
Effect of low dose laser cycloplasty on deepening anterior chamber in chronic angle-closure glaucoma
2023-12-14 08:52:24XuanLiZhengHaiShuangLinXiaoJieWangJiaQianLiYanQianXieShaoDanZhangYuanBoLiang
Xuan-Li Zheng, Hai-Shuang Lin, Xiao-Jie Wang, Jia-Qian Li, Yan-Qian Xie,Shao-Dan Zhang, Yuan-Bo Liang
1Wenzhou Medical University, Wenzhou 325027, Zhejiang Province, China
2National Clinical Research Center for Ocular Diseases, Eye Hospital, Wenzhou Medical University, Wenzhou 325027,Zhejiang Province, China
3Glaucoma Research Institute, Wenzhou Medical University,Wenzhou 325027, Zhejiang Province, China
Abstract
● KEYWORDS: chronic angle-closure glaucoma; low dose laser cycloplasty; anterior chamber depth; intraocular pressure
INTRODUCTION
Chronic angle-closure glaucoma (CACG) is caused by permanent closure of the angle due to peripheral anterior synechiae, inducing an increase in intraocular pressure (IOP).It is estimated that about 1.5 million people above 40 years old are blind in both eyes from CACG in China[1].Shallow anterior chamber depth (ACD) and narrow anterior chamber angle (ACA) have been identified as significant risk factors for CACG[2].Currently, the first-line treatment for chronic angle closure is Nd:YAG laser peripheral iridotomy (LPI)[3].
However, LPI is not completely effective in preventing longterm asymptomatic rises in IOP, and also unable to deepen the ACD[4].Lens extraction has become first-line treatment in the management of angle closure in patients with or without coexisting cataract, as age-related lens growth plays a major role in the mechanism of CACG[5].However, early lens extraction remains a topic of controversy, while the relatively high costs associated with cataract surgery also pose limitations on its widespread accessibility[6].
Transscleral cyclophotocoagulation (TSCPC) is a procedure that uses a semiconductor diode laser to target the pigmented ciliary epithelium, leading to a reduction in aqueous production and subsequent decrease in IOP[7].TSCPC can serve as the primary treatment for medically uncontrolled CACG, with significant reductions in IOP observed within 24h of the procedure[8].Additionally, compared to filtration surgery and glaucoma drainage devices, TSCPC offers several advantages including technical ease and low costs[9].However, despite its efficacy, TSCPC is always associated with a high incidence of complications[10].In order to minimize complications,our team have implemented a low-dose approach to cyclophotocoagulation that utilizes pulse and quadrant application, which was named as low-dose laser cycloplasty(LCP)[11].We have successfully employed LCP in the treatment of patients with malignant glaucoma and acute angle closure,resulting in increased ACD, re-opened ACA and reduced IOP with fewer complications[11-14].To evaluate the efficacy of LCP in lowering IOP and deepening the anterior chamber in patients with CACG, a retrospective case series was conducted.
SUBJECTS AND METHODS
Ethical ApprovalThis retrospective case series adhered to the principles of the Declaration of Helsinki and was granted approval by the Ethics Committee of the Eye Hospital of Wenzhou Medical University (No.2019-201-K-181).This study collected data of patients diagnosed with CACG who opted for LCP due to financial constraints.
Study Design and ParticipantsCACG were defined as eyes with a chronically elevated IOP (>21 mm Hg) along with glaucomatous optic neuropathy or visual field defect, the absence of visible posterior trabecular meshwork for ≥270°,without symptoms or signs of a prior acute attack, including glaucomatous fleck, keratic precipitates, or iris atrophy.Patients who underwent LCP and had at least 1y of follow-up after the procedure were included.Exclusion criteria included secondary CACG and the history of intraocular surgery.
Low-Dose Laser Cycloplasty ProceduresA transscleral diode 810-nm laser and contact G-probe were used as necessary to the treatment (Supra 810, Quantel Medical,France).The standard settings were 2000-ms duration and 1200 mW power.Increase the energy gradually in 100 mW increments until a burst sound was heard, then used the energy level for procedure.After a retrobulbar anesthesia or subtenon anesthesia (1:1 mixture of lidocaine and bupivacaine),the ciliary body was identified by transillumination.The G-probe was seated at the anterior aspect of the ciliary body,which were approximately 2.0 mm posterior to the limbus over the conjunctival surface.The treatment consisted of ≤15 applications over 4 to 6 o’clock or 6 to 8 o’clock (60 degrees in total) of the ciliary body.The power was modified until an effective bursting sound was obtained, and it was lowered if pigment dispersion or air bubbles were observed in the anterior chamber.After LCP, 0.1% dexamethasone ointment was placed.
Data CollectionBaseline information, including age, gender,axial length, lens thickness, central corneal thickness, visual acuity, IOP, ultrasound biomicroscopy (UBM) measurements and the number of glaucoma medications, was obtained for all participants.Biometric data inclusive of axial length, lens thickness and central corneal thickness was measured using a single optical biometer (Lens Star, Haag-Streit, USA).IOP was measured three times using non-contact tonometry (Full Auto Tonometer TX-20, Canon, Japan), and the average value was recorded.UBM was performed by a certified inspector utilizing the same instrument (50 MHz, AVISO, Quantelmedical, France).Gonioscopy was performed by a glaucoma specialist before and after the LCP procedure, utilizing a Goldmann-type 1-mirror lens.Postoperative information was gathered at 1d, 1wk, 1, 3, 6, and 12mo and last followup, consisting of visual acuity, IOP, the number of glaucoma medications, and UBM measurements.The intraoperative and postoperative complications, laser or surgical reinterventions were documented as well.
For UBM examination, radial scans were conducted at the 12, 6, 3, and 9 o’clock positions centered over the limbus,corresponding to the superior, inferior, nasal, and temporal quadrants.Additionally, horizontal perpendicular scans were conducted over the pupil center.The following UBM parameters were examined by the built-in caliper in the equipment.The definitions of these quantitative parameters were: 1) central ACD is the distance from the corneal endothelium to the anterior surface of the lens; 2) angle opening distance500(AOD500), is the distance between the inner corneal surface and the anterior iris surface measured on a line perpendicular to the plane of the trabecular meshwork at 500 μm from the scleral spur; 3) trabecular-iris angle (TIA)is measured with its apex at the scleral spur and the arms of the angle passing through a point on the trabecular meshwork at 500 μm from the scleral spur and the point on the anterior surface of the iris perpendicularly opposite; 4) maximum ciliary body thickness (CBTmax) is the distance from the most inner point of the ciliary body perpendicular to the inner surface of sclera or its extended line; 5) trabecular-ciliary process angle (TCPA) is measured with its apex at the scleral spur, one arm along the posterior corneal surface, and another arm along the most anterior surface of the ciliary body[15].The superior, inferior, nasal, and temporal aspects of these parameters were averaged.Vitreous chamber depth (VCD) is defined as axial length minus central corneal thickness, lens thickness and ACD.
Statistical AnalysisCategorical variables are presented as frequencies and percentages.Continuous variables of normal distribution are presented as means and standard deviations,whereas continuous variables of skewed distribution are presented as median and range.IOP, number of glaucoma medications and ACD at baseline and each follow-up were compared using pairedttest, and anterior segment parameters were compared using Wilcoxon signed-rank test.Statistical analyses were performed using SPSS (version 24.0 for Windows, SPSS, Inc., Chicago, IL, USA).AP-value <0.05 was considered statistically significant.

Figure 1 The mean IOP and number of glaucoma medications at various time points after LCP IOP: Intraocular pressure; LCP: Lowdose laser cycloplasty.
RESULTS
Seven eyes of seven patients were included in this study.Among these patients, there were three males and four females, with the mean age of 38.9±11.0y (range, 22 to 58y)at baseline.The mean axial length was 20.6±0.3 mm.Baseline characteristics of these patients are shown in Table 1.The mean follow-up period of all 7 eyes was 27.1±13.7mo (range,16 to 48mo).
On average, the IOP and glaucoma medications were consistently lower than the baseline throughout the study(Figure 1).The mean pre-operative IOP was 26.1±6.1 mm Hg(range, 18 to 35.6 mm Hg).The mean post-operative IOP was 16.8±4.9 mm Hg (range, 10.7 to 26.4 mm Hg) at 12mo(t=2.312,P=0.06) and 14.9±3.1 mm Hg (range, 10.5 to 20.1 mm Hg) at final follow-up (t=2.903,P=0.027).In terms of glaucoma medications, the mean number of medications at baseline was 3.1±1.1, and this number decreased at every postoperative time point compared to baseline, with a reduction to 0.3±0.8 medications at 12mo post-operation (t=5.774,P<0.001) and 0.4±1.1 medications at the final follow-up(t=4.608,P=0.001).
The baseline mean ACD was 1.65±0.33 mm (range, 1.26 to 2.25 mm), mean VCD:AL was 0.67±0.04 (range, 0.65 to 0.75).Following LCP, the mean short-term ACD increased to 1.85±0.38 mm (range, 1.4 to 2.31 mm), while the longterm ACD was 1.98±0.43 mm (range, 1.24 to 2.67 mm,t=-2.167,P=0.073).The mean short-term VCD:AL decreased to 0.66±0.04 (range, 0.64 to 0.76), while the long-term VCD:AL was 0.65±0.05 (range, 0.62 to 0.76; Table 2).Of the 6 eyes(85.7%) with increased ACD after LCP, 5 eyes (71.4%) had a long-term deepening of more than 0.3 mm (Figure 2).Prior to LCP, all eyes exhibited at least three quadrants of closure.Following LCP, five eyes (71.4%) showed an opening of at least one quadrant, and one eye (14.3%, patient 6) achieved a fully open angle.Figure 3 shows comparisons of the anterior segment parameters, where prior to LCP treatment, UBM examination showed a median AOD500and TIA of 0.05 mm (range, 0 to 0.30 mm) and 5.1° (range, 0 to 31.97°), respectively.The short-term AOD500increased to 0.16 mm (range, 0 to 0.64 mm) and the long-term to 0.53 mm(range, 0.42 to 0.91 mm,Z=-2.797,P=0.015).The short-term TIA increased to 16.3° (range, 0 to 48.57°) and the long-term to 45.9° (range, 40.2 to 59.4°,Z=-2.797,P=0.015).AOD500and TIA in each quadrant also increased compared to before treatment.The reopening of the ACA was observed in 6 eyes(85.7%).Regarding ciliary body parameters, the median CBTmax and TCPA showed an increase in value but no statistical difference was observed (P=0.057).
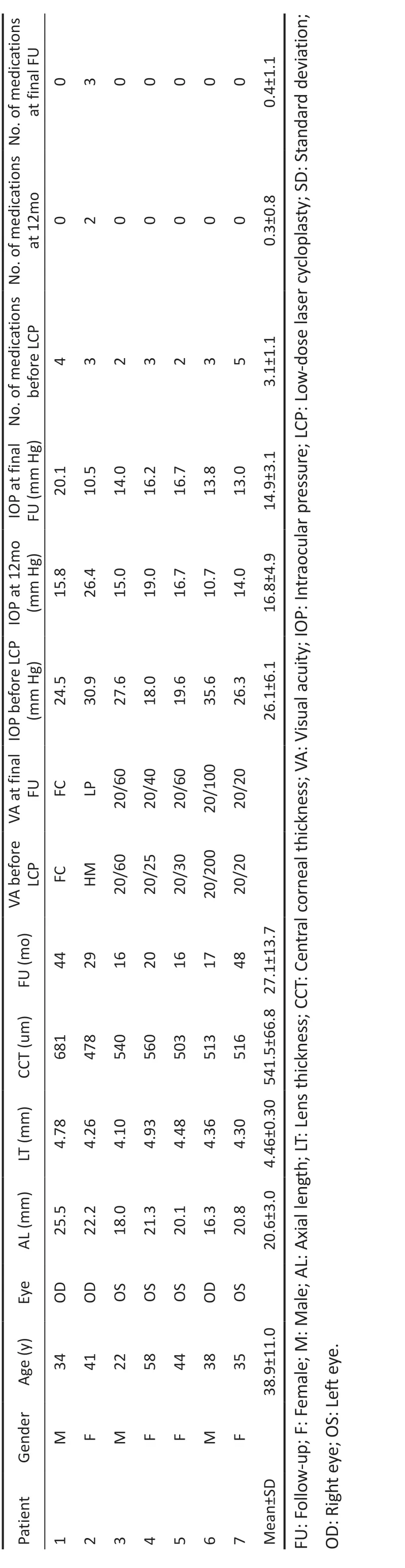
Table 1 Pre- and post-treatment data for all patients
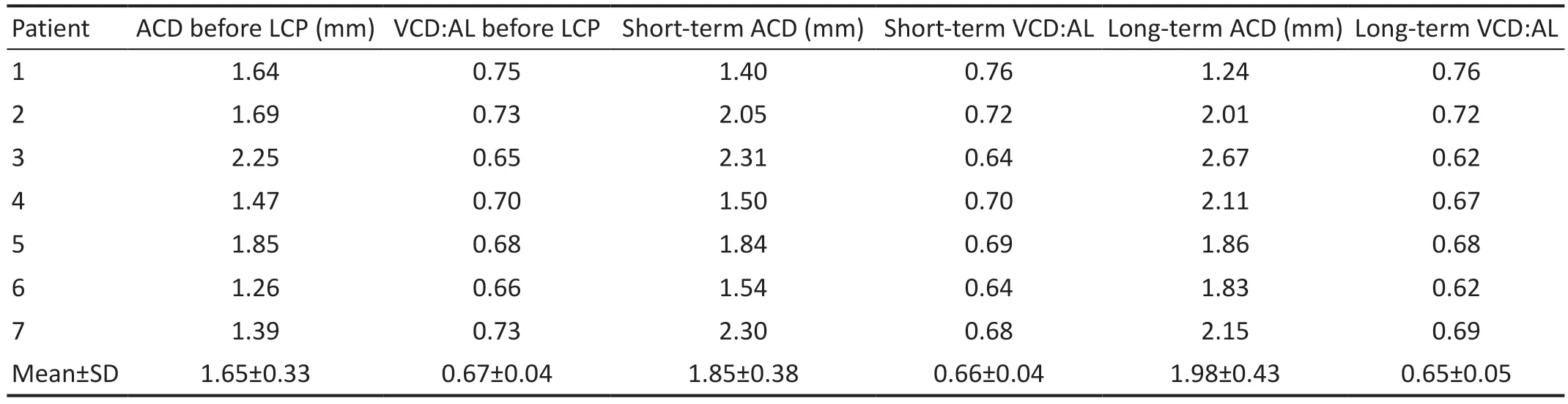
Table 2 ACD before and after low-dose laser cycloplasty

Figure 2 A 35-year-old female patient (patient 7) underwent UBM before and after LCP A: The central ACD was 1.39 mm and VCD:AL was 0.73 prior to LCP; B: UBM at 6 o’clock showed the anterior chamber angle closure before the LCP; C: The central ACD deepened to 2.30 mm and VCD:AL decreased to 0.68 one day after the LCP;D: UBM at 6 o’clock showed the open of the anterior chamber angle one day after LCP.ACD: Anterior chamber depth; UBM:Ultrasonographic biomicroscopy, LCP: Low-dose laser cycloplasty,VCD: Vitreous chamber depth; AL: Axial length.
Following laser treatment, all eyes had different degrees of anterior chamber inflammatory reaction.Ciliary body detachment was observed in three eyes (patients 1, 3 and 6), with two eyes recovering spontaneously and one eye(patient 1) requiring treatment with methylprednisolone.Cataract progression was observed in two eyes (patients 1 and 4).Transient increases in IOP greater than 25 mm Hg were observed in two eyes at 3 and 12mo, respectively, but were successfully managed with medication.None of the treated eyes experienced hypotony, hypotony maculopathy,corneal decompensation, pupillary abnormalities, conjunctival scarring, sympathetic ophthalmia, or phthisis bulbi.
DISCUSSION
The findings of this study provide evidence for the effectiveness of LCP in the management of CACG.Our results clearly demonstrate that LCP effectively reduces IOP and the number of glaucoma medications over an extended period of followup.In addition, our study highlights the ability of LCP to deepen the ACD and reopening the ACA.

Figure 3 Ultrasound biomicroscopy parameters of anterior segment in each quadrant before and after LCP Shown in median.LCP: Low-dose laser cycloplasty; AOD500: Angle opening distance500; TIA: Trabecular-iris angle; CBTmax: Maximum ciliary body thickness; TCPA: Trabecular-ciliary process angle.
Since 1972, TSCPC has been a viable treatment option for refractory glaucoma patients to decrease IOP and slow the progression of the disease[10].With advancements in surgery,TSCPC has also been utilized in the treatment of angle-closure glaucoma due to its simple operation, effective IOP-lowering properties, and decreasing economic costs[16-17].However, the high incidence of severe complications has limited its widespread use[10].To address these challenges, modified procedures, such as micropulse TSCPC (MP-TSCPC) and LCP, have been introduced.These techniques offer a promising alternative to traditional TSCPC, aiming to maximize the IOP-lowering effect while minimizing the risk of complications[11,18].The LCP design concept shares similarities with that of MP-TSCPC, but the LCP technique is a modified version of TSCPC that doesn’t require the purchase of an additional MP-TSCPC machine,resulting in lower costs.Both of them utilizes fewer laser spots and lower total laser energy, resulting in a better safety profile with comparable efficacy to traditional TSCPC[12,19].In a study by Emanuelet al[20], 84 eyes with uncontrolled glaucoma were treated using MP-TSCPC.The results showed a significant decrease in mean IOP and glaucoma medications from 27.7±10.3 mm Hg with 3.3±1.0 glaucoma medications preoperatively to 11.1±4.4 mm Hg with 2.3±1.5 glaucoma medications at 12mo postoperatively.Nguyenet al[21]treated 95 glaucoma eyes with MP-TSCPC.The mean preoperative IOP and glaucoma medications was 25.1±5.3 mm Hg with 3.0±1.1 glaucoma medications,and reduced to 17.5±5.1 mm Hg with 1.4±1.0 glaucoma medications at 12mo postoperatively.As for LCP, our previous study treated acute angle-closure glaucoma with LCP and found that it effectively lower the IOP 26.6 (7.3, 60.0) mm Hg at baseline to 15.5 (9.6, 20) mm Hg at 3mo[12].In this current study, LCP resulted in a reduction of IOP and glaucoma medications from 26.1±6.1 mm Hg with 3.1±1.1 glaucoma medications preoperatively at baseline to 16.8±4.9 mm Hg with 0.3±0.8 glaucoma medications after 12mo of follow-up.A study by Nguyenet al[21]found that the rate of choroidal effusion after MP-TSCPC was 3.2%.A previous study on 61 glaucoma eyes treated with MP-TSCPC found cataract progression in 10 out of 25 phakic eyes, with 5 eyes experiencing vision loss of ≥2 lines and requiring cataract extraction[22].Similar to the complications mentioned above regarding MP-TSCPC, our study found that three patients experienced ciliary body detachment after LCP, but all recovered within one week.Two patients developed progressive cataract, one of whom underwent phacoemulsification combined with intraocular lens implantation.
Our study has shown that LCP has a notable effect on deepening the ACD and reopening the ACA.This is in contrast to previous studies using LPI or argon laser peripheral iridoplasty to treat primary angle-closure glaucoma (PACG),where no ACD deepening was observed[3,23].In our study, LCP deepened the anterior chamber in 6 eyes (85.7%).In a prior study by Mouet al[24], 134 primary angle-closure suspect eyes were treated with LPI, with 79 eyes undergoing gonioscopy.They found that thirteen treated eyes (16.5%) had a completely open angle, while 74 eyes (93.7%) had opened by at least one quadrant.In our study, five eyes (71.4%) had opened by at least one quadrant and one eye (14.3%) had a completely open angle.Additionally, Liuet al[25]reported on LPI treatment in 97 angel clousre eyes, observing an increase in AOD500and TIA from 0.11±0.10 mm and 8.51±7.02° to 0.22±0.14 mm and 15.70±8.37°, respectively, one week after treatment (P<0.001).In our study, LCP resulted in a significant increase in AOD500and TIA from 0.05 mm (0, 0.30 mm) and 5.1° (0, 31.97°) to 0.53 mm (0.42, 0.91 mm) and 45.9° (40.2°, 59.4°), respectively(P=0.015).LCP led to a more pronounced widening of the ACA.
There is currently a dearth of research on the effects of ciliary body laser treatment, including LCP, TSCPC, and MP-TSCPC,on the anterior segement parameters in CACG.Our previous study[11]found that LCP could deepen the anterior chamber in cases of malignant glaucoma.Furthermore, we discovered that LCP could deepen the ACD and open the ACA in acute primary angle clousre glaucoma, resulting in an increase in ACD from 1.44±0.48 mm to 1.66±0.34 mm and widening of the ACA in 86.7% of cases[12].Similarly, Shiet al[26]reported that LCP deepened the ACD from 1.508 (1.090-2.037) mm to 1.713 (1.286-2.057) mm in 20 patients with prolonged acute PACG.In this study, we examined the effects of LCP on the anterior chamber in CACG, and found that LCP successfully deepened the ACD from 1.65±0.33 mm to 1.98±0.43 mm and reopened the ACA in 6 eyes (85.7%).LCP reduces IOP by reshaping the anterior chamber and partially reopening the closed angle, rather than by decreasing aqueous production[27].This is achieved by shrinking the ciliary processes and expanding the space between the ciliary processes and lens equator, which reduces ciliary flow resistance and trans-lens pressure differential.This causes the lens to move back and deepen the anterior chamber.With the deepening of the anterior chamber, the contact between the trabecular meshwork and the root of the iris may be opened, the ACA widened, and aqueous humor drainage restored.Given the crucial role of ACD in angle-closure glaucoma, we recommend that the application of LCP in angle-closure glaucoma receive greater attention.Additionally, investigating changes in anterior segement parameters during this process would also be valuable.
The present study has a few limitations like small sample size, retrospective nature, and lack of comparative group.A prospective study with a larger sample size and a comparative group is needed to validate our results and further evaluate the safety and efficacy of LCP in CACG treatment.In summary, the effectiveness in deepening anterior chamber and re-opening the ACA, reduction in IOP and glaucoma medication, demonstrates LCP as a promising treatment option for patients with CACG.
ACKNOWLEDGEMENTS
Foundations:Supported by the Program for Zhejiang Leading Talent of S&T Innovation (No.2021R52012); Key Research and Development Projects of Zhejiang Province(No.2022C03112); the Basic Scientific Research Program of Wenzhou (No.Y2020365).
Conflicts of Interest: Zheng XL,None;Lin HS, None;Wang XJ, None;Li JQ, None;Xie YQ, None;Zhang SD,None;Liang YB, None.
 International Journal of Ophthalmology2023年12期
International Journal of Ophthalmology2023年12期
- International Journal of Ophthalmology的其它文章
- Endoscopic transnasal optic canal decompression for pediatric traumatic optic neuropathy with no light perception
- Three siblings with gyrate atrophy of the choroid and retina: a case report
- Glaucoma among Saudi Arabian population: a scoping review
- Visualized analysis of research on myopic traction maculopathy based on CiteSpace
- Different approaches for treating myopic choroidal neovascularization: a network Meta-analysis
- Agreements’ profile of Scheimpflug-based optical biometer with gold standard partial coherence interferometry