
The effect of perirenal fat stranding on infectious complications after ureterorenoscopy in patients with ureteral calculi
2022-09-20 03:30:16ErhnDemirelliErnredenCemilByrktrAlptekinTosunUrlOuz
Asian Journal of Urology 2022年3期
Erhn Demirelli *,Ern reden Cemil Byrktr ,Alptekin Tosun ,Url Ouz
a Giresun University,Faculty of Medicine,Department of Urology,Giresun,Turkey
b Ministry of Health,Kayseri City Hospital,Department of Urology,Kayseri,Turkey
c Giresun University,Faculty of Medicine,Department of Radiology,Giresun,Turkey
KEYWORDS Perirenal fat stranding;Infective complications;Ureterorenoscopy;Ureteral stones;Double-J stent
Abstract Objective:Perirenal fat stranding(PFS)is linear areas of soft-tissue attenuation in the perirenal space on non-contrast computed tomography.The present study aimed to investigate whether PFS is associated with infectious complications after ureterorenoscopy(URS)in patients with ureteral calculi in any location.
1.Introduction
Stone disease is the third most common affliction of urinary tract and is also one of the most common causes of ureteral obstruction[1,2].Non-contrast computed tomography(NCCT)is the standard diagnostic method for obstructive ureteral stones,but not for indinavir stones.Hydronephrosis,enlarged ureter,perirenal fat stranding(PFS),pararenal fascial thickening,and perirenal fluid collection are secondary findings suggesting obstruction in NCCT[3].
PFS is linear area of soft-tissue in the perirenal space due to swelling of the fat surrounding the kidneys on NCCT(Fig.1).Although there are studies suggesting that PFS is a sign of acute pyelonephritis,some studies showed that PFS is not specific but may be a predisposing condition for acute pyelonephritis[4-6].
The urinary stone disease increases the risk of complicated urinary tract infection(UTI).Although ureterorenoscopy(URS)is a widely used method in the treatment of ureteral stones,the URS procedure increases the risk of UTI in the postoperative period[7,8].
The present study aimed to investigate whether PFS on NCCT is associated with infective complications after URS in patients with ureteral calculi.
2.Methods
The data of patients who were diagnosed with NCCT and treated with URS between January 2012 and January 2017 were retrospectively analyzed following the approval of the Giresun University Faculty of Medicine Clinical Research Ethics Committee(KAEK-03,03.10.2018/3).Patients who received antibiotic therapy for UTI or pyelonephritis prior to surgery and those who had undergone previous ureteral intervention or were treated with extracorporeal shock wave lithotripsy before the URS procedure were excluded from the study.

Figure 1 View of PFS in non-contrast computed tomography.PFS,perirenal fat stranding.
Urine cultures of all patients who underwent endoscopic stone procedures such as URS,SWL,and percutaneous nephrolithotripsy in our clinic were routinely examined before surgery,as recommended in the European Association of Urology guidelines[9].Only the patients with negative urine culture before the URS procedure were included in the study.Prophylactic antibiotics were administered 0-60 min before surgery,a single dose of 1 g cefazolin intravenously for adults and a single dose of 30 mg/kg intravenously for pediatric patients.All procedures were performed by three surgeons using a Karl Storz 27002L/K 8 Fr(Tuttlingen,Germany),or Richard Wolf 9.5 Fr(Knittlingen,Germany)semirigid ureteroscope under spinal or general anesthesia.In 14 patients,Ho:YAG laser energy was used and in 588 patients,a pneumatic lithotripter was used for stone fragmentation.Six hundred and two patients with complete medical records were included in the study.The gender and age of all patients,the size,side and localization of each stone,insertion of a double-J(DJ)stent,duration of surgical procedures,perioperative ureter injury and infectious complications after operation such as UTI,fever(defined as a temperature≥38°C),sepsis,and post-operative hospital stay were recorded.All NCCT scans were evaluated by the same radiologist.PFS is defined as the curvilinear areas of soft-tissue attenuation in the perirenal space in NCCT.Five hundred and thirty patients without PFS were classified as Group 1 and 72 patients with PFS were classified as Group 2.
Each group was compared in terms of gender and age of the patients,stone size,side,and localization,DJ stent insertion,perioperative ureteral injury,duration of hospital stay,and post URS infectious complications such as UTI,fever,and sepsis.
Pyuria(≥10 white blood cells per high-power field)and the presence of positive urine culture(≥105colony-forming units of uropathogen per milliliter)with or without fever and/or costovertebral angle sensitivity were evaluated as urinary infection.Signs of at least two systemic inflammatory response syndrome criteria such as fever>38°C or<36°C,heart rate>90 beats/min,respiratory rate>20/min or PaCO2<32 mmHg,and leucocytes>1 2000/mm3or<4000/mm3were accepted as urosepsis.
Statistical analysis was carried out using Statistical Package of Social Science(SPSS)software version 20.0(SPSS inc.,Chicago,IL,USA).Frequency and percentage distributions of the data were provided.Mann-Whitney U test was used to compare the variables between the groups that did not show normal distribution.Student’s t-test was used to compare the variables between the groups that show normal distribution.A p-value of less than 0.05 was considered to show a statistically significant result.Chi-square test and Fisher’s exact test were performed to compare the interdependencies between variables.For the multivariate analyses,the possible factors identified with univariate analyses were further entered into the logistic regression analyses to determine independent predictors of patients’outcome.Hosmer-Lemeshow goodness of fit statistics were used to assess the model fit.Type I error level of 5% was used to conclude statistical significance.
3.Results
The median age was 44(range:10-82)years in Group 1 and 43(range:20-71)years in Group 2 with no statistical difference(p=0.772).The female/male ratio was 0.56 in Group 1 and 0.29 in Group 2(p=0.021).Stone-free rates were 94.7%,95.2%,and 88.5% in all patients,Group 1,and Group 2,respectively(p=0.066).
The median stone size was 9(range:4-25)mm in Group 1 and 8(range:4-20)mm in Group 2.Remarkably,stone size was significantly smaller in patients with PFS(p=0.033)(Table 1).
In Group 1,253(47.7%)patients had the left ureter stones and 275(51.9%)patients had the right ureter stones.Similarly,in Group 2,35(48.6%)patients had left ureteral stones and 37(51.4%)patients had right ureteral stones.The number of lower,middle,and upper ureteral stones were 345(65.1%),126(23.8%),and 59(11.1%)in Group 1,and 55(76.4%),12(16.7%),and 5(6.9%)in Group 2,respectively.There were no statistical differences between both groups in terms of side of stones(p=0.820)and their localization distributions(p=0.145).
While the rate of hydronephrosis was 72.1% in Group 1,hydronephrosis was detected in 81.9% of the patients in Group 2.There was no statistically significant difference between the groups with and without PFS in terms of the incidence of hydronephrosis(p=0.076).It has also been shown that the presence of preoperative hydronephrosis has no effect on the development of postoperative infective complications(p=0.688)(Table 2).
The median interval time between the diagnosis and the operation was 12(range:1-46)days and 12(range:1-84)days for Group 1 and Group 2,respectively(p=0.903).The rate of patients with DJ stent insertion(29.2% in Group 1 and 27.8% in Group 2),as well as duration of procedures were statistically similar between both groups(p=0.904 and 0.910,respectively).The DJ stents were removed 2-4 weeks after the procedure and the DJ stent removal time was similar in both groups(p=0.66).
Infectious complications after URS were fever developments in 30(5.7%)patients in Group 1 and 38(52.8%)patients in Group 2.Development of post-procedure fever was significantly higher in patients with PFS(p=0.0001).UTIs were observed in 24(4.5%)and 27(37.5%)patients in Group 1 and Group 2,respectively with significant difference(p=0.0001).Urosepsis did not develop in any patient in Group 1,whereas urosepsis developed in 8(11.1%)patients in Group 2(p=0.0001)(Table 1).
The mucosal ureteral injuries were revealed in 13(2.5%)patients in Group 1 and 18(25.0%)patients in Group 2(p=0.0001).Ureteral perforation was detected in 3(0.6%)and 6(8.3%)patients in Group 1 and Group 2,respectively(p=0.0001).Ureteral avulsion was not experienced in any of the patients.Post-operative duration of stay in hospital was significantly higher in patients with PFS(p=0.033)(Table 1).

Table 1 Patients’data and postoperative infectious complications of two groups.
Since ureter perforation can also increase the risk of infectious complications,we reanalyzed the data after removal of patients with ureteral perforation.The frequencies of fever in Group 1 and Group 2 were 4.9% and 48.8%,respectively.Urinary infections rate was 3.4%in Group 1 and 30.2%in Group 2.While there was no urosepsis in Group 1,it was detected in 4.7% of the patients in Group 2.When patients with ureteral perforation were excluded,infective complications were also found to be statistically significantly higher in patients with PFS(p=0.005).
When we look at the total of infective complications,the risk of developing any infective complications after URS was found to be statistically significantly higher in the PFS group(p=0.002)(Table 2).According to the results of logistic regression analysis,PFS increased the risk of infection-related complications 49.8 times.The presence of impacted stones and DJ stenting at the end of the operation also increased the risk of infection-related complications 7.8-fold and 2.8-fold,respectively(Table 3).
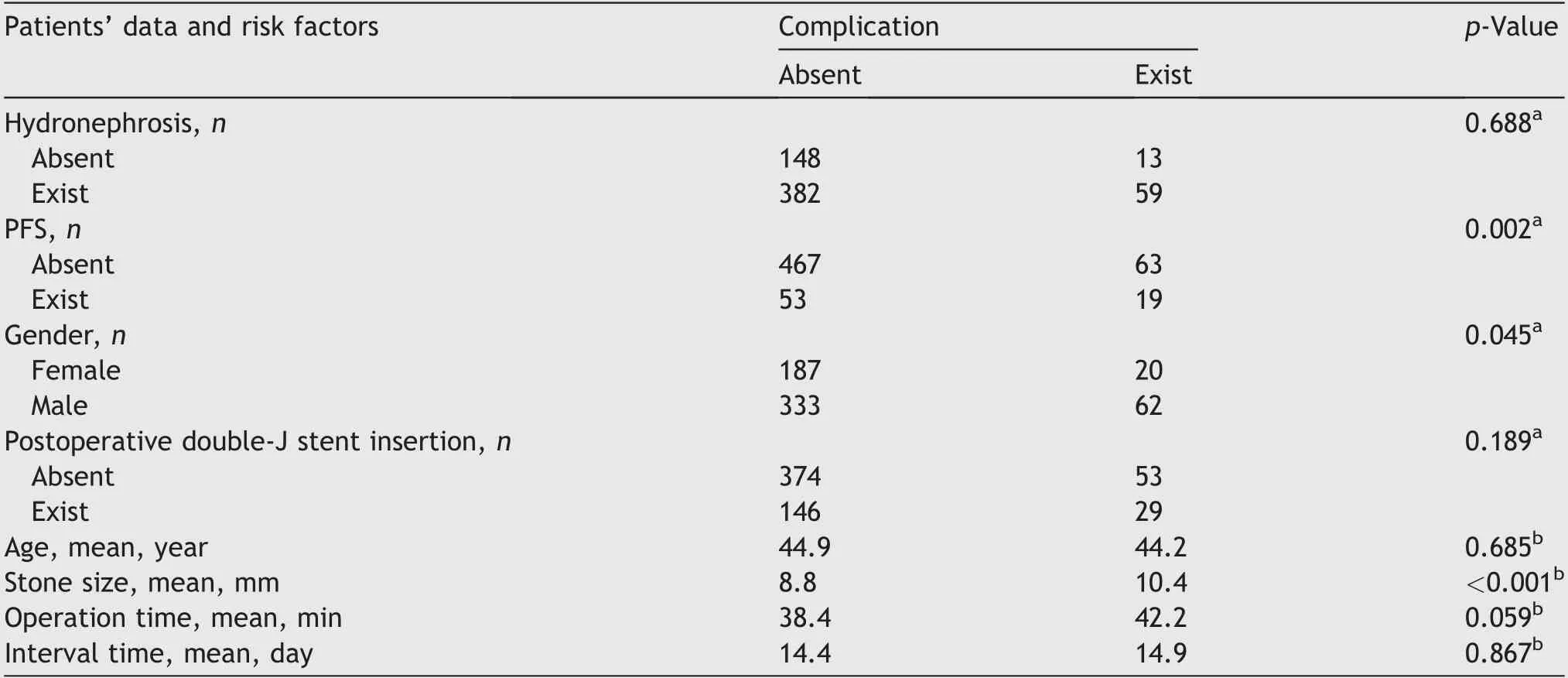
Table 2 Patients’data and risk factors for postoperative infectious complications.

Table 3 Logistic regression analysis for all infectious complications(fever,urinary infection,and urosepsis).
4.Discussion
Ureteral stones are one of the common causes of ureteral obstruction.Obstructed ureteral stones have primary and secondary findings in NCCT.The appearance of the stone in the ureter is the primary finding.Secondary manifestations include hydronephrosis,enlarged ureter,PFS,pararenal fascial thickening,and perirenal fluid accumulation[3].
Renal lymphatic pressure increases with increased intrapelvic pressure after acute ureter obstruction.Thus,fluid diffusion into renal interstitium occurs due to increased pressure.Continued pressure also causes rupture of renal calyceal.As a result of all these mechanisms,urinary extravasation develops into the perirenal area.In NCCT,linear dense changes in perirenal adipose tissue as a result of urinary extravasation are called PFS[10,11].PFS is an indication of urinary obstruction and can also be seen after spontaneous passage of a stone.This finding can also be seen in renal infection,inflammation,trauma,and renal vascular disease[12].In a study involving 312 patients presenting with renal colic,209 of all patients had PFS.In the same study,the authors emphasized that PFS is the second common secondary sign of obstruction following hydronephrosis[4].PFS detection rates in patients with UTIs range from 29.1% to 72%[5,6,13].In the literature,ithas been reported that advanced age and male gender increase the frequency of PFS significantly[11,13].The rate of patients with PFS was found to be approximately 12% in our study.The mean age in Group 1 and Group 2 were 44.9 years and 44.3 years,respectively without any difference.However,the number of male patients was detected significantly higher in the PFS group.The frequency of PFS in our study was slightly below the literature values.However,in the studies where the frequency of PFS was higher than in our study,the mean age was well above our mean and over 60 years old[5,6].
In patients with PFS,there was no significant relationship between PFSand stone localization[3,10].In our study,there was no significant difference between the groups in terms oflocalization.There are conflicting data between stone size and PFS in the literature.Although the development of PFS is reported to be independent of stone size[10],it has also been reported that PFS is significantly higher in patients with spontaneous transmission[3].As the stone size increases,the possibility of a spontaneous passage decreases[14].In our study,the median stone size was calculated as 8 mm in patients with PFS and 9 mm in patients without PFS.This difference was statistically significant.
It is confusing to explain the small stone size in patients with PFS.However,as a hypothesis,this may be due to low ureter calibration in some patients.Therefore,small stones can cause further blockage,causing PFS during spontaneous passage.However,this paradox still needs to be explored by further studies.Another reason that develops PFS is UTI.Although PFS is the most common NCCT finding in patients with acute pyelonephritis,the sensitivity and specificity of PFS in the diagnosis of acute pyelonephritis are 72% and 60%,respectively.Therefore,it is possible to define that PFS has insufficient reliability in the diagnosis of acute pyelonephritis.It has been reported that bacteremia is more common in patients with PFS.However,when febrile UTI develops in these patients,fever continues for longer[6,13].URS is used as a safe and easy method in the treatment of ureteral stones.However,various complications from microscopic hematuria to mortality have been reported to be associated with the URS operation[8,15-17].Infectious complications are generally considered as post-procedural fever,UTI,and urosepsis.In the literature,infectious complication rate ranges from 9% to 25%[18-21].A multi-center study involving 11 885 patients reported the rate of UTI was 1% and the rate of sepsis was 0.4%.In this study,both rigid URS and flexible URS were used in treatment[22].In another study using only rigid URS,postoperative rates of fever,UTI,and urosepsis were 10.2%,6.9%,and 1.2%,respectively[15].
In the present study,we evaluated the relationship between the infectious complications and PFS detected on NCCT in patients who underwent URS.Postoperative fever and UTI rates were 5.7% and 4.5% in patients without PFS,respectively,while 52.8% and 37.5% in patients with PFS(p=0.0001).While urosepsis was seen in 8(11.1%)patients in the PFS group,no urosepsis was observed in the non-PFS group.When we evaluated the postoperative infective complications in total,it was found that the rate of infective complications was higher in the group with PFS than in the group without PFS(p=0.002).According to results of logistic regression analysis,PFS increased the risk of infection related complications such as fever,UTI,and urosepsis 49.8-fold.
In addition,when evaluating ureteral injuries that may be associated with postoperative fever in the present study,mucosal injury(2.5% vs.25.0%)and ureteral perforation(0.6% vs.8.2%)were both detected significantly higher in patients with PFS(Table 1).Since ureter perforation might be a cause of an increased risk of infectious complications,we reanalyzed the data after excluding patients with ureteral perforation.We found that all infectious complications were significantly higher in patients with PFS,according to reanalysis results(p=0.002).
It has been reported in the literature that longer operative time is a risk factor for postoperative fever and systemic inflammatory response syndrome after ureteroscopy[23].However,the duration of surgical procedures in the present study was statistically similar in both groups.
It has been reported that DJ stent placement after URS does not increase the rate of postoperative infection[24].However,DJ stent placement before and after URS has been reported to increase infectious complications in patients with and without PFS[15,25,26].In our study,there was no difference in terms of DJ stent placement in patients with and without PFS.According to the results of logistic regression analysis,DJ stent insertion at the end of the operation increased the risk of infection related complications by 2.8-fold.
Hydronephrosis,like PFS,is an indicator of obstruction,and hydronephrosis is expected to be more common in patients with PFS.Rashid and Fakhulddin[27]have been reported that the presence of preoperative hydronephrosis increases the risk of developing postoperative fever,but has no effect on the development of sepsis.However,in the present study,hydronephrosis was similar in groups with and without PFS(p=0.076).It was shown that the presence of hydronephrosis did not have a statistically significant effect on the development of total infective complications(p=0.688).
Increase in stone size creates susceptibility to infectious complications.In a study comparing patients with and without infectious complications,the mean stone size was calculated as 16.6 mm in patients without complications and 20.6 mm in patients with complications[20].In our study,the median stone size was found to be 8 mm in patients with PFS and 9 mm in patients without PFS.
Although the duration of the stone in the ureter until the time of diagnosis is an important parameter for PFS formation,some patients could not be commented on this issue in our retrospective study due to insufficient data.Although all NCCT scans were evaluated by the same radiologist,the retrospective design of the study appears to be a limitation of the study.However,we think that this study will be a guiding light due to the limited number of studies demonstrating the importance of PFS.Larger scale prospective studies will also enable us to reach more robust results on this subject.
5.Conclusions
In conclusion,the risk of postoperative infectious complications is higher in patients with ureteral stones with PFS.Patients with PFS on NCCT should be monitored more closely in the postoperative period in terms of fever,UTI,and urosepsis.The effect of preoperative drainage on infectious complications should be investigated.
1.Presence of PFS in ureteral stones may predispose to postoperative infection.
2.Presence of PFS in ureteral stones may increase the risk of perioperative ureter injury.
3.Postoperative hospital stay was found to be longer in patients with PFS.
For the above reasons,patients with ureteral stones should be carefully examined in terms of preoperative PFS,and patients with PFS should be followed up closely in ordernot to miss or delay the diagnosis of infective complications in the postoperative period.
Author contributions
Study concept and design:Erhan Demirelli,Ural Ouz.
Literature research:Erhan Demirelli,Ercan O¨reden,Cemil Bayraktar.
Data acquisition:Erhan Demirelli,Cemil Bayraktar,Alptekin Tosun.
Drafting of manuscript:Ural Ouz,Alptekin Tosun.
Critical revision of the manuscript:Erhan Demirelli,Ural Ouz,Ercan O¨reden.
Manuscript writing:Erhan Demirelli.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年3期
Asian Journal of Urology2022年3期
- Asian Journal of Urology的其它文章
- Burned-out testicular seminoma with retroperitoneal metastasis and contralateral sertoli cell-only syndrome
- Endoscopic management of adolescent closed Cowper’s gland syringocele with holmium:YAG laser
- Transcutaneous dorsal penile nerve stimulation for the treatment of premature ejaculation:A novel technique
- Bilateral calcified Macroplastique® after 12 years
- Culture-positive urinary tract infection following micturating cystourethrogram in children
- A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer