most probable number (MPN)method and reported as CFU∙mL-1.
2.3.RNA extraction and RT-PCR analysis
First,500 mL of sewage samples and 2–3 mL of aerosol samples were centrifuged at 3000 g for 0.5 h,and the suspension was transferred to a sterilized bottle.Then, NaCl and polyethylene glycol(PEG)-6000 were added,and the final concentrations were adjusted to 0.3 mol∙L–1and 10%,respectively[24].The prepared suspension was allowed to settle overnight and centrifuged at 10 000g for 0.5 h.The residue after centrifugation was collected for further RNA extraction.The samples from septic tanks were centrifuged at 10 000g for 0.5 h.Then, the residue was also collected for RNA extraction.Total RNA was extracted using the EZ1 virus Mini kit(Qiagen,Germany)according to the manufacturer’s instructions.
Two target genes, which encoding nucleocapsid protein(CCDCN) and open reading frame lab (CCDC-ORF1), were simultaneously detected using reverse transcription-rolymerase chain reaction(RT-PCR), following the procedures described in the Project of COVID-19 Prevention and Control (fifth edition, Chinese Center of Disease Control and Prevention)[25].The sequences of the two primer pairs and probes are listed in Table 1.All RT-PCR amplifications were performed in a 25 μL reaction system using an AgPath-IDTMOne-Step RT-PCR Kit (Life Technologies, USA).All RTPCR mixtures contained 12.5 μL of 2× RT-PCR buffer, 1 μL of forward and reverse PCR primers, 1 μL of TaqMan probes, 1 μL of 25× RT-PCR enzyme mix, 4 μL of nuclease-free water, and 4.5 μL of RNA template.The PCR amplification procedures are shown in Table 1.
RT-PCR amplification was performed on a LightCycler 480 realtime PCR platform (Roche, USA) in triplicate.For each amplification, triplicate negative and positive controls were conducted to verify the results.Cycle threshold (Ct) values of ≤37, ≥40, and 37–40 were used to classify samples as positive, negative, and suspected samples, respectively.

Table 1 Primers and probes used in this study.
3.Results
3.1.Cross-transmission of SARS-CoV-2 by building sanitary plumbing systems
Since the spread of SARS-CoV-2 through aerosols has been confirmed,the fecal–oral route is emerging as a considerable environmental concern for community transmission.To evaluate the risk of transmission via aerosols within buildings where confirmed cases reside, five typical communities with confirmed patients were selected to detect SARS-CoV-2 nucleic acid in aerosols from the vent stack of the drainage system.Specifically, the detection of SARS-CoV-2 in the vent stack of the buildings was performed on days 4,30,32,42,and 52 after hospitalization of the confirmed patients.The detection results of all samples using primers for CCDC-ORF1 and CCDC-N both showed good consistency.No positive detection of SARS-CoV-2 nucleic acid was detected in the aerosol samples collected from vent stacks for four days after the confirmed patient left the residence(Table 2).The results did not indicate the persistence or flushing out of viral nucleic acid in the vent stacks for more than four days.Additional samples were collected from the vent stacks on days 4, 19, and 31 after the confirmed patients had recovered and returned to their residences from the hospital,and the results of nucleic acid tests from all of those samples were negative.
3.2.The fate of SARS-CoV-2 in septic tanks of the community drainage system
The presence of SARS-CoV-2 in the septic tanks of the buildings of residence of confirmed patients was investigated.The sewage,sediment, and aerosol samples were all obtained from the septic tanks 4–52 days after the confirmed patient was hospitalized.The results of RT-PCR testing are shown in Table 3.The samples from aerosols and sediments in septic tanks were all determined to be negative.On the 4th day after the patient was diagnosed with COVID-19 and hospitalized,one sewage sample collected from the FG community septic tank on March 20 tested positive for SARSCoV-2 with a Ct value of 34.41 ± 0.45 using the CCDC-ORF1 assay,while the CCDC-N assay failed to detect SARS-CoV-2 in this sample.This demonstrates that SARS-CoV-2 RNA was detected in the sewage of the septic tanks after the confirmed patient was absent from the building for four days.After the confirmed patient was hospitalized for 23 days, virological testing of various types of samples in the septic tanks was negative.Unfortunately, due to epidemic development and limited field conditions, no valid samples were available between the 4th and 23rd day.
3.3.SARS-CoV-2 surveillance at the outlet of the community drainage system
As shown in Table 4, although the SARS-CoV-2 RNA test was positive in the sewage from the building on the 4th day after the patient was hospitalized, no positive detection of nucleic acid was found at the outlet of the community drainage system.Moreover,the results of the nucleic acid tests of both the sediment and aerosol were classified as negative or not detected.Thereafter, at WD,no positive samples were detected in the septic tanks of their residential buildings after all the confirmed cases were hospitalized for 23 days.However, the nucleic acid tests were positive for samples from the outlet of the community range system on the 23rd day after the confirmed patients were hospitalized for both CCDC-ORF1 and CCDC-N primers and on the 30th day for the CCDC-ORF1 primer.At CF, SARS-CoV-2 RNA was detected (37.89 ±0.53) for the CCDC-N primer at the outlet of the community drainage system on the 31st day after the patients were hospitalized, while samples from septic tanks were negative in the same timeframe.Positive detection at the community outlet without confirmed SARS-CoV-2 emission source indicate that asymptomatic infection or other viral source might be present in the community.Unfortunately, due to inadequate awareness during the early period of the epidemic no valid information regarding confirmed asymptomatic infection during the study is available.
3.4.Estimation of the apoptosis of SARS-CoV-2 surrogate in community drainage system
E.coli,which has been used as an indicator of fecal transmission in sewage and the extent of fecal contamination in the environment,was selected to indirectly represent the dilution or apoptosis of SARS-CoV-2 during sewage transportation [26,27].The concentrations of E.coli in septic tanks near the building and the drainage outlets of the residences in CF,FD,FG,and DZ are shown in Table 5.The concentration of E.coli in sewage decreased by an order of magnitude from the septic tanks of buildings to the drainage outlet of the community in all four communities, and the average apoptosis percentage of E.coli was 87.25% ± 8.42%.Previous studies have shown that human coronavirus (CoV) can be affected by many environmental factors and are less likely to survive in sewage than E.coli [28].Based on previous data and the results of our E.coli testing, we speculate that concentrations of the new human CoV, namely, SARS-CoV-2, could decrease more than an order of magnitude from septic tanks to the main drainage outlet of the community, either through dilution or apoptosis.
4.Discussion
4.1.The recovery and detection method of SARS-CoV-2 RNA
The whole process for testing for SARS-CoV-2 RNA in sewage is complex.Issues with the sample collection, sample pretreatment,and nucleic acid extraction of the solid and aerosol samples may result in negative results [29].Various methods for recovery of SARS-CoV-2 RNA in untreated sewage have been reported worldwide, including PEG precipitation, ultrafiltration, ultracentrifugation, filtration with an electronegative membrane, and skimmedmilk flocculation [30–35].In this study,the PEG method was used to concentrate SARS-CoV-2 in sewage during the earliest period of the COVID-19 due to its ease of on-site operation,short processing time, lack of refrigeration requirements, and low reagent cost[32,36].However, this method is more appropriate for nonenveloped viruses than enveloped viruses, and thus, little is known about their applicability for enveloped viruses such as SARS-CoV-2.Consequently, selecting the PEG method and its recovery efficiency may have a certain influence on our detection results.

Table 2 The detection of SARS-CoV-2 at the outlet of vent stacks of buildings that confirmed that patients had lived in (2020).

Table 3 Detection of SARS-CoV-2 in septic tanks of buildings where confirmed patients live in (2020).
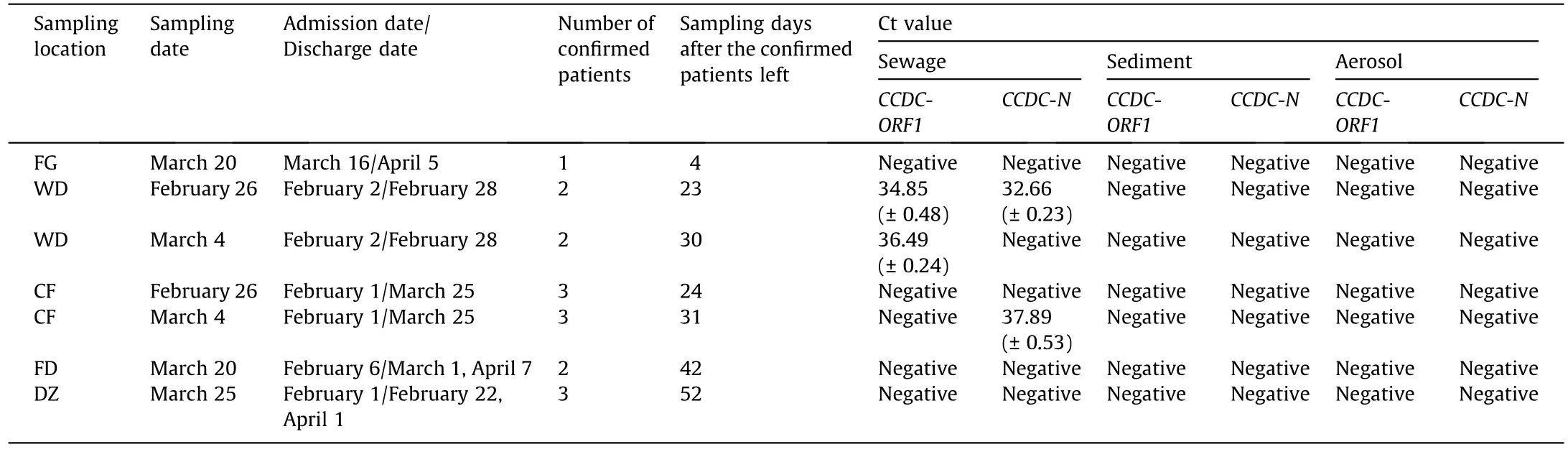
Table 4 Ct values of SARS-CoV-2 in the sewage, sediment, and aerosol in the main outlet of each community (2020).

Table 5 E.coli apoptosis within the community drainage system at the residence (2020).
The selection of primers targeting different fragments is another factor for the detection of SARS-CoV-2 RNA in sewage.Recent studies have proven that there were clear differences in the ability to differentiate between positives and negatives for low amounts of the virus with different primer–probe sets [24].The amplification results of the two target fragments of SARS-CoV-2 in sewage showed different results in the study,which might be due to the sensitivity difference of the two primer pairs during amplification.A recent study proved that the sensitivity of the primers of CCDC-ORF1 was higher than that of the primers CCDC-N at low virus concentrations[37],which might result in failed amplification with the primer pair of CCDC-N.Therefore,the verification of multitarget fragments of SARS-CoV-2 for RTPCR testing is needed to improve detection in the future.
4.2.Potential cross-transmission risks of SARS-CoV-2 in community drainage systems
The risk of cross-transmission of SARS-CoV-2 in buildings is affected by many factors, such as the number of infected patients,the interconnectedness of the sanitary plumbing system, and the viral load [38].The detection of SARS-CoV-2 RNA at the outlet of vent stacks of all selected buildings showed negative results, indicating that the risks of virus emission from buildings were low after all confirmed patients had been hospitalized.Only a small number of confirmed cases (≤3) were in the selected buildings with intact vent stacks, and the virus load was low.Furthermore,the high fluidity of the air also accelerated the removal of nucleic acid residue in the vent stack after confirmed patients were hospitalized.The low positive detection rates at the outlet of vent stacks in this study can prove that the continuous emission of SARSCoV-2 to environment via vent stack is low after the confirmed case were hospitalized.However, some previous studies have reported that the virus could spread via ventilation systems within buildings during the epidemic period of SARS,such as the events in Hong Kong in 2003 and in Guangdong in 2020[16,39].Therefore,it is still necessary to strengthen prevention in the early stage of the epidemic to eliminate possible transmission risks, especially for buildings with old ventilation facilities.Aerosol transmission within buildings remains a concern when the epidemic becomes more severe [40].The timely isolation of confirmed patients and maintaining the ventilation system intact are necessary to prevent the widespread transmission of the virus within buildings.
After the patients were hospitalized, negative SARS-CoV-2 RNA results were obtained in all sediment or aerosol samples in the septic tanks from the 4th day to the 52nd day.Only a few sewage samples were found to be positive.However, other studies found that enveloped viruses showed a tendency of higher partitioning in suspended solids of sewage[29].A recent study found that SARS-CoV-2 from primary clarified sludge samples was solid-rich and showed high sensitivity for SARS-CoV-2 detection [41].Another study showed that 90% of SARS-CoV-2 RNA was likely to be present in the liquid phase of sewage but not the suspended solid phase[42].This finding is similar to that found for mouse hepatitis virus(MHV),where approximately 70%of the enveloped virus existed in sewage liquids at equilibrium [43].The different results might be because the virus nucleic acid could be packaged in suspended solids or released into sewage under certain circumstances.Studies on virus partitioning in different phases may provide more information to assess the potential risk of SARS-CoV-2 in community drainage systems.
4.3.Implications for sewage surveillance of SARS-CoV-2
This is a very early study on the risk of SARS transmission within community sewerage systems after the COVID-19 patients were identified.The study provided the earliest experience with sewage surveillance for SARS-CoV-2.Although there were no documented confirmed cases for 31 days after the confirmed cases were hospitalized, the SARS-CoV-2 was still positively detected at the outlet of the community drainage system with comparable viral load attributed to the confirmed patients [44].The SARSCoV-2 RNA could also be excreted from recovered confirmed cases who were able to protract the viral RNA shedding in feces as long as days to three months [45–47].However, the time of positive detections in sewage were all earlier than the time that confirmed cases discharged from the hospital,thus ruling out this possibility.The results showed that hidden asymptomatic patients might be in the community during the study period.A recent study also showed that the decline in COVID-19 cases could precede the decline in SARS-CoV-2 RNA [42].Thus, sewage surveillance could be adopted as an effective tool for predicting and assessing potential pandemics,which is very useful for tracing the source of SARSCoV-2.Furthermore, the sewage sampling location would be an important factor for detection.The virus concentration might decay and be diluted by an order of magnitude even from the building septic tanks to the outlet of the community drainage system based on the results of the E.coli test.A feasible sewage sampling strategy could include rapid sampling to target the suspected area and conduct further screening.
5.Conclusions
This study conducted a comprehensive investigation of the occurrence and potential transmission of SARS-CoV-2 in a community sewage drainage system during the early days of the COVID-19 pandemic.The data suggest infection risk could be eliminated shortly after the confirmed patient left the building (< 4 days)under the condition of an intact new building structure.Less than 23 days after the confirmed patients were hospitalized, negative results for SARS-CoV-2 nucleic acid testing in the septic tanks were obtained.SARS-CoV-2 RNA could be more easily detected in sewage than in sediment or aerosols within the community drainage system.The virus concentration could be decayed and diluted by an order of magnitude even from the building septic tanks to the outlet of the community drainage system based on the E.coli indicator test.The study provided the earliest experience with sewage surveillance for SARS-CoV-2, and sewage surveillance could be adopted as an effective tool for predicting and assessing the potential pandemic,which is very useful for tracing the source of SARSCoV-2 at the community level.
Acknowledgments
This research was funded by the projects of the Major Program of National Natural Science Foundation of China (52091543),Tsinghua University Spring Breeze Fund (20213080026), and the Chinese Academy of Engineering (2020-ZD-15).
Compliance with ethical guidelines
Qian Dong, Jun-Xiong Cai, Yan-Chen Liu, Hai-Bo Ling, Qi Wang,Luo-Jing Xiang, Shao-Lin Yang, Zheng-Sheng Lu, Yi Liu, Xia Huang,and Jiu-Hui Qu declare that they have no conflict of interest or financial conflicts to disclose.
- Engineering的其它文章
- Profound Diversity of the N-Glycome from Microdissected Regions of Colorectal Cancer, Stroma, and Normal Colon Mucosa
- The Glycome and Glycomedicine
- Most Efficient Reaction Bolsters Prospects for Low-Carbon Ammonia
- Periodic Changes in the N-Glycosylation of Immunoglobulin G During the Menstrual Cycle
- Removable Dyes—The Missing Link for In-Depth N-Glycan Analysis via Multi-Method Approaches
- Serum N-Glycan Markers for Diagnosing Significant Liver Fibrosis and Cirrhosis in Chronic Hepatitis B Patients with Normal Alanine Aminotransferase Levels