
Machine learning predicts portal vein thrombosis after splenectomy in patients with portal hypertension: Comparative analysis of three practical models
2022-09-14 06:33JianLiQiQiWuRongHuaZhuXingLvWenQiangWangJinLinWangBinYongLiangZhiYongHuangErLeiZhang
World Journal of Gastroenterology 2022年32期
Jian Li, Qi-Qi Wu, Rong-Hua Zhu, Xing Lv, Wen-Qiang Wang, Jin-Lin Wang, Bin-Yong Liang, Zhi-Yong Huang, Er-Lei Zhang
Abstract
Key Words: Portal hypertension; Splenectomy; Portal vein thrombosis; Postoperative platelet elevation rate;Practical model; Machine learning
lNTRODUCTlON
Liver cirrhosis is recognized as an extremely important and rapidly increasing disease burden in the world[1]. In the progressive stage of liver cirrhosis, the complications caused by portal hypertension(PH), including esophagogastric variceal bleeding and hypersplenism, pose a great threat to the patients’ life and health[2,3]. Liver transplantation is currently recommended as a curative treatment for liver cirrhosis combined with PH; however, due to the shortage of liver sources and high transplantation cost, its clinical practicability is limited[4,5]. Transjugular intrahepatic portosystemic shunt seems to be a gospel for PH, but unfortunately, restenosis or/and hepatic encephalopathy will occur in more than 60% of patients[6,7]. In Asia, splenectomy (or combined with devascularization) has been widely adopted as an effective treatment for hypersplenism or esophageal and gastric variceal bleeding caused by PH[8,9].
Portal vein thrombosis (PVT) is often defined as thrombosis within the portal vein trunk or intrahepatic portal branches, with or without the splenic vein or superior mesenteric vein involvement[10,11]. PVT is considered a dreaded complication after splenectomy for patients with PH[12], and the probability of PVT has been reported to be 4.8%-51.5%[13-15]. For patients with acute PVT and PVT resulting in superior mesenteric vein thrombosis, it has been reported that PVT may be closely associated with acute liver failure and could influence mortality[16]. Hence, strategies are needed to prevent PVT in patients who underwent splenectomy. In clinical practice, anticoagulation is a critical method for the prevention and treatment of PVT in patients after splenectomy. However, when the anticoagulation therapy should be started remains controversial. Early anticoagulation may result in life-threatening bleeding events for patients with liver cirrhosis. Whether anticoagulant therapy should be prescribed to all patients after splenectomy deserves careful consideration. In addition, the majority of patients with PVT are asymptomatic and only a few experience abdominal discomfort[12]. Therefore,there is an urgent requirement to find effective diagnostic methods to early and rapidly identify individuals with high risk of PVT after splenectomy, and then further guide clinicians to take intervention measures. Color Doppler ultrasonography and/or contrast-enhanced computed tomography (CT) is commonly applied for the final diagnosis of PVT[17]; however, they seem to be useless for screening out the high-risk individuals who are vulnerable to PVT. Given this, many scholars attempted to investigate the risk factors closely related to the occurrence of PVT after splenectomy[8,18-21]. Several investigators paid attention to the fact that preoperative low platelet count (PLT) and postoperative high PLT may be crucial predictors of the risk of PVT postoperatively[19,22].
Generally speaking, patients with PH will experience rebounding rises in PLT after splenectomy[23],combined with hemodynamic changes in the portal venous system, and thus these patients are highly prone to developing PVT[24]. However, the effect of the amplitude of sharp postoperative rises in PLT on PVT has received little attention. We speculated that the postoperative platelet elevation rate (PPER)should be an important predictor of PVT. To the best of our knowledge, there are no reports on the relationship between PPER and PVT.
In recent years, to meet the urgent demand of finding effective methods to predict PVT after splenectomy, several studies have attempted to construct predictive models for PVT after splenectomy in patients with cirrhosis using multivariate regression analysis[25,26]. However, there are few clinical variables included in the analysis and the accuracy of these prediction models is still unsatisfactory.Therefore, there is an urgent need for an efficient and accurate visualization model.
Nowadays, novel machine learning algorithms based on more clinical features have shown great potential in various aspects of medical research, especially in the construction of predictive models, and the features screened for model construction are clinically interpretable[27-29]. Gaoet al[28] constructed four machine learning models based on 53 raw clinical features of coronavirus disease 2019 patients to distinguish individuals at high risk for mortality, with an area under the receiver operating characteristics (ROC) curve (AUC) of 0.976. Kawakamiet al[29] developed seven supervised machine learning classifiers based on 32 clinical parameters, among which the random forest (RF) model showed the best performance in distinguishing epithelial ovarian cancer from benign ovarian tumors with an AUC of 0.968. The wide range of applications of machine learning methods has surpassed conventional statistical analysis due to their higher accuracy, which might enable machine learning to be increasingly applied in the field of medical research[30-32]. Although compared with traditional multivariate analysis methods, machine learning algorithms have overwhelming advantages in constructing clinical prediction models, so far, only Wanget al[33] have tried to construct a prediction model of PVT after splenectomy in cirrhotic patients with PH using machine learning algorithms. The model that they constructed has greatly improved the prediction efficiency compared with the traditional models.However, the clinical parameters involved in the construction of the model are extremely complex,which limits its clinical use.
Therefore, the purpose of this study was to evaluate the predictive value of PPER for the risk of PVT after splenectomy for patients with PH. In addition, we sought to build simple, efficient, and accurate practical models for predicting PVT with machine learning algorithms to facilitate assisting clinicians in the early identification of individuals at high risk of PVT after splenectomy and taking intervention measures in time. We present the following article in accordance with the TRIPOD reporting checklist.
MATERlALS AND METHODS
Study population
We retrospectively recruited 944 consecutive patients aged no less than 18 years who underwent splenectomy at our institution between July 4, 2011 and September 7, 2018. The patients with the following conditions were excluded: (1) Splenic space-occupying lesion; (2) Hematological disease; (3)PH caused by non-hepatitis B virus (HBV) related etiologies, such as schistosome, hepatitis C virus, or other unknown causes;(4)Presence of PVT confirmed by preoperative imaging;(5)Previous history of endoscopic therapy, splenic embolization, shunt surgery, or anticoagulants; (6) Incomplete clinical features; (7) Unelevated PLT on the first (PLT1) and third day (PLT3) after the operation compared to the preoperative values; and (8) Receiving prophylactic anti-coagulant therapy after splenectomy.Finally, a total of 483 patients with PH interrelated to HBV were included in this study. The flow diagram of patient selection and study design is shown in Figure 1A. The study was approved by the Medical Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology.Owing to the retrospective nature of this study, written informed consent was waived.
Data collection

Figure 1 Flow chart and correlation chart. A: Flow diagram of patient selection and study design; B: Correlation matrix between candidate variables. The size and color of the circle in the matrix reflect the correlation between the corresponding variables. The darker the blue, the stronger the positive correlation between variables, and the darker the red, the stronger the negative correlation between variables. HCV: Hepatitis C virus; HBV: Hepatitis B virus; PLT1 and PLT3: Platelet counts on the first and third days after operation; PVT: Portal vein thrombosis; GLM: Generalized linear model; LSM: Least absolute shrinkage and selection operator model; RFM: Random forest model; RBC: Red blood cells; HLB: Hemoglobin; WBC: White blood cells; N: Neutrophil count; L: Lymphocyte count; NLR: Neutrophil to lymphocyte ratio; PLT: Platelet count; PLR: Platelet to lymphocyte ratio; PT: Prothrombin time; PTA: Prothrombin activity; INR: International normalized ratio; FIB:Fibrinogen; APTT: Activated partial thromboplastin time; ALT: Alanine aminotransaminase; AST: Aspartate aminotransaminase; ALB: Serum albumin; TBIL: Total serum bilirubin; Child: Child-Pugh grade; EGV: Esophageal and gastric varices; SPT: Spleen thickness; DPV: Diameter of the portal vein; PBT: Preoperative blood transfusion; De: Devascularization; PPER1: Platelet elevation rate at postoperative day 1; PPER3: Platelet elevation rate at postoperative day 3.
All the patients’ clinical features were acquired from the electronic medical record system in our institution, which mainly included sex, age, smoking and drinking history, previous treatment history,etiologies, blood biochemical parameters, and imaging information. The blood biochemical parameters included routine blood tests [red blood cells (RBC), reference interval: 4.30-5.80 × 1012/L; hemoglobin,reference interval: 130.0-175.0 g/L; white blood cells (WBC), reference interval: 3.50-9.50 × 109/L;neutrophil count (N), reference interval: 1.80-6.30 × 109/L; lymphocyte count (L), reference interval:1.10-3.20 × 109/L; neutrophil to lymphocyte ratio (NLR); PLT, reference interval: 125.0-350.0 × 109/L;platelet to lymphocyte ratio], coagulation function [prothrombin time, reference interval: 11.5-14.5 s;prothrombin activity (PTA), reference interval: 75.0%-125.0%; international normalized ratio, reference interval: 0.80-1.20; fibrinogen, reference interval: 2.00-4.00 g/L; activated partial thromboplastin time,reference interval: 29.0-42.0 s], and liver function [alanine aminotransaminase (ALT), reference interval:≤ 41 U/L; aspartate aminotransaminase (AST), reference interval: ≤ 40 U/L; serum albumin, reference interval: 35.0-52.0 g/L; serum total bilirubin, reference interval: ≤ 26 μmol/L] within 7 d before surgery,as well as PLT1 and PLT3. The preoperative Child-Pugh grade was divided into three levels of A, B, and C[34], with grade C excluded. Information on the esophageal and gastric varices (EGV), spleen thickness(SPT), diameter of the portal vein (DPV), and preoperative blood transfusion (PBT) within 7 d before the operation was also collected.
Definition of variables
We diagnosed PVT by color Doppler ultrasound examination[35] and contrast-enhanced CT would be applied as an auxiliary examination when its diagnosis was questioned[36]. In this study, abdominal ultrasound and contrast-enhanced CT examinations were routinely performed within 7 d before the operation. Routine ultrasonography was performed on the 7thday after the operation[19,20], or at any time when there were suspected clinical symptoms of PVT such as fever, severe abdominal pain,vomiting, abnormal liver function, and leukocytosis[12].
According to the definition of varices[8], EGV was divided into EGV without varices and EGV with varices in this study. SPT was defined as the vertical distance between the splenic hilum and the cut point of the lateral margin, and DPV was measured as the largest anteroposterior diameter at the point of intersection with the hepatic artery, during the patient’s breath holding[37].
The PPER was calculated from the preoperative PLT and postoperative PLT. For example, PPER1 (at the first day) was calculated as (PLT1 - PLT)/ PLT × 100%, and PPER3 (at the third day) was calculated as (PLT3 - PLT)/ PLT × 100%.
Development of models
All candidates were randomly divided into two parts by using the “caret” package, of which 70% were assigned to a training cohort and 30% were assigned to a validation cohort. All model building was performed in the training cohort. Multivariate forward stepwise logistic regression analysis was used to select valuable variables to construct the generalized linear model (GLM). The least absolute shrinkage and selection operator (LASSO) was a well-established shrinkage method that can effectively screen meaningful variables from a large set of variables with potential multicollinearity to develop the LASSO model (LSM)[38], which was implemented by using the “glmnet” package. RF was composed of a great number of individual decision trees running as a whole[39]. These multifarious decision tree models were applied for the construction of the RF model (RFM)[40]. The importance of candidate variables was reflected by the mean decreased Gini (MDG) score.
Evaluation of models
The robustness and clinical practicability of models were assessed using the ROC curve, calibration curve, decision curve analysis (DCA), and clinical impact curve (CIC). The AUC were used to estimate the discernment of each model by using “rms” packages. The calibration curves were applied to examine the calibration ability of each model and calibrated with 1000 bootstrap samples to reduce overfitting bias. The clinical applicability of each model was informed by DCA and CIC using “rms”and “rmda” packages.
Statistical analysis
Statistical analyses were performed with R Statistical Software (version 4.1.2, https://www.rproject.org/). Continuous variables were tested for normality. Those with normality are described as the mean ± SD, while those without normality are described as the median and interquartile range.Continuous variables were compared using the student’st-test or non-parametric rank-sum test(Kruskal-Wallis test) as appropriate. Categorical variables are described as numbers (percentage) and were compared using the Chi-square test or Fisher exact test as appropriate. Correlations between candidate variables were determined by Spearman’s correlation coefficient. All statistical tests were two-tailed, andP< 0.05 was considered significant.
RESULTS
Patient demographics and characteristics
The detailed clinical characteristics of 483 patients with PH are summarized in Table 1. All participants were randomly and automatically divided into a training cohort (n= 338, 70%) and a validation cohort (n= 145, 30%). The presence of PVT was diagnosed in 200 (41.4%) cases, 135 (39.9%) cases, and 65(44.8%) cases in the overall cohort, training cohort, and verification cohort, respectively. Consistent with the results of the intergroup comparison, among the 31 candidate variables included, 14 were associated with PVT, including RBC, WBC, L, NLR, PLT, PTA, ALT, AST, EGV, SPT, DPV, PBT, PPER1, and PPER3(Figure 1B and Supplementary Table 1), which indicated that PPER1 and PPER3 were highly likely to be potential predictors of PVT.
Logistic regression analysis
Univariate and multivariate logistic regression analyses for risk factors associated with PVT in theoverall cohort are presented in Table 2. In the univariate analysis, a total of 11 variables withP< 0.05 were included in the further multivariate analysis. Finally, the following six variables were revealed to be closely associated with the occurrence of PVT: L [odds ratio (OR): 0.28, 95% confidence interval (CI):0.14-0.54,P< 0.001], EGV (OR: 0.51, 95%CI: 0.32-0.79,P= 0.003), SPT (OR: 1.22, 95%CI: 1.06-1.40,P=0.005), DPV (OR: 3.57, 95%CI: 1.86-7.03,P< 0.001), PPER1 (OR: 1.78, 95%CI: 1.24-2.62,P= 0.002), and PPER3 (OR: 1.43, 95%CI: 1.16-1.77,P< 0.001). This result demonstrated that PPER1 and PPER3 were independent risk factors for the occurrence of PVT.

Table 1 Detailed clinical characteristics of 483 patients with portal hypertension

No 159 (78.3)95 (70.4)67 (83.8)43 (66.2)Yes 44 (21.7)40 (29.6)13 (16.2)22 (33.8)De, n (%)0.4570.344 No 16 (7.88)7 (5.19)4 (5.00)6 (9.23)Yes 187 (92.1)128 (94.8)76 (95.0)59 (90.8)PLT11 (× 109/L)79.0 (61.0-106)79.0 (64.0-102)0.86674.0 (57.7-93.8)77.0 (61.0-102)0.418 PLT31 (× 109/L)103 (78.5-158)117 (85.0-164)0.13198.5 (75.5-140)112 (81.0-156)0.122 PPER11 (%)0.59 (0.34-0.88)1.18 (0.57-2.31)< 0.0010.70 (0.36-1.11)0.87 (0.64-2.03)0.002 PPER31 (%)1.15 (0.62-2.02)2.38 (1.52-3.87)< 0.0011.32 (0.79-2.04)2.29 (1.36-3.54)< 0.001 1Continuous variables are presented as the median and interquartile range (IQR).PH: Portal hypertension; PVT: Portal vein thrombosis; RBC: Red blood cells; HLB: Hemoglobin; WBC: White blood cells; N: Neutrophil count; L:Lymphocyte count; NLR: Neutrophil to lymphocyte ratio; PLT: Platelet count; PLR: Platelet to lymphocyte ratio; PT: Prothrombin time; PTA: Prothrombin activity; INR: International normalized ratio; FIB: Fibrinogen; APTT: Activated partial thromboplastin time; ALT: Alanine aminotransaminase; AST:Aspartate aminotransaminase; ALB: Serum albumin; TBIL: Total serum bilirubin; EGV: Esophageal and gastric varices; SPT: Spleen thickness; DPV:Diameter of the portal vein;PBT:Preoperative blood transfusion;De:Devascularization;PLT1:Platelet count at postoperative day 1;PLT3:Platelet count at postoperative day 3; PPER1: Platelet elevation rate at postoperative day 1; PPER3: Platelet elevation rate at postoperative day 3.
Establishment of PPER-based models
As shown in Supplementary Table 2, the following five variables strongly associated with PVT were chosen to construct the GLM: L (OR: 0.34, 95%CI: 0.14-0.77,P= 0.01), SPT (OR: 1.21, 95%CI: 1.02-1.44,P= 0.02), DPV (OR: 5.85, 95%CI: 2.57-14.05,P< 0.001), PPER1 (OR: 1.77, 95%CI: 1.13-2.82,P= 0.01), and PPER3 (OR: 1.42, 95%CI: 1.12-1.84,P= 0.005). The optimal LSM was obtained when all 31 candidate variables were shrunk to 10 through the LASSO (Figure 2A and B), which included L, NLR, PLT, PTA,AST, EGV, SPT, DPV, PPER1, and PPER3. In the RF, the total sample group had the smallest error of 24.56%, when the number of random trees was 133 (Figure 2C). A total of 133 random trees were set and passed through five iterations, and the importance scores of the candidate variables are presented in Figure 2D. Ultimately, nine variables with higher MDG scores were selected to construct the RFM.
Assessment and verification of PPER-based models
The ROC curves of the GLM, LSM, and RFM in the training cohort are shown in Figure 3A, and their AUCs were 0.83 (95%CI: 0.79-0.88), 0.84 (95%CI: 0.79-0.88), and 0.84 (95%CI: 0.79-0.88), respectively. All models had excellent calibration ability in the training cohort (Figure 3B).DCA and CIC revealed that they both conferred high clinical net benefits (Figures 3C and 4A-C).
In the validation cohort, the ROC curves of all models are presented in Figure 3D, and their AUC were 0.77 (95%CI: 0.69-0.85), 0.83 (95%CI: 0.76-0.90), and 0.78 (95%CI: 0.70-0.85), respectively. All models demonstrated highly satisfactory calibration capability and clinical functionality (Figures 3E and F and 4D-F).
Importance of PPER for models
As shown in Figure 5A, the nomogram for GLM recruited a total of five variables, including L, SPT,DPV, PPER1, and PPER3, which happened to be the intersection variables of the GLM, LSM, and RFM(Figure 5B). From this, it appeared that the aforementioned variables were significant predictors of the occurrence of PVT and they produced remarkable effects on the construction of the models. Moreover,the present study revealed that among these variables shared by the GLM, LSM, and RFM, the order of weight from high to low was DPV, PPER1, PPER3, SPT, and L (Figure 5C), which fully promulgated the predictive value of the PPER (PPER1 and PPER3) for PVT in all models.
Comparative analysis of PPER-based models
The performance of three PPER-based models in predicting PVT in different cohorts is shown in Table 3.In the overall cohort, the accuracy of the GLM, LSM, and RFM was 76.2%, 77.4%, and 77.4%respectively. In the training cohort, the accuracy of the GLM, LSM, and RFM was 79.6%, 79.0%, and78.7% respectively. In the validation cohort, the accuracy of the GLM, LSM, and RFM was 74.5%, 79.3%,and 76.6% respectively. When other metrics of the models, such as AUC, sensitivity, specificity, positive predictive value, negative predictive value, kappa values, and Brier scores, were comprehensivelyconsidered, the LSM and RFM appeared to be slightly superior to the GLM.

Table 2 Univariate and multivariate logistic regression analyses for risk factors associated with portal vein thrombosis in the overall cohort

Table 3 Performance of models for portal vein thrombosis risk prediction in different cohorts
DlSCUSSlON
Undoubtedly, PVT is a lethal complication after splenectomy in cirrhotic patients with PH[12]. Once PVT exists, there will be elevated portal venous pressure, ischemic bowel necrosis, progressive impairment of liver function, and even liver failure, which can eventually be life-threatening[41,42].Therefore, research on the optimization of early detection of individuals at high risk of PVT after splenectomy is urgently needed. In this study, we successfully constructed the PPER-based models for predicting PVT by machine/deep learning, which would be conducive to early identifying the population at high risk of PVT.
In the present study, conventional generalized linear (CGL) method and machine/deep learning(including the LASSO and RF) were applied separately to screen out the variables that greatly affected the PVT prediction. The CGL method is characterized by strong interpretability, especially when the multifactorial forward stepwise regression method is used, and therefore, it has been widely applied as the traditional method to construct a predictive model[43]. However, with the rapid progress of artificial intelligence technology, a novel prediction model based on machine/deep learning has emerged with a higher probability of accuracy, which has led some clinicians to question the value of the CGL model in the clinical application of individualized patients[44]. Coincidentally, our research results proclaimed that the performance of the LSM and RFM seemed to be slightly better than the GLM.
Interestingly, the PPER-based models contained the following five intersecting factors, namely, SPT,DPV, L, PPER1, and PPER3, which sufficiently illustrated that these were the main contributors to the higher incidence of PVT. Previous studies found that preoperative SPT and DPV were important predictors of the formation of PVT after splenectomy in patients with PH[8,45], which was highly consistent with our findings. A very reasonable explanation is that a wide preoperative DPV and SPT will lead to slow portal vein blood flow, which is closely related to postoperative thrombosis[45,46].
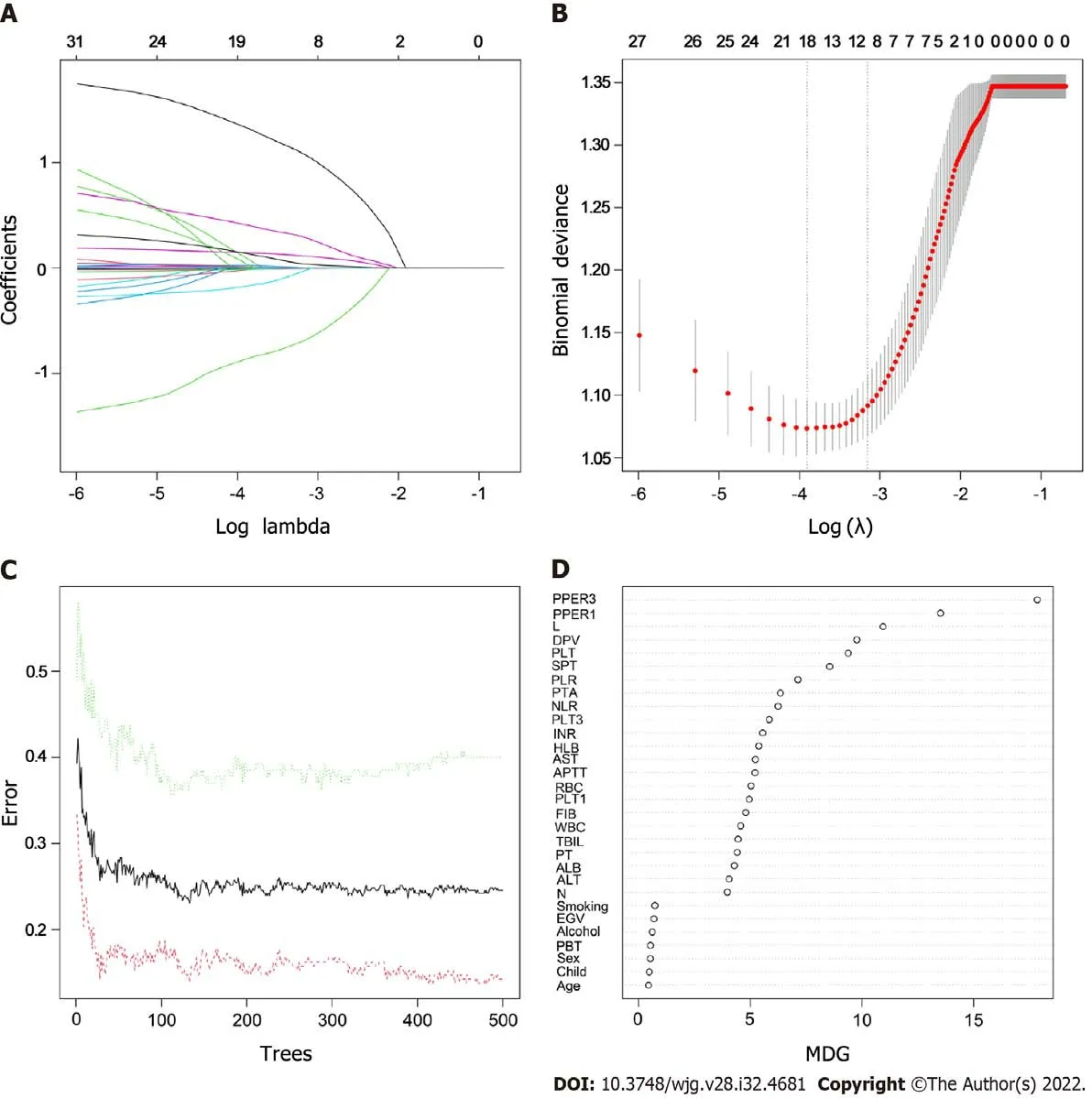
Figure 2 Features selection.A:Least absolute shrinkage and selection operator variable trace profiles of the 31 features.The 3-fold cross-validation was employed; B: Mean square error (MSE) plots of models under different lambda. The lambda corresponding to one MSE away from the minimum MSE was the optimal lambda value of 0.043, and the target variables shrunk to 10; C: Relationships between the error and number of trees. There are three lines, green representing error in the positive event group, red representing error in the negative event group, and black representing error in the total sample group; D: Importance scores of the candidate features. RBC: Red blood cells; HLB: Hemoglobin; WBC: White blood cells; N: Neutrophil count; L: Lymphocyte count; NLR: Neutrophil to lymphocyte ratio;PLT: Platelet count; PLR: Platelet to lymphocyte ratio; PT: Prothrombin time; PTA: Prothrombin activity; INR: International normalized ratio; FIB: Fibrinogen; APTT:Activated partial thromboplastin time; ALT: Alanine aminotransaminase; AST: Aspartate aminotransaminase; ALB: Serum albumin; TBIL: Total serum bilirubin; Child:Child-Pugh grade; EGV: Esophageal and gastric varices; SPT: Spleen thickness; DPV: Diameter of the portal vein; PBT: Preoperative blood transfusion; PLT1:Platelet count at postoperative day 1; PLT3: Platelet count at postoperative day 3; PPER1: Platelet elevation rate at postoperative day 1; PPER3: Platelet elevation rate at postoperative day 3; MDG: Mean decreased Gini.
In most cases, platelet, erythrocyte, and leukocyte counts rose dramatically over a short time after splenectomy in patients with PH, and the blood was hypercoagulable[8]. Therefore, previous studies suggested that preoperative low platelet and leukocyte counts were founders of the formation of PVT postoperatively[47]. This study revealed that preoperative L was an influential factor in PVT postoperatively, which coincided with the above view. Of note, the present study employed the PPER to reflect the magnitude of dynamic changes in preoperative and postoperative PLT. Subsequently, it was found that the PPER had high predictive value for the risk of PVT postoperatively, which was not addressed previously.
Stamouet al[48] reported that the median time to the formation of PVT after splenectomy in patients with PH was the 6thday (range, 3-11). Luet al[8] concluded that 49.19% of patients developed PVT within 7 d after splenectomy. Therefore, scholars routinely applied ultrasonography examination to diagnose the PVT on the 7thday after splenectomy[8,19,20]. In this study, combined with the preoperative predictors and PPER, the PPER-based models that we constructed can effectively discriminate individuals with high risk of PVT as early as the first 3 d after the operation, which was extremely critical for guiding clinicians’ treatment strategies.

Figure 3 Evaluation and validation of the postoperative platelet elevation rate-based models in the training cohort and validation cohort.A and D: The receiver operating characteristic curves of the postoperative platelet elevation rate (PPER)-based models; B and E: The calibration curves of the PPERbased models; C and F: The decision curve analysis of the PPER-based models. GLM: Generalized linear model; LSM: Least absolute shrinkage and selection operator model; RFM: Random forest model; AUC: Area under the receiver operating characteristic curve.
Currently, there is no standard preventive regimen for PVT after splenectomy in cirrhotic patients with PH[49]. Most scholars have recently advocated that the prophylactic anticoagulant therapy is administered earlier postoperatively, which will be more helpful in reducing the incidence of PVT[50,51]. However, it should be cautiously chosen because in patients with liver cirrhosis, it cannot avoid the risk of bleeding[51]. In addition, if the preventive regimens are routinely adopted for all individuals with PH after splenectomy, it is bound to raise the suspicion of overtreatment. Excitingly, in the present study, the accuracy of the PPER-based models in predicting PVT was up to 80%, which can distinguish individuals at high risk of PVT with high efficiency, and thus guide clinicians to take targeted individualized preventive measures in time.
The present study has some limitations. First, due to the retrospective nature of the study, selection bias cannot be eliminated. Second, the uncommon preoperative factors that may influence the formation of PVT, such as splenic vein diameter, spleen volume, and portal vein flow velocity[8,19], were not routinely measured in our institution and thus failed to be included in the present study. However, the SPT and DPV in this study can indirectly reflect these indicators to a certain extent[45,46]. Third, this was a monocentric study design. Although the PPER-based models demonstrated excellent performance for predicting PVT, they still lacked the verification of external cohorts. Therefore, large-scale prospective multicenter studies are warranted, which are beneficial to the popularity and application of the PPER-based models.

Figure 4 Clinical impact curves of the postoperative platelet elevation rate-based models in the training cohort and validation cohort. A and D: Clinical impact curves for the generalized linear model; B and E: Clinical impact curves for the least absolute shrinkage and selection operator model; C and F:Clinical impact curves for the random forest model.
CONCLUSlON
PPER1 and PPER3 are effective indicators for postoperative prediction of PVT. We have successfully developed the PPER-based practical models for predicting PVT, which could help clinicians identify individuals at high risk for PVT early and efficiently, and thus guide the timely intervention measures.
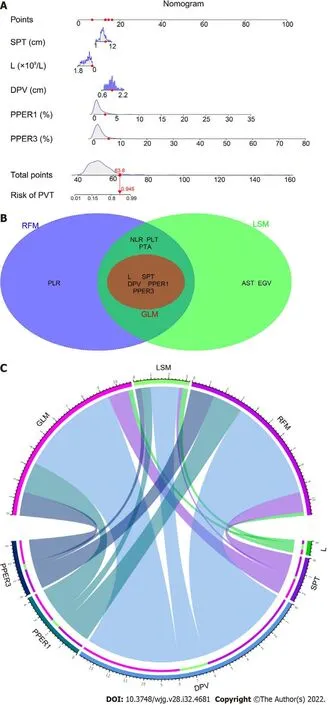
Figure 5 Nomogram for the generalized linear model and weighting of variables. A: Nomogram for the generalized linear model (GLM); B:Intersection variables among the GLM, least absolute shrinkage and selection operator model (LSM), and random forest model (RFM); C: Weights of the intersection variables in the GLM, LSM, and RFM, respectively. SPT: Spleen thickness; L: Lymphocyte count; DPV: Diameter of portal vein; PPER1 and PPER3: The first and third days for postoperative platelet elevation rate; PVT: Portal vein thrombosis; PLR: Platelet to lymphocyte ratio; NLR: Neutrophil to lymphocyte ratio; PLT: Platelet count; PTA: Prothrombin activity; EGV: Esophageal and gastric varices; AST: Aspartate aminotransaminase.
ARTlCLE HlGHLlGHTS
Research background
Patients with portal hypertension (PH) often experience rebounding rises in platelets following splenectomy. However, the value of postoperative platelet elevation rate (PPER) in predicting portal vein thrombosis (PVT) is unknown.
Research motivation
PVT is a potentially fatal complication after splenectomy for patients with PH, and the probability of PVT has been reported to be nearly 50%. Therefore, there is an imperious demand for effective diagnostic methods to early and rapidly identify individuals at high risk of PVT after splenectomy to further help clinicians take intervention measures as soon as possible.
Research objectives
We aimed to investigate the predictive value of PPER for PVT and establish PPER-based practical prediction models to early identify individuals at high risk of PVT after splenectomy.
Research methods
We retrospectively reviewed 483 patients with PH related to hepatitis B virus who underwent splenectomy between July 2011 and September 2018, and they were randomized into either a training (n= 338) or a validation (n= 145) cohort. The generalized linear (GL) method, least absolute shrinkage and selection operator (LASSO), and random forest (RF) were used to construct models. The receiver operating characteristic (ROC) curves, calibration curve, decision curve analysis (DCA), and clinical impact curve (CIC) were used to evaluate the robustness and clinical practicability of the GL model(GLM), LASSO model (LSM), and RF model (RFM).
Research results
PPER at the first (PPER1) and third (PPER3) days were strongly associated with PVT [odds ratio (OR):1.78, 95% confidence interval (CI): 1.24-2.62,P= 0.002; OR: 1.43, 95%CI: 1.16-1.77,P< 0.001, respectively]in the multivariate logistic regression analysis. The areas under ROC curves of the GLM, LSM, and RFM in the training cohort were 0.83 (95%CI: 0.79-0.88), 0.84 (95%CI: 0.79-0.88), and 0.84 (95%CI: 0.79-0.88),respectively; and were 0.77 (95%CI: 0.69-0.85), 0.83 (95%CI: 0.76-0.90), and 0.78 (95%CI: 0.70-0.85) in the validation cohort, respectively. The calibration curves showed satisfactory agreement between prediction by models and actual observation. DCA and CIC indicated that all models conferred high clinical net benefit.
Research conclusions
PPER1 and PPER3 are effective indicators for predicting PVT. We have successfully developed the PPER-based practical models to accurately predict PVT, which could conveniently help clinicians rapidly differentiate individuals at high risk of PVT, and further guide the adoption of timely interventions.
Research perspectives
According to our experience, patients with a more remarkable increase in platelet count in the first 3 d after operation have a higher probability of PVT, which should be prioritized for prophylactic anticoagulation.
FOOTNOTES
Author contributions:All authors contributed to the study; Li J wrote the manuscript, and collected and analysed the data; Wu QQ collected the data, and contributed to the follow-up results; Zhu RH, Lv X, and Wang WQ collected the data and performed the analysis; Wang JL contributed to the data; Liang BY and Huang ZY provided the resources and supervision; Zhang EL contributed to writing the manuscript, and drafting the conception and design; all authors read and approved the final manuscript.
Supported byNational Natural Science Foundation of China, No. 81902839; and Hubei Provincial Special Grants for Scientific and Technical Innovation, No. 2021BCA115.
lnstitutional review board statement:The study was approved by the Medical Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (No. 2022-LSZ (S066)).
lnformed consent statement:Written informed consent from the patients was waived due to the retrospective nature of this study.
Conflict-of-interest statement:All authors declare no conflicts of interest related to this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Jian Li 0000-0001-9025-4968; Qi-Qi Wu 0000-0002-5556-4394; Rong-Hua Zhu 0000-0002-8588-7493; Xing Lv 0000-0002-8363-6383; Wen-Qiang Wang 0000-0002-9648-5481; Jin-Lin Wang 0000-0003-0073-4197; Zhi-Yong Huang 0000-0002-2239-0674; Er-Lei Zhang 0000-0002-7251-0275.
S-Editor:Fan JR
L-Editor:Wang TQ
P-Editor:Chen YX
 World Journal of Gastroenterology2022年32期
World Journal of Gastroenterology2022年32期
- World Journal of Gastroenterology的其它文章
- The mechanism of Yinchenhao decoction in treating obstructivejaundice-induced liver injury based on Nrf2 signaling pathway
- Anoctamin 5 regulates the cell cycle and affects prognosis in gastric cancer
- Effects of Granule Dendrobii on chronic atrophic gastritis induced by N-methyl-N'-nitro-N-nitrosoguanidine in rats
- Sirolimus increases the anti-cancer effect of Huai Er by regulating hypoxia inducible factor-1α-mediated glycolysis in hepatocellular carcinoma
- lnternational patterns in incidence and mortality trends of pancreatic cancer in the last three decades: A joinpoint regression analysis
- Expanding beyond endoscopy: A review of non-invasive modalities in Barrett’s esophagus screening and surveillance