
Primary malignant melanoma of the esophagus combined with squamous cell carcinoma: A case report
2023-04-02 10:49:10MeiLinZhuLingYunWangXueQinBaiChenWuXiangYuLiu
Mei-Lin Zhu,Ling-Yun Wang,Xue-Qin Bai,Chen Wu,Xiang-Yu Liu
Mei-Lin Zhu,Department of Geriatrics,Jining No.1 People's Hospital,Jining 272000,Sahndong Province,China
Ling-Yun Wang,Chen Wu,Xiang-Yu Liu,Department of Gastroenterology,Jining No.1 People's Hospital,Jining 272000,Shandong Province,China
Xue-Qin Bai,Department of Pathology,Jining No.1 People's Hospital,Jining 272000,Sahndong Province,China
Chen Wu,College of Clinical Medicine,Jining Medical University,Jining 272013,Shandong Province,China
Abstract BACKGROUND Primary malignant melanoma of the esophagus is a rare malignant tumor of the esophagus,and its combination with squamous cell carcinoma is also rare.Here,we report the diagnosis and treatment of a case of primary esophageal malignant melanoma combined with squamous cell carcinoma.CASE SUMMARY A middle-aged man underwent gastroscopy for dysphagia.Gastroscopy revealed multiple bulging esophageal lesions,and after pathologic and immunohistochemical analyses,the patient was finally diagnosed with "malignant melanoma with squamous cell carcinoma".This patient received comprehensive treatment.After one year of follow-up,the patient was in good condition,and the esophageal lesions seen on gastroscopy were controlled,but unfortunately,liver metastasis occurred.CONCLUSION When multiple esophageal lesions are present,the possibility of multiple pathological sources should be considered.This patient was diagnosed with primary esophageal malignant melanoma combined with squamous cell carcinoma.
Key Words: Squamous cell carcinoma;Primary malignant melanoma;Endoscopy;Case report
lNTRODUCTlON
Among malignant tumors,esophageal cancer currently ranks seventh worldwide in terms of incidence and sixth in terms of mortality rate.More than 90% of esophageal cancers in China are of the esophageal squamous cell carcinoma pathological type.In contrast,melanoma accounts for only 0.1% of all esophageal malignancies[1].Although both types of malignant tumors can occur in the esophagus,no case of esophageal malignant melanoma combined with squamous cell carcinoma has been reported.Here,a case of primary esophageal malignant melanoma combined with squamous cell carcinoma is reported.
CASE PRESENTATlON
Chief complaints
A 53-year-old man underwent esophagogastroduodenoscopy for dysphagia.
History of present illness
The patient had a history of progressive dysphagia for more than 1 mo.
History of past illness
The patient had no past medical problems.
Personal and family history
He smoked 30 cigarettes per day for 30 years but only rare drinks alcohol.He is a farmer by profession and has other bad habits.No significant personal or family history was noted.
Physical examination
He was 1.76 m tall,weighs 72 Kg and has a BMI of 23.2 Kg/m2.During physical examination,no specific physical signs were found.
Laboratory examinations
Routine blood,liver function,renal function and prothrombin tests were normal.Alpha-fetoprotein,carcinoembryonic antigen,carbohydrate antigen 19-9,carbohydrate antigen 724,neuron-specific enolase and cytokeratin-19-fragment were normal.
Imaging examinations
Chest and enhanced abdominal computed tomography (CT) indicated upper and lower esophageal wall thickening,and the lumen was narrow.Enhanced scanning showed the enhancement of the wall.The mediastinal lymph nodes were enlarged.Multiple small nodules were seen in both lungs,and emphysema,liver cysts,and cholecystitis were also observed (Figure 1).
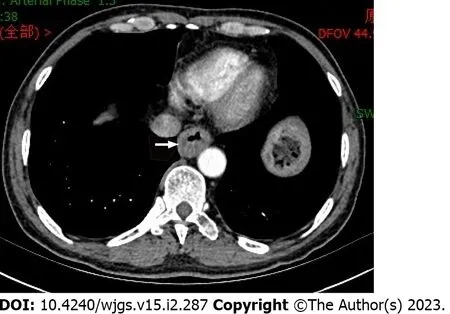
Figure 1 Computed tomography indicates thickening of the esophageal wall.
Gastroscopy observation showed irregular hyperplasia at 23-27 cm from the incisor,with no melanin deposition;hemispherical bulges at 29 cm and 32 cm from the incisor;and irregular hyperplasia at 39-43 cm from the incisor,indicating ulcers with a small amount of melanin deposition.Biopsies were performed at 23-27 cm,32 cm,and 39-43 cm (Figure 2).
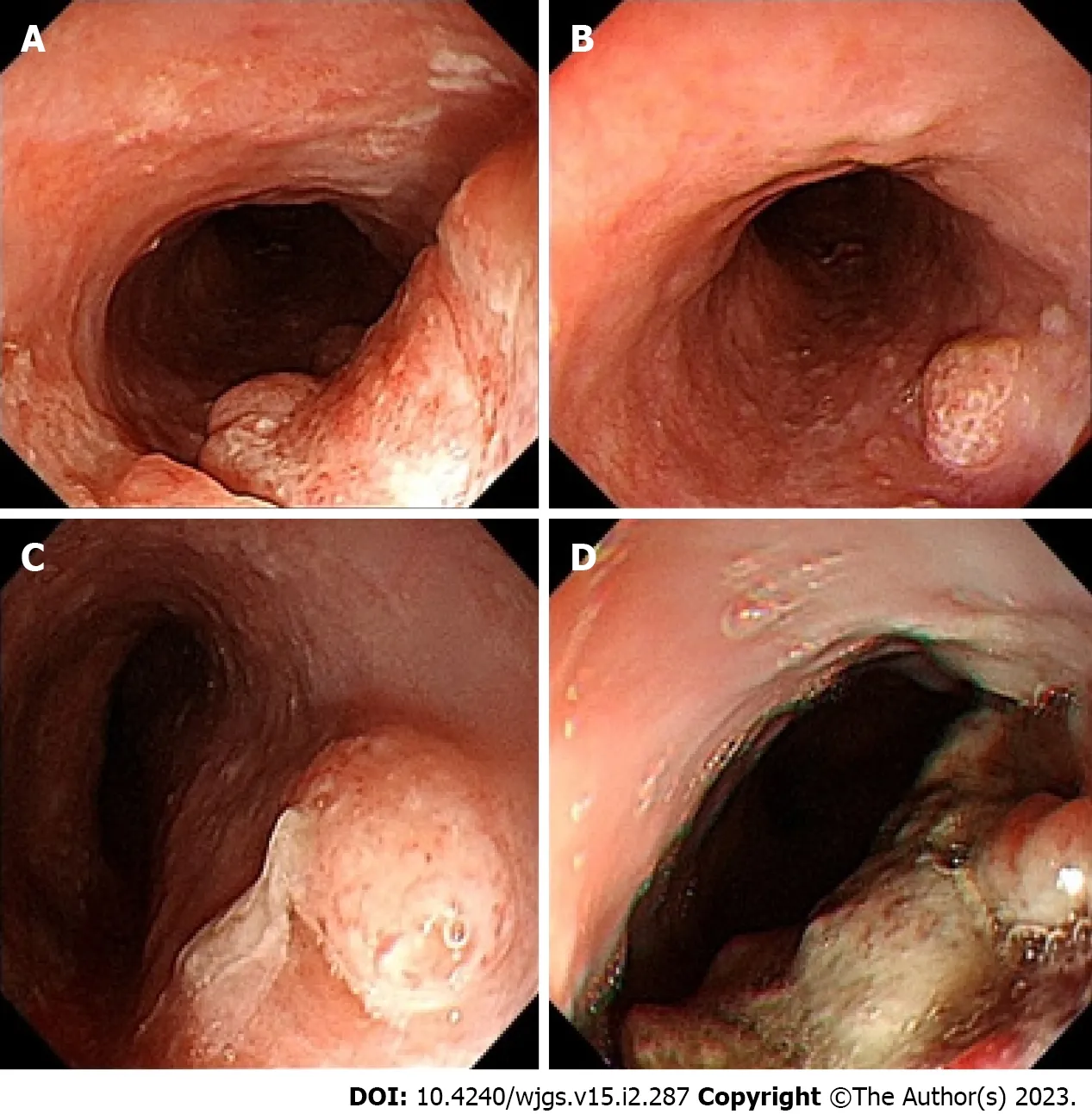
Figure 2 Gastroscopy suggested multiple lesions of the esophagus.
Pathologic analysis indicated malignant melanoma (23-27 cm from the incisor,39-43 cm from the incisor) combined with squamous cell carcinoma (23-27 cm from the incisor) and solitary squamous cell carcinoma (32 cm from the incisor).Immunohistochemistry showed the following: Vimentin(+),HMB45(+),Melan-A(+),S-100(focus+);squamous cell carcinoma CK5/6(+),P40(+),P63(+),LCK(+),CD56(-),CgA(-),and Syn(-);and Ki-67(+) was approximately 30% (Figure 3).
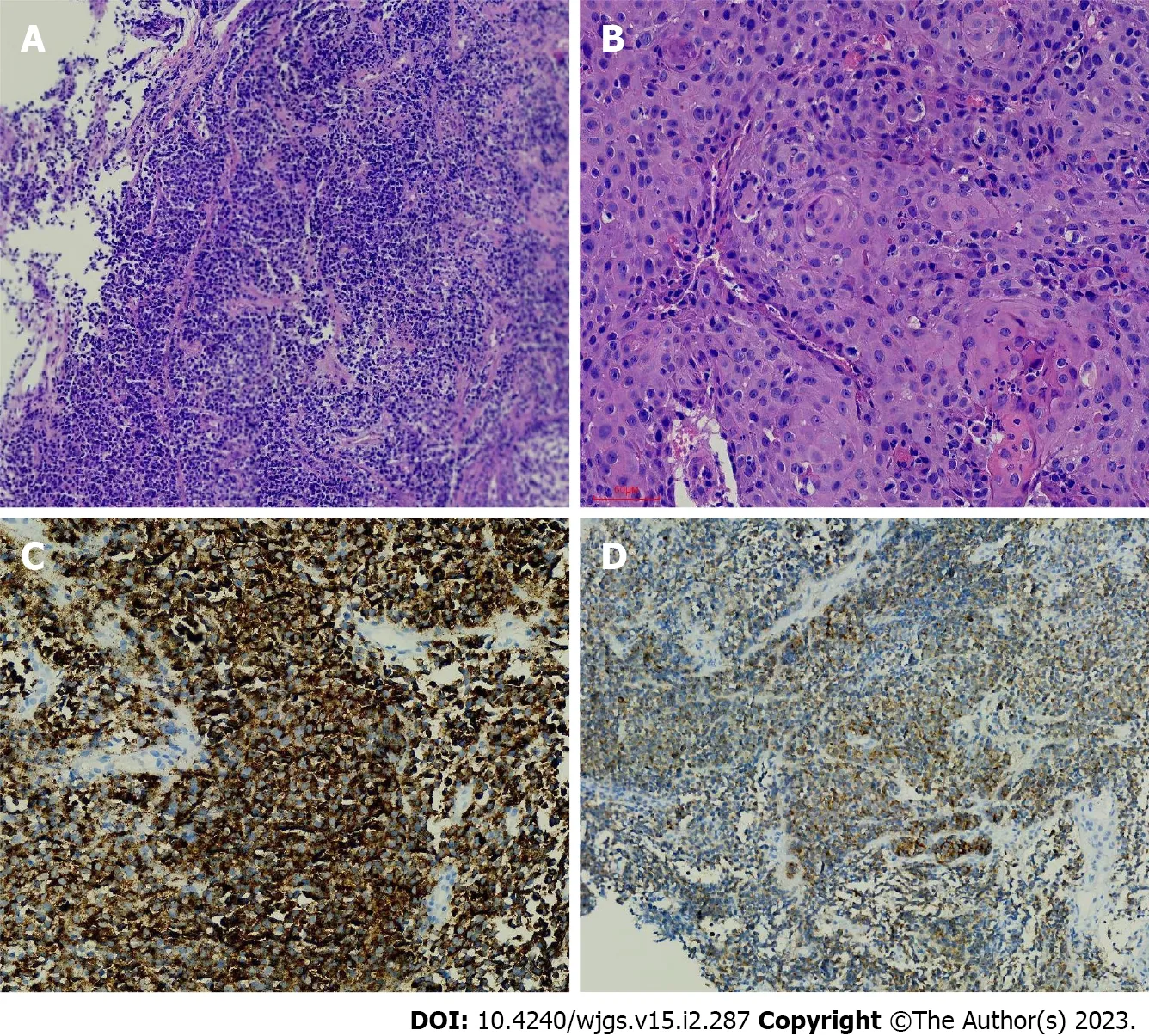
Figure 3 Endoscopic biopsy.
Upper gastrointestinal imaging revealed irregular filling defects approximately 4.5 cm and 5.7 cm in length in the upper and lower sections,respectively,which were accompanied by tube wall stiffness,poor expansion,restricted passage of contrast agent,and disruption of the continuity of the mucosa (Figure 4).
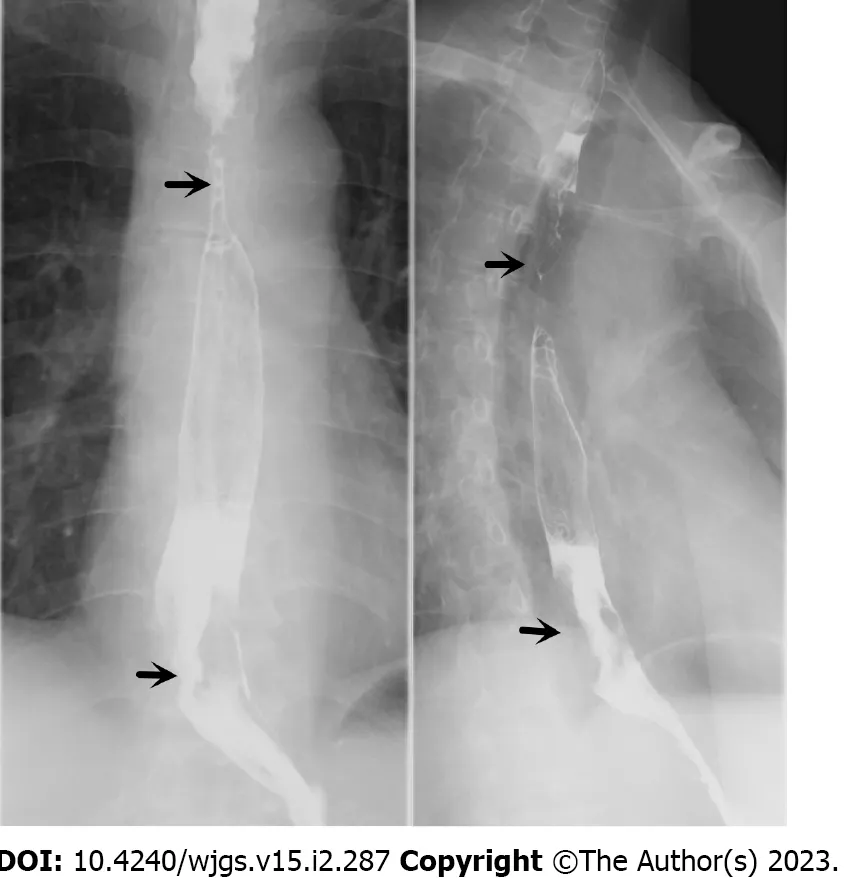
Figure 4 Esophageal barium swallow (the arrow indicates the location of the lesion).
Positron emission tomography/computed tomography (PET/CT) showed thickening of the upper and lower thoracic walls of the esophagus,an abnormal increase in fluorodeoxyglucose (FDG) metabolism,and multiple enlarged lymph nodes in the mediastinum and right axilla.Multiple small nodules were observed in both lungs,and the FDG metabolism was increased.
No metastatic lesions were observed on brain magnetic resonance imaging (MRI).
The microsatellite instability results were MSS.Programmed death ligand-1 immunohistochemistry 22C3: The tumour proportion score results were 1%-2% (Figure 5).

Figure 5 Programmed death ligand-1 immunohistochemistry 22C3: The tumour proportion score results were 1%-2%.
FlNAL DlAGNOSlS
The final diagnosis was esophageal malignant melanoma,esophageal squamous cell carcinoma (stage IV),bilateral lung metastases,and metastases in the mediastinal lymph nodes and right axillary lymph nodes.
TREATMENT
The patient was first treated with 1 cycle of 200-mg camrelizumab,followed by 2 cycles of 300-mg nabpaclitaxel.Later,the patient was administered local radiotherapy,which was terminated because the patient could not tolerate it.Subsequently,he was given 2 cycles of 200-mg camrelizumab and 300-mg nab-paclitaxel.
OUTCOME AND FOLLOW-UP
The patient underwent another gastroscopy six months later,and no obvious space-occupying lesion was observed in the esophagus,while only a small amount of melanin deposition was seen (Figure 6).Regrettably,both enhanced CT and enhanced MRI of the patient's abdomen suggested liver metastasis.It is recommended that patients continue treatment with camrelizumab combined with apatinib.The current case has been followed-up for approximately 1 year,and he has not experienced dysphagia.

Figure 6 Gastroscopy review.
DlSCUSSlON
Primary malignant melanoma of the esophagus (PMME) is a rare disease that accounts for 0.5% of all nonskin melanomas[2].Primary melanin-free melanoma is also extremely rare,with slightly more than 20 cases reported thus far[3],and combined esophageal squamous cell carcinoma is even rarer.
The average age of patients with PMME is 60.5 years,and the incidence rate is higher in male patients than in female patients,with a ratio of 2:1[4,5].The degree of PMME malignancy is high and is associated with a poor prognosis;PMME has a median survival rate of 18.1 mo and a 5-year survival rate of less than 10%[6].
The clinical manifestations of PMME are similar to those of esophageal squamous cell carcinoma,and most patients experience the following symptoms: Dysphagia,poststernal pain,and weight loss.Hematemesis and melena are rare.Typical PMME on endoscopy is a lobular or polyp-like tumor with clear boundaries and pigmentation.More than 90% of PMME lesions are located in the distal 2/3 of the esophagus[7].Approximately 10% to 25% of PMME cases have lesions that are different colors,including purple,brown,and white,depending on the amount of melanin[8,9].Some tumors are composed of melanin-free cells,and the identification of other tumors by endoscopy is difficult.The pathological manifestations of primary malignant melanoma in the esophagus can represent the superficial spreading type or a nodule-like growth pattern,and a distinct Peyer’s patch-like or frecklelike melanocyte nest invasion is observed in adjacent squamous epithelium.Tumor cells are primarily composed of epithelial-like mole-like cells,which are round,oval,polygonal,or shuttle shaped and have large nuclei and large,clear nucleoli.Base film samples are dyed to show thick-walled blood vessels and tubes,which are significant features of melanoma[10].HMB-45,S-100,vimentin,and melanoma-specific antigen (Melan-A) are specific to this diagnosis[11].
PMME mainly occurs through hematogenous metastasis and lymphatic metastasis,and common sites of metastases include the liver (31%),mediastinum (29%),lung (18%),and brain (13%)[12].Whether mediastinal invasion,lymphadenopathy,and distant metastasis are present can be determined through chest and abdominal CT,which can be used to show and determine the stages of lesions.PET-CT plays an important role in the diagnosis of metastatic lesions.
Esophageal malignant melanoma has no specific treatment,and complete surgical removal of lesions is preferred,along with lymph node clearing.Four to six cycles of temozolomide/dacarbazine (DTIC)-based auxiliary chemotherapy are recommended.Radiation therapy is also a possibility.DTIC is the “gold standard” for the medical treatment of advanced melanoma,but its overall efficacy is poor.For targeted therapy,ipilimumab can be used to treat advanced melanoma.Anti-PD-1 and anti-CTLA-4 drugs and IL-2 are FDA-approved immunotherapy drugs that result in significant survival benefits in patients with advanced skin melanoma,but their effects on esophageal malignant melanoma require further investigation[13-15].
Esophageal squamous cell carcinoma is the most common malignant tumor of the esophagus.Patients are located in cities in China with a high incidence of esophageal cancer[16,17],which is mainly associated with diet and lifestyle habits.Radical surgery is the main approach for treating esophageal squamous cell carcinoma.PD-1 inhibitors are currently the first-line drugs for advanced melanoma and have been shown to be effective in treating squamous cell carcinoma of the esophagus[18].Although radiotherapy and chemotherapy are not sensitive to malignant melanoma of the esophagus,the patient was treated with nab-paclitaxel in combination with squamous cell carcinoma of the esophagus and 40 Gy/20 F radiotherapy to the esophageal lesion and mediastinal lymph node area.Overall,our treatment was effective.
CONCLUSlON
In this case,many lesions indicative of esophageal disease were found by gastroscopy.The lesions contained no melanin on their surfaces and were thus unsuitable for endoscopy-based diagnosis and identification.Through pathology and immunohistochemistry,esophageal malignant melanoma combined with esophageal squamous cell carcinoma was diagnosed.This case demonstrated that multiple lesions in the same location can represent different pathologies.
We report a very rare case of primary malignant melanoma of the oesophagus combined with squamous cell carcinoma.Although we do not have much experience in treating this disease,the patient's oesophageal lesions were well controlled through aggressive treatment.We hope this will provide an insight into the diagnosis and treatment of this type of disease.
FOOTNOTES
Author contributions: Zhu ML and Wang LY contributed equally to this work;Zhu ML,Liu XY,Wang LY designed the research report;Bai XQ provided pathological diagnosis and pictures,Zhu ML and Wu C analyzed the data and wrote the manuscript;Wang LY and Liu XY guided and reviewed this article;All authors have read and approved the final manuscript.
lnformed consent statement:Informed written consent was obtained from the patients for publication of this report and any accompanying images.
Conflict-of-interest statement:All the authors declare that they have no conflict of interest to report.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number: Mei-Lin Zhu 0000-0003-3830-5494;Ling-Yun Wang 0000-0003-4514-7498;Xue-Qin Bai 0000-0003-0448-4906;Chen Wu 0000-0003-1352-8931;Xiang-Yu Liu 0000-0003-4702-976X.
S-Editor: Liu JH
L-Editor: A
P-Editor: Liu JH
 World Journal of Gastrointestinal Surgery2023年2期
World Journal of Gastrointestinal Surgery2023年2期
- World Journal of Gastrointestinal Surgery的其它文章
- Fecal microbiota transplantation as potential first-line treatment for patients with Clostridioides difficile infection and prior appendectomy
- Mesh erosion into the colon following repair of parastomal hernia: A case report
- Does size matter for resection of giant versus non-giant hepatocellular carcinoma? A meta-analysis
- Hypophosphatemia as a prognostic tool for post-hepatectomy liver failure: A systematic review
- Hepatobiliary manifestations following two-stages elective laparoscopic restorative proctocolectomy for patients with ulcerative colitis: A prospective observational study
- Efficacy and safety of preoperative immunotherapy in patients with mismatch repair-deficient or microsatellite instability-high gastrointestinal malignancies