
Surgical outcome comparisons of multifocal lOLs of Lentis Comfort LS-313 MF15 and Tecnis Eyhance DlB00V
2023-12-14 08:52:24KyoheiSugawaraRyosukeItoHiroshiHoriguchiKeiMizobuchiSatoshiKatagiriHisatoGunjiTadashiNakano
Kyohei Sugawara, Ryosuke Ito, Hiroshi Horiguchi, Kei Mizobuchi, Satoshi Katagiri, Hisato Gunji,Tadashi Nakano
Department of Ophthalmology, the Jikei University School of Medicine, Tokyo 105-8461, Japan
Abstract
● KEYWORDS: cataracts; intermediate distances;intraocular lens; multifocal; surgical outcomes
INT RODUCTION
Intraocular lens (IOL) implantation is the most commonly performed surgical procedure for the treatment of cataracts worldwide[1-3].Several types of IOLs, such as monofocal,multifocal, accommodating, and extended depth of focus(EDOF) IOLs[3-5], are available.Monofocal IOLs, or the classic type of IOLs, restore visual resolution to the pre-cataract level but only focus on one distance (i.e., near or far)[6-7].Therefore,the use of external devices, such as glasses or contact lenses, is often still required, resulting in ongoing issues.In contrast, multifocal IOLs focus on two or more distances simultaneously; however, compared with monofocal IOLs,multifocal IOLs result in decreased resolution at each distance,and the incidence of halo and glare is higher[8-10].EDOF IOLs extend the depth of focus compared with monofocal IOLs and have demerits similar to those of multifocal IOLs[4-5].
Lentis Comfort LS-313 MF15 (Oculentis GmbH, Berlin,Germany) is a multifocal IOL with an additional +1.5 dioptre(D) that is designed to enhance intermediate performance while suppressing disturbing photic phenomena[11].Tecnis Eyhance DIB00V (Abbott Medical Optics, Inc., Santa Ana, CA, USA) is an enhanced monofocal IOL designed to improve intermediate distance vision, and its outcomes are comparable with those of aspheric monofocal IOLs[4].Reports have indicated that both IOLs provide better intermediate visual acuity (VA) than that of conventional monofocal IOLs[4,8-13]with similar contrast sensitivity[4,10,13]and similar incidence of halo and glare symptoms[4,13].Furthermore, both IOLs are available under the national healthcare insurance in Japan.Nevertheless, some differences are present between the two IOLs.First, except for the higher-order aspheric anterior surface that creates continuous power progression, the Eyhance DIB00V lenses have the same structure as that of the previous Tecnis series IOLs.Moreover, the LS-313 MF15 lenses have a plate design,which may affect the postoperative refractive values.Second,in contrast to the LS-313 MF15 lenses, which are ultraviolet light-filtering IOLs, there are two types of Eyhance DIB00V lenses with different wavelength transmission properties:ICB00 lenses, which filter ultraviolet light, and the Eyhance DIB00V lenses, which filter short wavelength light.Previous reports on Eyhance DIB00V, which are IOLs that filter short wavelength light, are rare.Third, the number of additional power sources differs.The LS-313 MF15 lenses are refractive multifocal IOLs with an addition of +1.5 D[14], whereas the Eyhance DIB00V lenses have an addition of approximately+0.5 D[15].
Several previous studies have compared these lenses with conventional monofocal IOLs[4,8-13].However, no study has compared LS-313 MF15 with Eyhance DIB00V.In Japan,LS-313 MF15 and Eyhance DIB00V are available at a relatively low cost as they are covered by the national health insurance system.The wide variety in the choice of lenses makes it difficult for surgeons to determine a suitable IOL for patients requiring intermediate distance vision.Therefore, we designed a study to perform a direct comparison between LS-313 MF15 and Eyhance DIB00V with enhanced performance at intermediate distances.This study aimed to compare the surgical outcomes of these two IOLs directly.
SUBJECTS AND METHODS
Ethical ApprovalThe Institutional Review Board of the Jikei University School of Medicine approved this retrospective study, which was conducted in accordance with the principles of the Declaration of Helsinki [approval number: 34-084(11231)].This study did not involve an intervention or utilise any human biological specimens or personal information that required special care; thus, the requirement for obtaining informed consent from each research subject was waived according to the Ethical Guidelines for Medical and Health Research Involving Human Subjects (the Japanese Ministry of Health, Labour and Welfare).Documents approved by the Institutional Review Board of the Jikei University School of Medicine were posted on the website.We also posted the information regarding this research on the bulletin board in our hospital, guaranteeing the subjects the right to refuse participation in this study at any time.
PatientsAll patients who underwent cataract surgery with LS-313 MF15 or Eyhance DIB00V IOL implantation at the Jikei University Kashiwa Hospital between July 2021 and March 2022 were retrospectively enrolled in this study.The exclusion criteria were corneal astigmatism over 1.0 D; other ophthalmic diseases that affect visual function, such as glaucoma, retinal diseases, and amblyopia; and systemic diseases that interfere with examinations, such as dementia.
Subjects and Ophthalmic ExaminationsInformation regarding the patients’ age, sex, medical history, and ophthalmic examinations before the cataract surgery and one and three months postoperatively were collected retrospectively.Furthermore, the surgical records were reviewed to collect information regarding the implanted IOLs and other relevant factors.The recorded information included the distance-corrected or uncorrected distance VAs, axial lengths [measured using AL-Scan (Nidek Co.Ltd., Gamagori,Japan)], objective refractive errors, the refractive power of the cornea and implanted IOLs, contrast sensitivity, depth of focus,visual discomfort due to the presence of halos and glare, and responses to the 14-item Visual Function Index Questionnaire.Huiet al[16]reported that the objective refractive values for segmental multifocal IOLs are myopic and inaccurate.Therefore, the postoperative refractive values were evaluated using subjective equivalent spherical power.The 14-item Visual Function Index Questionnaire and halo and glare tests were performed on both eyes in patients with the same IOL implanted bilaterally.VAs, defocus curves, and contrast sensitivity were evaluated in each eye.Each eye of the patients with the same IOL implanted bilaterally were also evaluated.Decimal uncorrected and distance-corrected distance VAs were measured using Landolt C charts from Takagi Seiko (Nakano,Japan) at a distance of 5 m.Intermediate and near distance VAs of 1 m, 70, 50, and 30 cm were measured using Landolt C charts from T.M.I Co.Ltd.(Saitama, Japan).Distancecorrected VAs were measured under distance correction at all distances to minimize the effects of refractive error and induced astigmatism.These values were subsequently converted to logMAR best-corrected VA values.The objective refractive errors and refractive power of the cornea were measured using TONOREF Ⅱ (Nidek Co.Ltd., Japan).Contrast sensitivity was measured using the CSV-1000 chart (Vector Vision, Greenville,OH, USA) at spatial frequencies of 3, 6, 12, and 18 cycles per degree.This inspection was conducted under best-correction and mesopic conditions without glare.Both eyes of patients with IOLs implanted bilaterally were examined.A defocus curve was created for ten defocus levels from +1.5 to −3.0 D in 0.5 D steps.Visual discomfort due to the presence of halos and glare was assessed subjectively by the patient.The Halo& Glare Simulator (Eyeland-Design Network GmbH, Vreden,Germany) was displayed on an iPad and shown to the patient,and the degree of symptoms was quantified and recorded.The degree of symptoms was evaluated to determine the sizes of the halo and glare with a fixed intensity of 50% for the examination.The halo and glare degrees were assessed from 0 to 100%.The translated version (from English to Japanese) of the 14-item Visual Function Index Questionnaire[17]was used in this study; however, several terms that were uncommon in Japanese culture were modified in the questionnaire (e.g.,from “writing checks or filling out forms” to “writing letters or documents”).The questions were divided into four groups:near-distance vision (questions 1-6), intermediate-distance vision (questions 7-10), far-distance vision (questions 11-13),and night-time vision (question 14).The patients answered each question using a satisfaction scale ranging from zero(very dissatisfied) to four (very satisfied).The total 14-item Visual Function Index Questionnaire score was calculated as the mean score of each answered scale multiplied by 25.The Halo & Glare Simulator and 14-item Visual Function Index Questionnaire were only administered to patients with the same IOLs implanted bilaterally.
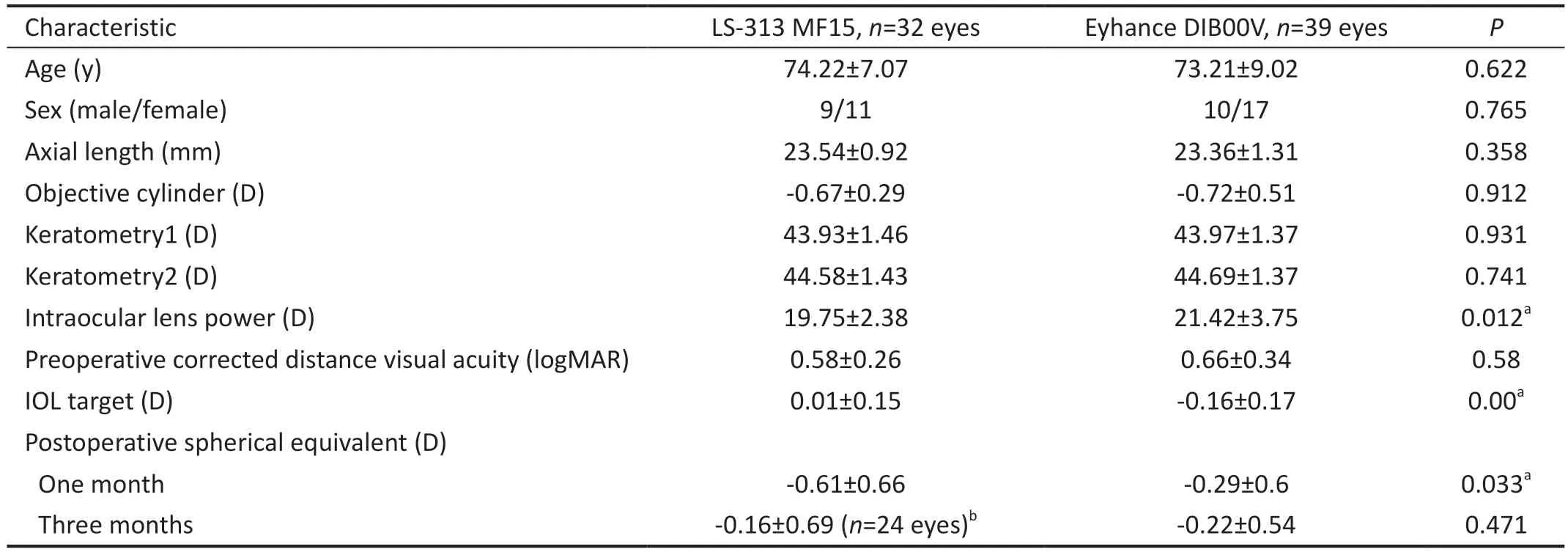
Table 1 Patient demographics, preoperative ophthalmic data, and postoperative spherical equivalent data
Cataract SurgeryPreoperative calculation of the required dioptre power for IOL implantation was determined by two researchers (Ito R and Sugawara K) using the Barrett Universal II formula.Emmetropia was targeted for all eyes undergoing LS-313 MF15 lens implantation, whereas the negative value closest to zero was targeted for all eyes undergoing Eyhance DIB00V implantation.Each surgeon used standard smallincision, phacoemulsification cataract extraction surgical techniques to implant the IOLs.Using a validated insertion system, the IOLs were folded for implantation and inserted into the capsular bag through a clear corneal, limbal, or scleral-tunnel incision of 2.4 mm as per the surgeon’s standard technique.Anterior capsulotomies were continuous,curvilinear capsulorhexis approximately 5.0-5.5 mm in diameter performed using the manual (rhexis) method.Lens removal was performedviaconventional phacoemulsification and aspiration.Ophthalmic viscosurgical device materials,preoperative and intraoperative medications, and the wound closure method were determined at the surgeon’s discretion.The surgeries were performed by 10 surgeons, and only cases with no surgical complications were included in this study.
Statistical AnalysesThe preoperative data of the two groups(LS-313 MF15 and Eyhance DIB00V) were summarised and statistically compared using the Mann-WhitneyUtest or Fisher’s exact test.The uncorrected and distance-corrected distance VAs at each distance one month postoperatively were compared using the Mann-WhitneyUtest.The subjective and objective refractive errors; differences between the targeted and postoperative refractive errors; contrast sensitivities at 3,6, 12, and 18 cycles per degree; depths of focus; and the 14-item Visual Function Index Questionnaire scores three months postoperatively were compared using the Mann-WhitneyUtest.Statistical analyses were conducted using Python 3.9.6(Python Software Foundation, Wilmington, DE, USA), and statistical significance was set atP<0.05.
RESULTS
DemographicsAmong the 71 eyes (47 patients) included in this study, 32 eyes (20 patients) underwent LS-313 MF15 lens implantation, and 39 eyes (27 patients) underwent Eyhance DIB00V lens implantation.The preoperative age, sex, axial length, objective cylinder, keratometric power, and corrected distance VA did not differ between the two groups (Table 1).Ophthalmic examinations and the uncorrected and distancecorrected VAs at each distance were evaluated preoperatively and one month postoperatively in both groups.
The contrast sensitivities at 3, 6, 12, and 18 cycles per degree and depths of focus were evaluated in 24 eyes (16 patients)in the LS-313 MF15 group and 39 eyes (27 patients) in the Eyhance DIB00V group three months postoperatively.The preoperative age, sex, axial length, objective cylinder,keratometric power, and corrected distance VA did not differ between the two groups.Due to the deterioration of their general condition and other reasons, some patients were not able to continue with the follow-up visit three months postoperatively.
Refraction and Visual AcuityEmmetropia (±0.5 D) was roughly targeted as the postoperative refraction.The target was set as the absolute value closest to 0 in the LS-313 MF15 group and the negative value closest to 0 in the Eyhance DIB00V group.Thus, the targeted refractions were 0.01±0.15 D in the LS-313 MF15 group and -0.16±0.17 D in the Eyhance DIB00V group (P=0.00).The postoperative spherical refraction was -0.61±0.66 and -0.29±0.6 D (P=0.033) one month postoperatively and -0.16±0.69 and -0.22±0.54 D(P=0.471) three months postoperatively in the LS-313 MF15 and the Eyhance DIB00V groups, respectively (Table 1).
One month postoperatively, the distance-corrected VAs(logMAR) were -0.01±0.12 and -0.04±0.08 at 5 m, 0.11±0.15 and 0.13±0.16 at 1 m, 0.2±0.18 and 0.23±0.16 at 70 cm,0.38±0.21 and 0.36±0.18 at 50 cm, and 0.64±0.22 and 0.62±0.2 at 30 cm in the LS-313 MF15 and Eyhance DIB00V groups,respectively (Figure 1A).The uncorrected distance VAs were 0.2±0.24 and 0.16±0.18 at 5 m, 0.16±0.21 and 0.17±0.18 at 1 m, 0.2±0.24 and 0.22±0.18 at 70 cm, 0.3±0.21 and 0.35±0.21 at 50 cm, and 0.55±0.18 and 0.57±0.24 at 30 cm in the LS-313 MF15 and Eyhance DIB00V groups, respectively(Figure 1B).The uncorrected and distance-corrected VAs did not differ between the two IOL groups at any distance.
Monocular Defocus CurvesVA was measured at each defocus dioptre from +1.5 to -3.0 D in 24 eyes from the LS-313 MF15 group and 35 eyes from the Eyhance DIB00V group three months postoperatively.Monocular defocus curves were generated subsequently (Figure 2A).The curves showed a peak in VA at defocus 0 (5 m), which was the target dioptre,and then a gradual decrease in VA as the defocus progressed positively or negatively.The logMAR VAs were 0.34±0.21 and 0.38±0.2 at a defocus of +1.5 D, -0.05±0.1 and 0.05±0.1 at a defocus of 0, 0.24±0.22 and 0.18±0.17 at a defocus of-1.5 D, and 0.68±0.27 and 0.63±0.27 at a defocus of -3.0 D in the LS-313 MF15 and Eyhance DIB00V groups, respectively.The VAs did not differ between the two IOL groups for any dioptres.
Contrast SensitivityMonocular distance-corrected contrast sensitivity was measured in 24 eyes from the LS-313 MF15 group and 35 eyes from the Eyhance DIB00V group three months postoperatively (Figure 2B).The contrast sensitivities were 1.56±0.23 and 1.65±0.29 at 3 cycles per degree of spatial frequencies, 1.77±0.24 and 1.81±0.27 at 6 cycles per degree,1.45±0.29 and 1.4±0.31 at 12 cycles per degree, and 0.89±0.35 and 0.93±0.3 at 18 cycles per degree in the LS-313 MF15 and Eyhance DIB00V groups, respectively.These results were within the normal range for healthy subjects aged 50-75y.Furthermore, the mean values for contrast sensitivity at any cycle per degree did not differ between the two IOL groups.
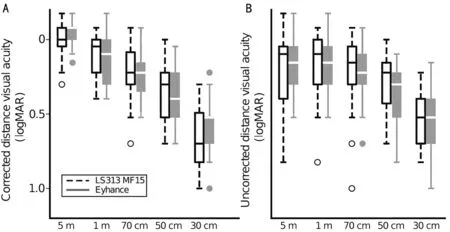
Figure 1 Corrected and uncorrected visual acuity one month postoperatively Corrected distance (A) and uncorrected (B) visual acuity measured in 32 eyes implanted with LS-313 MF15 intraocular lenses and 39 eyes implanted with Eyhance DIB00V lenses.The visual acuities of the two groups do not differ at any distance.
Halo and GlareSubjective halo and glare were evaluated using the Halo & Glare Simulator in patients with the same IOLs implanted in both eyes (eight patients in the LS-313 MF15 group and nine in the Eyhance DIB00V group).The preoperative age, sex, axial length, objective cylinder,keratometric power, and corrected distance VA did not differ between the two groups.Most of the eyes had no subjective symptoms.Halo was not subjective in five patients (62.5%)in the LS-313 MF15 group and seven patients (77.8%) in the Eyhance DIB00V group.Glare was not subjective in sixpatients (75.0%) in the LS-313 MF15 group and eight patients(88.9%) in the Eyhance DIB00V group.The halo size scores were 9.8%±15.5% and 5.6%±16.7% in the (P=0.33), and the glare size scores were 2.3%±4.7% and 1.0%±3.0% (P=0.47) in the LS-313 MF15 and Eyhance DIB00V groups, respectively.
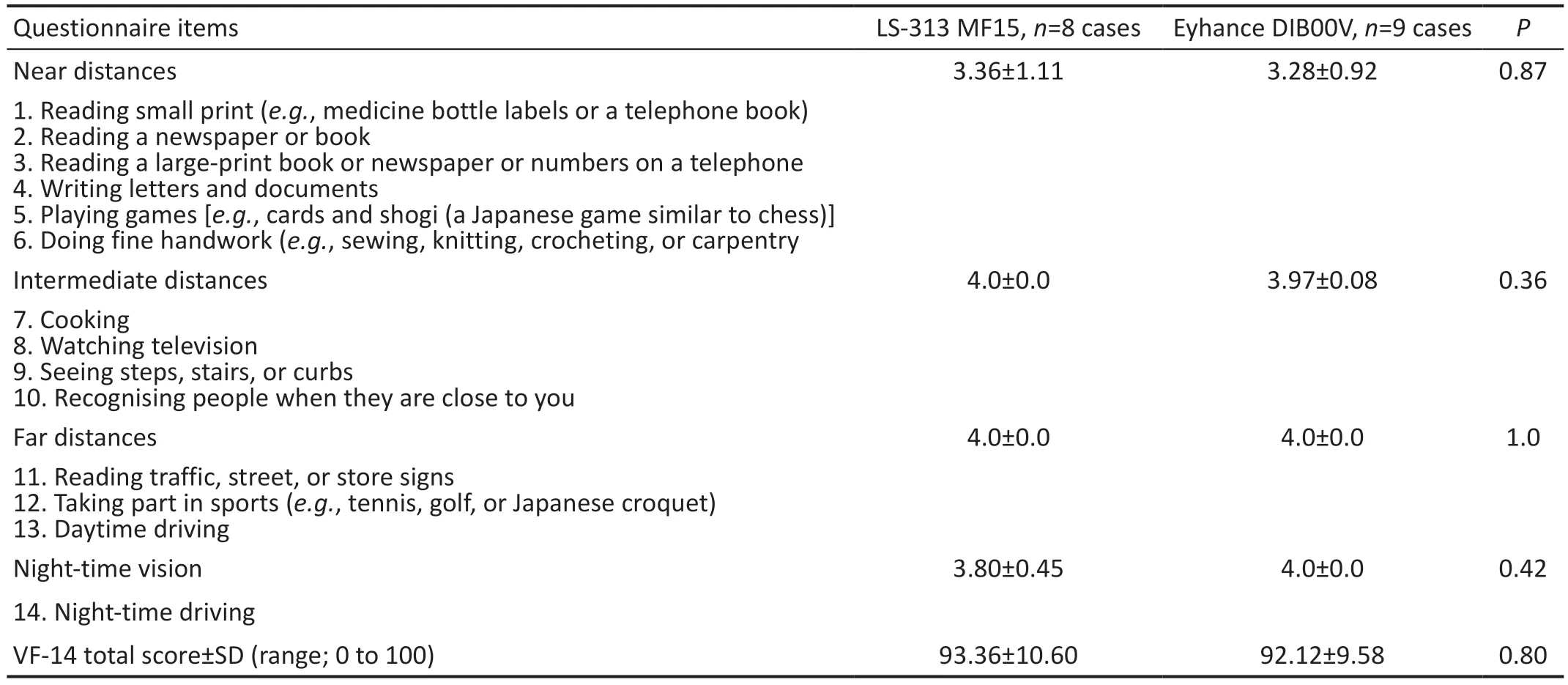
Table 2 Subjective evaluations using the 14-item Visual Function Index Questionnaire (VF-14) three months postoperatively
Subjective SymptomsTable 2 summarises the results of the 14-item Visual Function Index Questionnaire.Eight patients in the LS-313 MF15 group and nine patients in the Eyhance DIB00V group completed the questionnaire to determine subjective satisfaction.The near, intermediate, and far distance vision scores and the night-time scores were comparable between the LS-313 MF15 and Eyhance DIB00V groups (allP>0.05), as were the total scores (93.36±10.60vs92.12±9.58).
DISCUSSION
This study compared two different IOLs: LS313 MF15 and Eyhance DIB00V.The preoperative ophthalmic and general data, distance-corrected and uncorrected VAs one month postoperatively, subjective symptoms based on the 14-item Visual Function Index Questionnaire, monocular defocus curves, contrast sensitivities, and incidence of halos and glare three months postoperatively did not differ between the two IOL groups.Notably, the spherical equivalent one month postoperatively was significantly more myopic in the LS-313 MF15 group than that in the Eyhance DIB00V group; however,this finding was no longer observed after three months.Previous studies investigating the comfort of LS-313 MF15 lenses or Eyhance DIB00V lenses have analysed the surgical outcomes of these IOLs compared with those of classic monofocal IOLs[4,8-13,18].However, the present study had two unique characteristics.First, the LS-313 MF15 and Eyhance DIB00V IOLs were directly compared in this study; second,Eyhance DIB00V lenses, which filter short-wavelength light,were used in this study instead of the Tecnis Eyhance ICB00 lenses, which filter ultraviolet light.
Several reports have compared monofocal IOLs with LS-313 MF15 or Eyhance IOLs, both of which have significantly better distance-corrected and uncorrected VAs at intermediate distances.It was found that their distance-corrected and uncorrected VAs at near and far distances, contrast sensitivities, and halo and glare incidences did not differ from other monofocal IOLs[4,8-13,15].However, a few studies have reported decreasing contrast sensitivity and increasing incidence of halos and glare with the use of LS-313 MF15 or Eyhance DIB00V IOLs compared with the use of other monofocal IOLs[11,13].Therefore, based on these reports, similar surgical outcomes were expected on comparing the LS-313 MF15 and Eyhance DIB00V IOLs despite the differences in their mechanisms (i.e., multifocalvsenhanced monofocal).As predicted, no differences were observed between LS-313 MF15 and Eyhance DIB00V IOLs in terms of the uncorrected and distance-corrected VAs for near to far distances, subjective symptoms, contrast sensitivities, VAs at each defocus dioptre(from +1.5 to -3.0 D),and the incidence of halo and glares.The only significant difference identified between the two IOLs was in the spherical equivalent, which was more significantly myopic in the LS-313 MF15 group than that in the Eyhance DIB00V group one month postoperatively.Previous studies have also reported temporary myopic changes in eyes implanted with LS-313 MF15[19].However, the myopic changes had resolved by three months postoperatively in the present study; thus, these changes were not expected to cause problems with uncorrected distance VA.Although the additional power of LS-313 MF15 was larger than that of Eyhance DIB00V, no significant differences were observed between the intermediate visual acuities of the two IOLs.This finding may be attributed to the significant difference between the IOL targets of the two groups.The IOL targets were based on the manufacturer’s recommendations in this study:the closest value to 0 was selected for LS-313 MF15 and the closest negative value to 0 was selected for Eyhance DIB00V,resulting in a significant difference in the IOL targets.This may have caused an improvement in intermediate VA for Eyhance DIB00V, which has a lower additional power.
Comprehensive ophthalmic examinations did not identify any differences between the LS-313 MF15 and Eyhance DIB00V groups, except for the previously mentioned myopic changes.Therefore, surgeons must select IOLs based on other factors, such as cost, accessibility, and range of IOL power.In Japan, the cost of lenses is nearly the same because of the insurance system; thus, both types of IOLs can be obtained easily.However, the range of IOL power differs between the two lenses: 10-27 D in the LS-313 MF15 IOLs and 6-30 D in the Eyhance DIB00V IOLs.None of the postoperative examination items evaluated in this study differed between the two IOLs.Therefore, the surgeon must determine the type of lens to be used depending on the characteristics of each lens.For example, whether the patient prefers clear lenses and whether they have undergone or are likely to undergo a vitrectomy (LS-313 MF15 lenses are made of hydrophilic acrylic, which carries the risk of calcium deposition in diseases for which vitrectomy is performed).As reported by Wuet al[20],hydrophobic IOLs are associated with a lower risk of posterior capsule opacification than hydrophilic IOLs, especially in patients older than 70y.
Our study has some limitations.First, the sample size was small, and the study population was limited to eyes with no other ophthalmic diseases and non-severe corneal astigmatism.In particular, the incidence of halo and glare and the 14-item Visual Function Index Questionnaire were evaluated only in the patient with the same IOLs implanted bilaterally because of their nature, as these examinations evaluate the patient’s vision in daily life.Thus, the sample size was small and may not be sufficient for statistical evaluation.However, several previous reports comparing LS-313 MF15 or Eyhance DIB00V with monofocal IOLs reported no significant difference in the degree of halo and glare.Based on these results, the lack of significant difference in the degree of halo and glare on directly comparing both IOLs in this study may be considered consistent with the results of this study.Therefore, largescale studies must be conducted in the future to confirm the differences between the surgical outcomes of LS-313 MF15 and Eyhance DIB00V IOLs.Second, this study included a mix of patients with one and both eyes under evaluation, which may have introduced bias.Third, ideally, the surgery should be performed by a single surgeon to reduce the influence of the surgical technique on the outcome.However, in this study, the surgeries were performed by multiple surgeons owing to the nature of the study design; this was considered an influential factor in the results.Fourth, pupil diameter is a factor that may extend the depth of focus, but it was not evaluated in this study and should be considered in the future.Lastly, spherical aberration is also considered an important factor that can affect the depth-of-focus extension and contrast sensitivity.However,spherical aberration was not measured in this study; thus, its influence could not be evaluated.
In conclusion, this study directly compared the LS-313 MF15 and Eyhance DIB00V IOLs through comprehensive ophthalmic examinations, including contrast sensitivity, halo and glare tests, and defocus curves.Both IOLs showed good and comparable surgical outcomes one and three months postoperatively, except for the temporary myopic change with the LS-313 MF15 lenses one month postoperatively.
ACKNOWLEDGEMENTS
We would like to thank Takuya Shiba for the helpful comments and the patients for their participation in this study.
Authors’ contributions:Sugawara K and Ito R collected,analysed, and interpreted the data and drafted the manuscript.Horiguchi H and Katagiri S critically reviewed the study design and drafted the manuscript.Gunji H conceived and supervised the study.Nakano T critically revised the manuscript for intellectual content.All authors have read and approved the final manuscript.
Foundations:Supported by the grant of Japan Society for the Promotion of Science (JSPS) KAKENHI (No.21K09729); a grant from Alcon Japan Ltd., awarded to Horiguchi H.
Conflicts of Interest:Sugawara K,None;Ito R,None;Horiguchi H,None;Mizobuchi K,None;Katagiri S,None;Gunji H,None;Nakano T,None.
 International Journal of Ophthalmology2023年12期
International Journal of Ophthalmology2023年12期
- International Journal of Ophthalmology的其它文章
- Endoscopic transnasal optic canal decompression for pediatric traumatic optic neuropathy with no light perception
- Three siblings with gyrate atrophy of the choroid and retina: a case report
- Glaucoma among Saudi Arabian population: a scoping review
- Visualized analysis of research on myopic traction maculopathy based on CiteSpace
- Different approaches for treating myopic choroidal neovascularization: a network Meta-analysis
- Agreements’ profile of Scheimpflug-based optical biometer with gold standard partial coherence interferometry