
Long-term outcomes of anti-VEGF treatment with 5+PRN regimen for macular edema due to central retinal vein occlusion
2023-10-21 03:11:48YaYeYuMengDengZhenHuangQiaoWeiWuYanNianHuiYanPingSong
Ya Ye, Yu-Meng Deng, Zhen Huang, Qiao-Wei Wu, Yan-Nian Hui, Yan-Ping Song
1The First School of Clinical Medicine, Southern Medical University, Guangzhou 510515, Guangdong Province, China
2Department of Ophthalmology, General Hospital of Central Theater Command, Wuhan 430070, Hubei Province, China
3Department of Ophthalmology, Xijing Hospital, Fourth Military Medical University, Xi’an 710032, Shaanxi Province,China
Abstract
● KEYWORDS: central retinal vein occlusion; macular edema; anti-vascular endothelial growth factor; regimen;laser; dexamethasone implant
INTRODUCTION
Central retinal vein occlusion (CRVO) is the second most common vision-impairing retinal vascular disease in the world.Macular edema (ME) occurs as a major complication of CRVO and results in significant visual loss[1].The standard and first-line therapy for CRVO-ME is intravitreal injection of antivascular endothelial growth factor (VEGF) drugs[2].Several randomized clinical trials (RCTs) have confirmed the safety and efficacy of intravitreal injections of aflibercept monthly for 6mo for CRVO-ME[3-4], including the COPERNICUS[5]and GALILEO[6]studies.The SCORE2[7]study included 362 patients who were randomized 1:1 and received 6 monthly injections of either bevacizumab or aflibercept.The LEAVO[8]study included 436 patients allocated 1:1:1 to the ranibizumab,bevacizumab, and aflibercept groups.All patients received a 4+pro re nata(PRN) regimen and were followed up for 2y.The mean number of injections in the first year ranged from 8.2 to 11.8, and the mean best-corrected visual acuity (BCVA)improved from 12.7 to 18.9 letters at the endpoint.
However, the results of RCTs may not reflect real-world effectiveness, since the actual practices in clinics may differ from the conditions strictly controlled by RCTs.Inadequate or non-standard treatment in clinical practice often leads to unsatisfactory treatment outcomes, requiring additional injections or switching to a different anti-VEGF drug[9-10]or dexamethasone implants (DEX)[11-12]in followup visits.Several retrospective real-world studies[13-15]that used 1+PRN or 3+PRN treatment regimens reported mean numbers of injections in the first year of 3.7 to 7.6, and a mean improvement in visual acuity (VA) of 8.0 to 14.8 letters at month 12, indicating that fewer injections in real clinical practices may result in unsatisfied BCVA improvement.
According to our observations in clinical practice, BCVA or macular structure in some CRVO patients is still unsatisfactory after two or three injections due to the recurrence of ME or persistent fluid cysts, and additional injections are required.Therefore, the aim of the study was to evaluate the clinical outcomes and patterns of the 5+PRN regimen in patients with ME secondary to ischemic CRVO (iCRVO) and non-ischemic CRVO (iCRVO), with a follow-up time exceeding 15mo.
SUBJECTS AND METHORDS
Ethical ApprovalThe current study adhered to the tenets of the Declaration of Helsinki and approved by the Medical Research Ethics Committee and Institutional Review Board of the Hospital, and the registration number of this study in the Chinese Clinical Trial Registry is ChiCTR2000040087.The risks/benefits of intravitreal injection and laser therapy were explained to all patients, and they all provided related written informed consent.
Enrollment of SubjectsThis retrospective study included 27 eyes of 27 patients diagnosed with CRVO-ME by the same ophthalmologist between November 2014 and September 2020.Records were collected for at least five consecutive loading doses of anti-VEGF injections within the study period,and a follow-up exceeded 15mo.Inclusion criteria were as follows: 1) fundus manifestation and fundus fluorescein angiography (FFA) conformed to diagnosis of CRVO; 2)macular thickness >250 μm by spectral-domain optical coherence tomography (OCT) scans at the initial visits;3) ME treated with intravitreal injections of conbercept or ranibizumab.Exclusion criteria included eyes with branch retinal vein occlusion, vitreomacular traction, age-related macular degeneration, glaucoma, associated diabetes,hypertensive or renal retinopathy and that have not previously received surgical treatment or anti-VEGF therapy.
Ophthalmic ExaminationsAt the initial visit, the patient’s medical history, including systemic diseases, was collected through medical interviews.At 1, 2, 3, 4, 5, 6, and 12mo and the final visit, all patients underwent a comprehensive ophthalmic examination, including BCVA with the Snellen chart, which was converted to logarithm of the minimum angle of resolution (logMAR), intraocular pressure (IOP), indirect ophthalmoscopy, slit-lamp biomicroscope anterior segment,fundus examination, and OCT examination.FFA examination was performed on each patient at baseline and at each followup visit, based on the judgment of the ophthalmologists.A non-perfusion area larger than 10 disc areas on the FFA examination was defined as iCRVO.The CRVO subtypes(ischemic and non-ischemic) were determined by two masked retinal specialists.The deadline observation was March 2022.
Anti-Vascular Endothelial Growth Factor TreatmentPatients received either ranibizumab (0.5 mg/0.05 mL) or conbercept (0.5 mg/0.05 mL) monotherapy or underwent a switch between the two drugs.All 27 eyes received intravitreal injections every four weeks for five consecutive times.After the loading treatment, patients received an additional injection if they met any of the following criteria: 1) BCVA decrease of ≥0.1 logMAR; 2) central retinal thickness (CRT) increase of ≥50 μm; or 3) BCVA decrease due to ME recurrence or persistent fluid sac cavity in the neuroepithelium.Drug switching between anti-VEGF may apply when ME persists or reappears after more than 2 consecutive injections of conbercept or ranibizumab.
Intravitreal Dexamethasone ImplantsDEX (Ozurdex Allergan Inc., Irvine, CA, USA) is the only glucocorticoid drug approved by the US Food and Drug Administration and the European Union for treating ME associated with retinal vein occlusion (RVO-ME).Multicenter clinical trials have shown that intravitreal injection of Ozurdex alone is safe and effective for RVO-ME[16-17]and it can also be used for RVO-ME patients with poor anti-VEGF treatment efficacy[18-19].Thus, Ozurdex was applied to CRVO-ME patients who showed persistent or recurrent ME, despite repeated anti-VEGF therapy in this study.
Laser TreatmentThe Novus Varia multi-wavelength laser(Lumenis, USA) was used for panretinal photocoagulation(PRP) or treatment on partial non-perfusion areas in CRVOME patients.Laser irradiation was performed 500 μm away from the fovea.PRP was performed outside the superior andinferior vascular arch, 2500 μm from the fovea on the temporal side and 500 μm from the optic disc edge on the nasal side.Laser parameters were as follows: the spot diameter was 200-300 μm, the power output was 200-500 mW, the exposure time was 200ms, and the reaction was grade II-III heavy white.The range was from the outer spot of the superior and inferior temporal vascular arch to the serrated margin, and the upper,lower, and nasal edges of the disc.The spot spacing was one spot diameter.
Efficacy CriteriaIn reference to the European Society of Retinal Diseases RVO Clinical Guidelines[2], the efficacy criteria were defined in our study as follows: 1) Cured: CRT is in the normal range.Visual acuity was normal or restored to pre-onset VA; 2) Apparent effective: CRT decreased by more than 50% compared with the baseline; BCVA increased by 20 letters or more; 3) Effective: CRT decreased by <50%and ≥10% compared with baseline; BCVA increased by 10 letters or more; and 4) Ineffective: CRT remained unchanged or continued to worsen; BCVA did not change or decreased;complications such as neovascular glaucoma occurred.
Statistical AnalysisAll statistical analyses were carried out using SPSS statistical software version 25.0 (IBM, New York,USA).Data are presented as mean±standard deviation (SD).The logMAR and CRT parameters before and after treatment were compared using paired samplet-tests.Differences between treatment groups were compared using independent samplet-tests.A Chi-square test was used to compare the rates of VA improvement among the different groups at different periods.AP-value of <0.05 was considered statistically significant.
RESULTS
Demographic and Clinical CharacteristicsThis study enrolled 27 eyes diagnosed with CRVO-ME.Table 1 shows the baseline characteristics of the included patients with different types of CRVO before anti-VEGF treatment.The patient sample comprised 13 males and 14 females, with a mean age of 59.4±15.1y.The affected eyes included 12 left eyes and 15 right eyes.The mean follow-up period was 24.7±8.8mo(range: 15-42mo).The patients included 15 patients with noniCRVO and 12 with iCRVO.The mean baseline BCVA was 0.84±0.39 logMAR for the non-iCRVO group and 1.28±0.66 logMAR for the iCRVO group.The mean baseline CRT was 638.9±247.3 μm for the non-iCRVO group and 761.2±295.2 μm for the iCRVO group.
Visual and Anatomical OutcomesAfter anti-VEGF treatment, the mean baseline BCVA (1.04±0.56 logMAR) of all included patients steadily improved and peaked to 0.59±0.36 logMAR at the final visit (P=0.038; Figure 1).BCVA improved throughout the observation time in both the non-iCRVO and iCRVO groups, but there was no statistical significance in both groups (P=0.197 and 0.33, respectively; Figure 1).The mean CRT at different time points for 27 patients is shown in Figure 2.CRT significantly decreased throughout the observation time in all included patients and both non-iCRVO and iCRVO groups (P<0.001), and reach to the lowest value at the last visit.Statistical differences at each visit time compared to the baseline for BCVA and CRT are shown in Figure 2.
Efficiency of BCVA and CRT ImprovementAfter the first injection, the apparent effective rate for all included patients was 22.22% for BCVA and 37.04% for CRT.After five consecutive injections, the apparent efficiency andtotal effective rate for BCVA were 48.15% and 62.96%, respectively(Table 2).Moreover, the total effective rates for BCVA and CRT increased with the number of injections, reaching to 74.08% and 100% respectively at the last visit.
Therapeutic InterventionTwelve iCRVO eyes finished PRP treatment before and after the first injection (Figure 3).Five non-iCRVO eyes received local laser therapy targeting nonperfusion areas at 3, 6, and 12mo (Table 2).Four and five eyes received intravitreal injections of Ozurdex in the non-iCRVOgroup and the iCRVO group, respectively.Table 3 illustrates the number of injections in each group at the 12-month and final visits.The median number of injections in the total CRVO population was 9.0±2.4 and 14.9±8.1 at the 12-month and final visits, respectively.The eyes received an average of 14.4±8.8 injections in the non-iCRVO group and 15.5±7.5 injections the iCRVO group at the final visit.After five consecutive injections, the injection intervals were 1.32±1.03 and 1.41±0.36mo in the non-iCRVO group and the iCRVO group, respectively (P>0.10).In the iCRVO group, the number of the eyes received 6-10 injections and ≥21 injections was larger than that in the non-CRVO group.Table 4 shows the overview of 27 patients treatment, 6 and 3 eyes treated with anti-VEGF drugs switched therapy in the non-iCRVO group(Figure 4) and the iCRVO group, respectively, of which 1 eye had no change in CRT after switching from conbercept to ranibizumab, and 1 eye had no change in CRT after switching from ranibizumab to conbecept, but the CRT all improved after DEX injection, and the CRT height in 1 eye did not return to normal at the observation deadline.
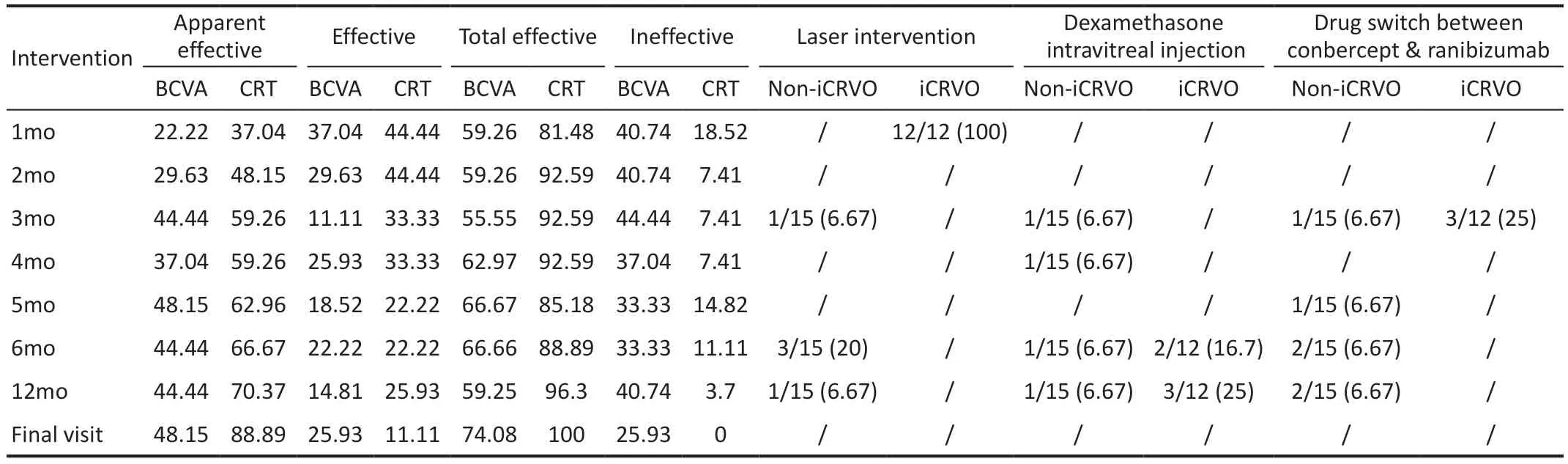
Table 2 Efficacy rate (%) and therapeutic intervention

Figure 1 BCVA at each observation point during the follow up time A: BCVA in total; B: BCVA in non-iCRVO group; C: BCVA in iCRVO group.BCVA: Best-corrected visual acuity; CRVO: Central retinal vein occlusion; iCRVO: Ischemic central retinal vein occlusion.aP<0.05.

Figure 2 CRT at each observation point during follow up time A:CRT in total; B: CRT in non-iCRVO group; C: CRT in iCRVO group.CRT: Central retinal thickness; iCRVO: Ischemic central retinal vein occlusion.aP<0.05.

Figure 3 Changes in ME after treatment of a patient with iCRVO A 30-year-old male patient diagnosed with iCRVO-ME in the right eye, with baseline BCVA of 1.0 logMAR and CRT 533 μm, received 26 injections of conbercept during a 34mo follow-up period, and received PRP within 1mo.The patient had a delayed response to anti-VEGF treatment.After 5 consecutive injections, the macular edema appeared.BCVA was 1.0 logMAR, and the CRT was 235 μm at the final visit; no adverse event occurred during the follow-up period.A: Tortuous and dilated retinal veins with extensive flaky retinal hemorrhage; B-C: Large areas of nonperfusion before treatment (yellow arrows); D: Fundus color photograph of this patient who underwent panretinal photocoagulation; E-F: A laser photocoagulation spot and posterior polar retinal capillary fluorescence leakage.After treatment, the ME was gradually absorbed and the CRT decreased to normal (G: 533 μm, baseline; H: 510 μm, 1mo; I: 395 μm,2mo; J: 497 μm, 3mo; K: 312 μm, 4mo; L: 327 μm, 5mo; M: 227 μm; 6mo; N: 211 μm,12mo; O: 235 μm; 34mo).ME: Macular edema; iCRVO:Ischemic central retinal vein occlusion; CRT: Central retinal thickness; BCVA: Best-corrected visual acuity; PRP: Panretinal photocoagulation;VEGF: Vascular endothelial growth factor.

Table 3 Anti-VEGF therapy status for different types of CRVO during the observation period

Table 4 Overview of 27 patients treatment
Safety ProfileTwo eyes (7.4%) developed severe lens opacities that affected the BCVA, and one eye (3.7%)developed macular epiretinal membrane.Mild adverse events included mild subconjunctival hemorrhage, vitreous opacity,and temporarily elevated IOP.The above adverse events returned to normal after observation or drug treatment.
DISCUSSION
Unlike the traditional 3+PRN regimen for CRVO-ME, we screened 27 patients who received the 5+PRN regimen and summarized their baseline characteristics, clinical treatment strategies, and efficacy.These eyes had worse mean baseline BCVA (1.04±0.56 logMAR) and higher mean CRT(693.2±271.3 μm).The present study showed that treatment of ME secondary to non-iCRVO and iCRVO with a 5+PRN anti-VEGF regimen combined with Ozurdex and laser treatment achieved significant improvement in BCVA and CRT at the final visit.During the five consecutive anti-VEGF treatments,the total effective rate for BCVA and CRT declined mildly at 3 and 5mo, respectively.However, the total effective rate for BCVA and CRT increased at 6mo with continuous treatment,suggesting the inevitability and effectiveness of 5+PRN treatment in clinical practice.The mean BCVA improved significantly from 1.04 at baseline to 0.74 (P>0.1) at the 6-month visit and 0.59 (P<0.01) at the final visit for the entire CRVO population, corresponding to an increase of 13 ETDRS letters at the 6-month visit and 21 ETDRS letters at the final visit.Compared to other anti-VEGF drugs, patients injected with aflibercept gained a mean of 18.0 letters and 17.3 letters at 6mo in the COPERNICUS[5]study and the GALILEO[6]study, respectively, but our study showed a lower level of visual improvement.The reason may be the smaller number of patients in our study and the lower baseline BCVA compared to these two studies.Moreover, 9 out of 12 eyes in the iCRVO group had baseline BCVA lower than 1.0 logMAR.

Figure 4 Changes in ME after treatment in a patient with non-iCRVO A 64-year-old female patient, with a baseline BCVA of 0.4 logMAR and CRT 470 μm, diagnosed with non-iCRVO-ME in the left eye, received 15 anti-VEGF injections during a 19mo follow-up period.CRT decreased gradually after 4 consecutive injections, but increased at 5mo, BCVA was 0.4 logMAR and CRT was 147 μm at the final visit; no adverse event occurred during the follow-up period.A: Tortuous and dilated retinal veins with extensive flaky retinal hemorrhage; B-C: Retinal vein wall fluorescence staining, retinal telangiectasia at the posterior pole, fluorescence leakage, and spreading to the macular area.After treatment,the ME was gradually absorbed and the CRT decreased to normal (D: 470 μm, baseline; E: 310 μm, 1mo; F: 146 μm, 2mo; G: 267 μm, 3mo; H:685 μm, 4mo; I: 233 μm, 5mo; J: 167 μm, 6mo; K: 275 μm, 12mo; L: 147 μm, 19mo).ME: Macular edema; iCRVO: Ischemic central retinal vein occlusion; CRT: Central retinal thickness; BCVA: Best-corrected visual acuity; VEGF: Vascular endothelial growth factor.
Therefore, it is important to highlight the results of our iCRVO group, given that there have recently been a few studies about iCRVO-ME.Some studies have revealed that anti-VEGF drugs are effective for iCRVO eyes.Pielenet al[20]found that BCVA gain over six months in ranibizumab-treated RVO patients is not affected by ischemia, and is associated with less development of new ischemia during the first 6mo, but longterm observations are still lacking.Spooneret al[21]analyzed the 8-year outcomes of eyes with ischemic and non-ischemic RVO following treatment with a 3+PRN anti-VEGF regimen.BCVA (0.88±0.7 logMAR) and CRT (714.6±275.5 μm)improved significantly in eyes with iCRVO at 8y.Mean BCVA improved by 18 letters at 1y and 16 letters at 8y.In the present study, the BCVA of eyes in the iCRVO group gradually improved, with an improvement equivalent to 13 letters at 1y and 21 letters at the final time.CRT also gradually dropped from the baseline of 761.2±295.2 to 238.3±70.3 µm.We should mention that the baseline VA was lower and CRT was higher in the iCRVO group than in the above study,but a smaller sample size was involved; thus, reasonable comparisons could not be made.
Notably, laser treatment plays an important role in the treatment of iCRVO-ME.Each iCRVO patient in this study underwent PRP treatment.Five eyes (33.3%) in the noniCRVO group underwent local photocoagulation targeting the ischemic areas.Liuet al[22]showed that conbercept with retinal photocoagulation could effectively improve VA and reduce CRT caused by iCRVO-ME.A systematic review[23]of the efficacy of PRP in ischemic CRVO indicated that laser therapy achieved better outcomes in neovascularization of the retina,improvement in the visual field, ME, and macular thickness.Our results suggest that significant vision improvements could be achieved over longer periods of treatment, despite the more severe baseline conditions.This is an important finding,especially for iCRVO patients.
During the average follow-up of 24.7mo, the mean number of injections in the first year was 9.0, while a previous retrospective study[13]administered 7.6 anti-VEGF injections in the first year using a 3+PRN regimen.However, the SCORE2 Report 10 study[24](a Phase III prospective, multicenter,randomized clinical trial) reported 9.7-10.8 injections in the first year, and a mean of 4.7 injections in the aflibercept group and 5.5 in the bevacizumab group during months 12 to 24.These previous findings are comparable to the average number of 14.9 injections at the final visit in the present study.There was no significant difference in the number of injections between the two groups at 12mo (8.8vs9.1) and at the final visit time (15.5vs14.4).In total, 25% of eyes in the iCRVO group received ≥21 injections, nearly twice as many as in the non-iCRVO group, which may suggest that iCRVO patients need more injections.
In this study, 9 eyes underwent drug switching.When ME persisted or reappeared after more than 2 consecutive injections of conbercept or ranibizumab, the switching between the two drugs was performed, 7 eyes switched from initial ranibizumab injection to subsequent conbercept injection, 2 eyes switched from initial conbercept injection to subsequent ranibizumab injection.The conversion from ranibizumab to conbercept was more common, and the improvement rate of CRT (85.7%) is significantly improved.It has been reported that patients with refractory or continuous CRVO-ME who had received at least three consecutive intravitreal injections of bevacizumab or ranizumab had improved macular thickness and prolonged injection interval after switching to conbercept injection[10].As a fusion protein, conbercept bonded to not only VEGF-A but also VEGF-B and placental growth factor, conbercept contains one additional binding domain of VEGF receptor 2 which enhances the affinity.It was believed that the molecular characteristics of the higher affinity of conbercept to VEGF-A might contribute to the superior treatment effect[25].
Overall, our primary findings suggest that the 5+PRN anti-VEGF regimen was safe and effective for both iCRVO and non-ischemic CRVO in a real-world clinical situation,especially in the iCRVO group.CRVO eyes with lower baseline BCVA and higher baseline CRT may require more anti-VEGF injections and adjuvant therapy, suggesting that continuing long-term anti-VEGF therapy may be necessary to improve and maintain visual and anatomic outcomes.
This study had several limitations, including a related small study population and retrospective design, and the absence of a control group.Several confounding factors were involved, such as glucocorticoid intravitreal injections and laser treatment.The integrity of the outer foveal layers is not reported, and therefore the interpretation of the VA outcome is lacking these relevant data.Future studies with a larger population and a standard treatment protocol and control group will be required to strengthen the statistical validity of the findings of this study,the relationship between OCT characteristics as a predictor and BCVA and CRT in patients with non-iCRVO and iCRVO will be observed.
ACKNOWLEDGEMENTS
Conflicts of Interest: Ye Y,None;Deng YM,None;Huang Z,None;Wu QW,None;Hui YN,None;Song YP,None.
 International Journal of Ophthalmology2023年10期
International Journal of Ophthalmology2023年10期
- International Journal of Ophthalmology的其它文章
- A novel pathogenic splicing mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa verified by minigene splicing assay
- Vault predicting after implantable collamer lens implantation using random forest network based on different features in ultrasound biomicroscopy images
- Multiple evanescent white dot syndrome relapse following BNT162b2 mRNA COVID-19 vaccination
- Acute micro-macular hole associating with extensive intraoperative rotation of implantable collamer lens without ophthalmic viscosurgical device assistance: a case report
- Effectiveness of conjunctival bleb scarring by knockdown of heat shock protein 47 in rat model
- Effect of miR-27b-3p and Nrf2 in human retinal pigment epithelial cell induced by high-glucose