
Evaluating factors associated with the risk of hydrothorax following standard supracostal percutaneous nephrolithotomy
2022-09-20 03:30:14PankajMaheshwariAmandeepAroraMaheshSaneVivekJadhao
Asian Journal of Urology 2022年3期
Pankaj N.Maheshwari*,Amandeep Arora,Mahesh S.Sane,Vivek Jadhao
Department of Urology,Fortis Hospital Mulund,Mumbai,India
KEYWORDS Calculous disease;Stone;Supracostal;Percutaneous nephrolithotomy;Hydrothorax
Abstract Objective:To report our experience with supracostal percutaneous nephrolithotomy(SC-PNL)and evaluate factors which could predict the risk of hydrothorax following SC-PNL.
1.Introduction
Since its first description more than 4 decades ago,percutaneous nephrolithotomy(PNL)has revolutionised the way we treat renal stones.PNL is now the recommended modality to treat stone burden more than 2 cm[1].It is also the fall-back option when other modalities like retrograde intrarenal surgery and extracorporeal shock wave therapy fail.
Establishing an ideal percutaneous access is the initial and the most crucial step of performing PNL.The ideal access tract should be the shortest direct approach to the stone via a renal papilla.With this as the guiding principle,most stones in the lower and middle group of calyces and the pelvis can be reached via a subcostal percutaneous access[2].An attempt to reach the upper group of calyces through a lower calyceal puncture may be traumatic to the upper calyceal infundibulum.A lower calyceal access would also impede approach to a stone impacted at the ureteropelvic junction or just distal to it.For such situations,an upper calyceal access is usually required which almost always needs a supracostal puncture[2].Sometimes,access to even the middle group of calyces would require a supracostal puncture.
Although it was initially discouraged due to concerns about injuring the pleura or the lung,multiple series have described their experience with supracostal PNL(SC-PNL)[3-10].Most of them have compared supracostal and subcostal approaches in their studies and reported a higher,but acceptable rate of complications with the supracostal approach.A recent meta-analysis concluded that SC-PNL is associated with a significantly higher incidence of hydrothorax compared to the subcostal approach[11].
Although it is well known that SC-PNL is associated with a higher incidence of post-operative hydrothorax,there are scarce data available about what factors while performing a SC-PNL could lead to the hydrothorax.In addition,very few studies reported results with supra-11th rib punctures[9,10,12].In this retrospective study,we sought to review our experience with SC-PNL and find out factors which were significantly associated with post-operative hydrothorax following SC-PNL.
2.Patients and methods
2.1.Patients
This study was approved by the institutional ethics committee(IEC/2017/OAS/17).We searched a prospectively maintained institutional registry for patients undergoing PNL from January 2011 to December 2019.We excluded patients undergoing miniaturized PNL and those with history of ipsilateral renal surgery.Out of the 980 patients undergoing primary standard PNL during this period,347(35.4%)underwent SC-PNL.In all these patients,a supracostal puncture was made only if a lower calyceal tract was considered inadequate for complete stone clearance.Patients who required a second subcostal access for complete stone clearance were also included.
A complete blood count,serum biochemistry and coagulation profile,urine culture,ultrasound of the kidneys,ureters and bladder,chest X-ray,and a computed tomography urography or intravenous urography were performed in all patients.All patients were explained about the possible need of an intercostal drain and informed consents were obtained.
2.2.PNL technique and post-operative course
All cases were performed under general anesthesia.In the lithotomy position,a 6 Fr ureteral catheter was placed.All patients underwent fluoroscopy guided punctures in the prone position.The access tract was made either in the 10th or 11th intercostal space just superior to the lower rib to avoid injuring the intercostal neurovascular bundle(lower half of the intercostal space).In patients who also needed a subcostal access tract,the tract that offered access to most stone burden was made first.The supracostal puncture and subsequent tract dilatation were done with the patient maintained in full expiration.Whenever possible,this tract was created just lateral to the midscapular line.As depicted in Fig.1,the parietal pleura is attached to the 12th rib at the mid-scapular line.Thus,a puncture in the 11th intercostal space lateral to the midscapular line would avoid passing through the pleural cavity and thus theoretically would not result in hydrothorax.
The access tract was dilated with metallic dilators(Alken telescopic dilators,Karl Storz Ltd.,Tuttlingen,Germany)up to 24 Fr and a 24 Fr sheath(Amplatz sheath,Cook Medical,Brisbane,Australia)was then passed.A rigid nephroscope(22 Fr with 20°lens,Richard Wolf GmbH,Knittlingen,Germany)and a pneumatic lithotrite(Swiss LithoClast,Boston Scientific,Marlborough,MA,USA)were used for all cases.A double-J ureteric stent and a nephrostomy tube(NT)were placed in all cases.At the end of the procedure,the costophrenic angle was examined under fluoroscopy.If the angle was clear and chest auscultation was normal,the patients were monitored clinically(Fig.2).Patients with an obscured angle or decreased air entry on auscultation were managed as per the protocol described previously by us[13].The first step was to confirm thediagnosis of a pleural collection by a portable chest X-ray or a chest ultrasound.The collection was then tapped under fluoroscopy guidance to determine the nature of the fluid.If the fluid was clear(indicating irrigation fluid)and was of small amount,then the collection was completely aspirated,during which the anesthetist hyperventilated the patient.If the lung was seen to expand completely,no indwelling chest tube was placed and the patient was kept under close observation.If,however,the quantity of the clear fluid was more or if the aspirate was haemorrhagic,then a chest tube was placed and connected to an underwater drainage system.
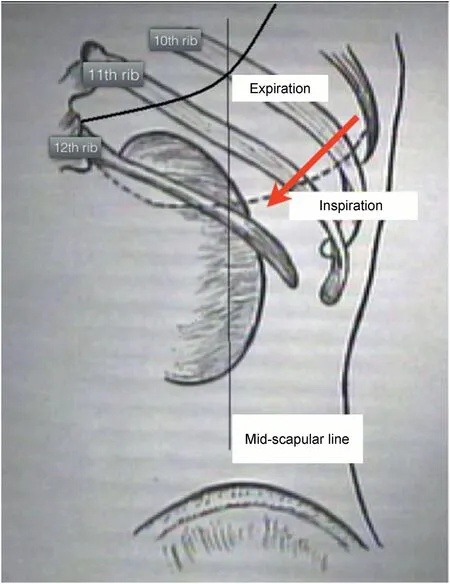
Figure 1 Anatomical relations of the parietal pleura in both phases of respiration.It also shows that a puncture lateral to the mid-scapular line(red arrow)would miss the parietal pleura in expiration.
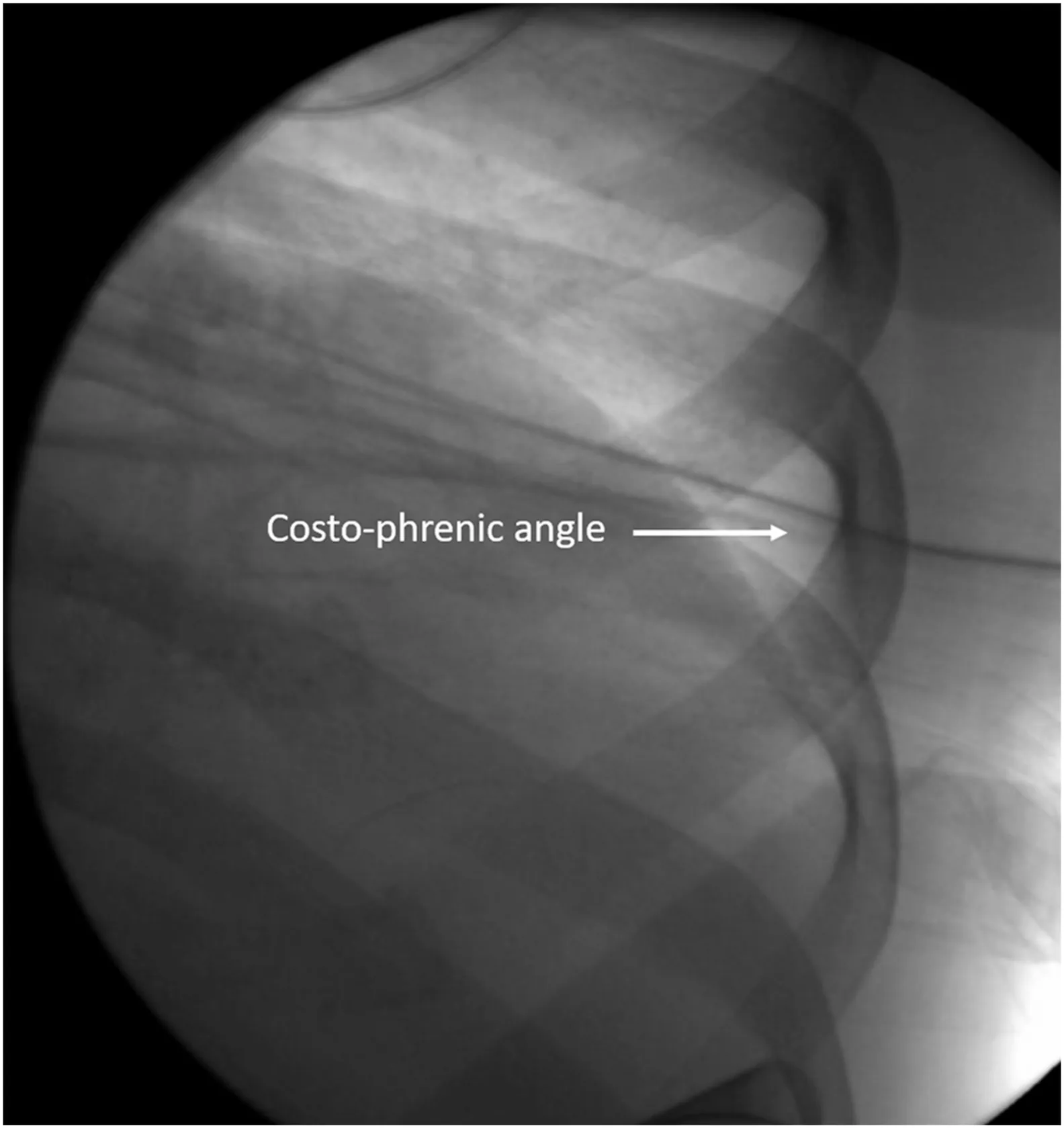
Figure 2 The costo-phrenic angle is seen clearly on fluoroscopy at the end of the procedure.This determines absence of pleural violation.
A preoperative antibiotic was given to every patient at the time of induction.Antibiotic therapy was continued until removal of the NT.The per urethral catheter was removed 6 h following NT removal.Residual stone fragments were evaluated by a post-operative abdominal radiograph or an ultrasonography(for radiolucent stones).A chest radiograph was performed before discharge.Clinical chest evaluation was repeated at 3 weeks follow-up visit.When needed,a chest radiograph was repeated.
Patients were assessed for demographic characteristics,indication for the supracostal access,level of supracostal access,anatomy of the kidney(normal or malrotated),site of the puncture in relation to the mid-scapular line(medial or lateral),and whether another subcostal tract for stone clearance was required or not.Patients were assessed for the incidence of hydrothorax and requirement of intercostal drain depending on the level of percutaneous access.Also,a regression analysis model was developed to identify factors which could predict the occurrence of hydrothorax following SC-PNL.
2.3.Statistical analysis
Normality of the data was determined using the Kolmogorov-Smirnov test.The unpaired t-test and Chi-square test or Fisher exact test were used to compare the statistical significance of differences in means and proportions respectively.Multivariable logistic regression analysis was performed to determine predictors of hydrothorax following SC-PNL.Statistical significance was considered at p<0.05.Statistical analyses were performed using SPSS v.20.0 software(IBM Corporation,Armonk,NY,USA).
3.Results
3.1.Demographics,supracostal tracts,and their indication
SC-PNL was performed in 347 patients during the study period.This included 211(60.8%)male and 136(39.2%)female patients with a mean age of 36.7 years(range 13-67 years).Most of the patients were treated by a supra-12th rib approach(n=248;71.5%),while the rest needed a supra-11th(n=85;24.5%)or a supra-10th(n=14;4.0%)rib tract.A single supracostal tract was made in 225(64.8%)patients while an additional subcostal tract was required in 122(35.2%)patients.
Table 1 lists the indications for SC-PNL in the patients with the site of their supracostal puncture.A staghorn stone was the most common indication(49.3%)followed by upper calyceal stone(18.2%),impacted large upper ureteric stone(17.9%),upper ureteric stone with lowercalyceal stone(11.2%),and upper calyx diverticular stone(3.5%).

Table 1 Distribution of patients according to stone burden and the site of puncture.
3.2.Incidence of pleural complications and its predicting factors
Table 2 summarizes the incidence of hydrothorax and requirement of intercostal drain.
Overall,17(4.9%)patients developed a hydrothorax while an intercostal drain was required in seven of these 17 patients for 48 h.The other ten patients who had a clinically insignificant pleural effusion were managed conservatively.Pleural effusion resolved on follow-up in all these patients.All patients showed a proper expansion of lung at 3 weeks post-operative radiograph.
None of the patients with a supra-12th rib puncture required an intercostal drain.More than a third of the patients with a supra-10th puncture developed a hydrothorax(35.7%)and all of them required an intercostal drain.A supra-11th rib access was associated with a significantly higher incidence of hydrothorax(p<0.001)compared to a supra-12th rib access,but it did not lead to a significantly higher requirement of intercostal drain(p=0.06).A significantly higher incidence of hydrothorax and intercostal drain requirement was observed when supra-10th rib access was compared to a supra-11th rib tract.
Predictors of hydrothorax following SC-PNL are summarized in Table 3.Factors such as anteriorly malrotated kidney(odds ratio[OR]=2.722;95%confidence interval[CI]=1.042-5.617,p=0.03),puncture medial to the midscapular line(OR=1.669;95% CI=0.542-1.578,p=0.03),and an access higher than the supra-12th level(OR=5.265;95% CI=1.292-9.342,p<0.001)proved to be independent predictors of hydrothorax following a SC-PNL on multivariable logistic regression analysis.Requirement of an additional subcostal tract did not significantly increase the risk of hydrothorax(p=0.1).

Table 2 Incidence of hydrothorax and intercostal drain requirement in supracostal percutaneous nephrolithotomy.

Table 3 Univariable and multivariable logistic regression analysis to determine predictors of hydrothorax following supracostal percutaneous nephrolithotomy.
4.Discussion
Despite the initial inhibitions,SC-PNL has been widely adopted with multiple series reporting its feasibility,safety,and efficacy[3-10].However,supracostal access carries with it an inherently higher risk of hydrothorax and requirement of intercostal drain insertion,compared to a subcostal puncture.Our results showed that puncture medial to the mid-scapular line,anteriorly malrotated kidney,and puncture higher than the 12th intercostal space were factors significantly associated with hydrothorax post SC-PNL.
While most of the renal stone burden can be accessed via subcostal tracts,certain types of stone burdens and renal anatomies necessitate a supracostal access.A higher rate of complications with SC-PNL has been uniformly reported in literature[11].With this background,we have used the supracostal approach only when the subcostal approach was deemed inadequate for stone clearance.The most common indication in our series was a staghorn calculus followed by an upper calyceal calculus.Some other series have reported similar indications[4,9],while some have reported their stone burdens in the form of stone number[3]or stone size[10].In some of our patients,especially those with upper ureteric calculi and upper calyceal calculi,a supracostal puncture could have been avoided if we had access to flexible nephroscopy.There is very scarce evidence for supra-10th rib punctures.Therenal anatomy and stone location compelled us to create an access tract above the 10th rib in 14 of our cases with seven of these being for upper calyceal stones.
de la Rosette and colleagues[14]published a consensus of complications in PNL graded as per the Clavien-Dindo classification(CDC).According to this,hydrothorax managed by watchful waiting is graded as a CDC 1 complication while hydrothorax requiring placement of an intercostal drain is included under CDC 3a complications.Other series have reported a 0%-12% incidence of hydrothorax with SC-PNL[2-4,11].We encountered post-operative hydrothorax in 4.8% of all our supracostal punctures.However,only seven of these(2% of total cases)had clinically significant hydrothorax which required placement of an intercostal drain.It is important to note that none of our patients with a puncture in the 11th intercostal space developed a hydrothorax which was significant enough to warrant insertion of an intercostal drain.Sinha et al.[10](179 supra-11th punctures)reported a 7.3% incidence of hydrothorax with a 2.2%risk of needing an intercostal drain and our results are comparable to this.We believe our incidence of pleural complications is very low in this subgroup as most of our punctures were from the lateral half of the intercostal space where the chance of encountering the pleural cavity is very low.Kara and colleagues[12]reported that only two of their 39(5.1%)cases with a supra-11th access developed a hydrothorax,but none of them needed an intercostal drain.Apart from this,there is not much evidence about pulmonary complications with supra-11th access.It is prudent to note that all of our patients who underwent a supra-10th rib access developed significant hydrothorax and required an intercostal drain.None of our patients experienced a lung parenchymal injury.
Thus,we can conclude that a supra-12th rib access is associated with a minimal risk of a significant hydrothorax and although a supra-11th rib access has a higher risk of requiring an intercostal drain,the actual incidence of the complication is still low.It does add to the morbidity and prolongs hospital stay,but is not life threatening.A supra-10th rib access has an extremely highchance ofdevelopinga significant hydrothorax and should be avoided unless absolutely unavoidable.Almost all of our supra-10th punctures were performed during the first few years of the study.Over time,we have become very selective with the use of supra-10th puncture in our practice.With the availability of the flexible nephroscope and flexible ureteroscope in recent times,a supra-10th puncture is rarely,if ever,required.
None of the series reporting on SC-PNL have evaluated factors which might predict occurrence of hydrothorax following a supracostal puncture.We found that an anteriorly rotated kidney and puncturing medial to the mid-scapular line were independent factors associated with the risk of developing a hydrothorax.These two factors may in fact be inter-related.Our technique of SC-PNL was to make the tract lateral to the mid-scapular line in an attempt to avoid going through the pleural cavity in the 11th intercostal space.However,if the kidney is anteriorly rotated,the posterior calyces are oriented in a more sagittal plane and the puncture needs to be situated medially to develop the shortest possible tract which is in line with the direction of the upper calyx.This can increase the risk of pulmonary complications.
The other factor which was found to be an independent predictor of hydrothorax on multivariable analysis was the level of the supracostal puncture.As discussed above,higher the puncture,greater is the risk of developing hydrothorax due to increased chance of violating the pleural space.
We would like to discuss few nuances about the technique of SC-PNL which help us in maintaining a very low incidence of this specific complication of hydrothorax[15].Firstly,it is of utmost importance to have knowledge about the anatomy of the visceral and parietal pleura.Stening and Bourne[16]elaborately described the pleural anatomy and the anatomic basis of a supracostal puncture.The parietal pleura is closely applied to the diaphragm and crosses the 12th rib at its midpoint near the mid-scapular line.The visceral pleura is closely applied to the lung surface and at the mid-scapular line,it is in relation with the 10th rib.The pleural rib-levels are summarised in Fig.1.The parietal and visceral pleurae ascend cranially and laterally on the ribs and further rise in deep expiration.Thus,a puncture made lateral to the mid-scapular line,below the tenth rib,in deep expiration would almost always prevent damage tothe visceral pleura.Tracts below the eleventh rib made lateral to the mid-scapular line would miss not only the visceral pleura but also may miss the parietal pleura.Tracts made through the parietal pleura may not be of clinical significance especially when the Amplatz sheath was utilised,as this would avoid the leakage of the irrigation fluid in the pleural space by maintaining a low-pressure irrigation.Secondly,an experienced anaesthetist played a major role during supracostal puncture and tract dilatation.The anesthetist should co-ordinate the respiration to maintain the patient in expiration during puncture and tract dilatation to increase the distance between the visceral and parietal pleurae.Thus,a supracostal access tract should be made in full expiration lateral to the mid-scapular line no higher than the 10th intercostal space,unless the renal anatomy or stone burden compelled us to make a medial or higher puncture.
We all have encountered an occasional patient with an absent 12th rib.Although there is no available literature about SC-PNL in such patients,we believe that a supra-11th puncture in such a patient should be planned according to the same guiding principles.
We do acknowledge the retrospective nature of our study.Also,we did not evaluate the role of tubeless SC-PNL as our practice has been to use a NT for all cases with SC-PNL.A recently reported randomized study has shown a decreased incidence of hydrothorax with a tubeless approach following SC-PNL[17].Despite these limitations,our series presents one of the largest single centre experiences with SC-PNL and is one of the few studies to evaluate factors predicting the risk of hydrothorax following SC-PNL.
5.Conclusion
SC-PNL may be required in about a third of all PNLs for effective stone clearance.Creating the access tract medial to the mid-scapular line,an anteriorly malrotated kidney and a puncture higher than the 12th intercostal space are factors which have a significantly higher risk of leading to hydrothorax post SC-PNL.Very few patients develop clinically significant hydrothorax needing an intercostal drain.A supra-10th rib puncture should be avoided unless absolutely necessary.Adhering to the underlying principles of creating a supracostal tract will help to decrease the incidence of hydrothorax post SC-PNL.Knowledge of the predicting factors will help to anticipate the risk of hydrothorax in a particular patient and take necessary peri-operative measures.
Author contributions
Study concept and design:Pankaj N.Maheshwari.
Data acquisition:Pankaj N.Maheshwari,Amandeep Arora,Vivek Jadhao.
Data analysis:Pankaj N.Maheshwari,Amandeep Arora,Mahesh S.Sane.
Drafting of manuscript:Pankaj N.Maheshwari,Amandeep Arora,Mahesh S.Sane.
Critical revision of the manuscript:Pankaj N.Maheshwari,Amandeep Arora,Mahesh S.Sane,Vivek Jadhao.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2022年3期
Asian Journal of Urology2022年3期
- Asian Journal of Urology的其它文章
- Burned-out testicular seminoma with retroperitoneal metastasis and contralateral sertoli cell-only syndrome
- Endoscopic management of adolescent closed Cowper’s gland syringocele with holmium:YAG laser
- Transcutaneous dorsal penile nerve stimulation for the treatment of premature ejaculation:A novel technique
- Bilateral calcified Macroplastique® after 12 years
- Culture-positive urinary tract infection following micturating cystourethrogram in children
- A phase II study of neoadjuvant chemotherapy followed by organ preservation in patients with muscle-invasive bladder cancer