
Clinical effect of governor meridian moxibustion on treatment of lumbar disc protrusion: A meta analysis
2022-09-05 00:59:56ShengYueWenMinZhangGuoQingDuJianPangXunLinNingYangGaoYueLongCaoYuYunWuYuXinZhengBoChenHongShengZhan
Journal of Hainan Medical College 2022年13期
Sheng-Yue Wen, Min Zhang, Guo-Qing Du, Jian Pang, Xun Lin, Ning-Yang Gao, Yue-Long Cao, Yu-Yun Wu, Yu-Xin Zheng, Bo Chen, Hong-Sheng Zhan
Shi's Traumatology Medical Center, Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
Keywords:Governor meridian moxibustion Lumbar disc protrusion Meta-analysis Randomized controlled trial
ABSTRACT Objective:To explore the clinical effect of governor meridian moxibustion on lumbar intervertebral disc protrusion. Methods:Randomized controlled trials on treatment of lumbar intervertebral disc protrusion with governor meridian moxibustion and combined governor meridian moxibustion were retrieved from CNKI,VIP,Wan Fang Data,CBM,Web of ScienceTM Core Collection,EBSCO Medline,PubMed,OVID,the Cochrane Library,and other databases.The time was from the inception of the database until October 2021. The studies were screened according to the inclusion and exclusion criteria,extracted,and evaluated for quality assessment. The data were analyzed with Review Manager 5.3 software. Results:A total of 24 randomized controlled trials(2 379 cases in total)were included. Meta-analysis results showed that compared with control groups such as acupuncture,electroacupuncture,and massage,the governor meridian treatment improved the clinical efficacy[RR=1.17,95%CI(1.13,1.20),P<0.001],relieved patients' pain[MD= -1.56,95%CI(-1.89,-1.22),P<0.001],and improved patients’dysfunction to a certain extent[MD=4.84,95%CI(3.87,5.82),P<0.001]. Funnel plot analysis showed that the included literature may be potentially biased in publication.Conclusion:Governor meridian moxibustion has a significant effect on the treatment of lumbar disc protrusion and is worthy of widespread use. However,given the small number of highquality literature included in the study,the small sample size,and the short follow-up time,highquality randomized controlled trials are needed to further study the long-term therapeutic effect of governor meridian moxibustion.
1. Introduction
Lumbar disc herniation (LDH) is a degenerative degeneration of the lumbar disc that, under the action of external forces, leads to partial or complete rupture of the fibrous annulus within the disc and protrusion or prolapse, either alone or together with the nucleus pulposus and cartilage endplates, into the spinal canal, irritating or compressing the corresponding nerves and/or nerve roots, thus causing pain in the low back, unilateral or bilateral lower limb [1].The incidence of lumbar disc herniation mostly occurs in people in the age range of 40 to 60 years, with the incidence gradually increasing with age in women and gradually decreasing in men[2]. In Chinese medicine, lumbar disc herniation is classified as"paralysis", of which the occurrence of the disease is most closely related to the Directing Vessel. The Governor's Vessel runs along the midline of the back and is related to the spine in terms of circulation and function, so spine-related diseases are first treated from the Governor's Vessel. Moxibustion, also known as long snake moxibustion, pavement moxibustion, and fire dragon moxibustion,is often applied to the Governor's Vessel and is mostly used to treat spine-related diseases [3]such as the neck, waist, and back. It has a wide area of application, large fire power of moxa cone, and strong ability of warming and tonifying the Governor's Vessel, warming the qi and blood, balancing yin and yang, opening paralysis, and activating blood circulation to remove blood stasis. It is suitable for the treatment of all the symptoms of the Governor's Vessel[4],persistent [5]paralysis and chronic deficiency diseases[6]. Initially,moxibustion was used to treat ankylosing spondylitis, [7]but with the rapid development of medicine, it has gradually been applied to other diseases.[8, 9] In recent years, although there are some treatments for lumbar spondylitis, there are also some treatments for chronic deficiency diseases. In recent years, although there have been clinical studies and literature reports on the treatment of lumbar disc herniation by dou moxibustion, there is still a lack of systematic and standardized evidence-based medical research. The aim was to provide more in-depth evidence-based medical evidence for the treatment of lumbar disc herniation by collecting randomized controlled trials on the treatment of lumbar disc herniation in China and abroad, so as to better guide the clinical treatment of this disease.
2. Information and methodology
2.1 Inclusion and exclusion criteria
2.1.1 Study type Randomized controlled1ed trial (RCT)
2.1.2 Study subjectsPatients with lumbar intervertebral disc herniation were diagnosed according to any of the four criteria: "Diagnostic and Efficacy Criteria for Chinese Medicine Evidence" [13][10]or "Shanghai Diagnostic and Treatment Practice for Chinese Medicine Evidence"[11]or "Diagnostic and Treatment Practice for Orthopedic Evidence"[12]or "Guidelines for Clinical Research on New Chinese Medicines"promulgated by the State Administration of Traditional Chinese Medicine; the age, gender and source of disease duration of the included patients were not limited.
2.1.3 Interventions Treatment group
dou moxibustion or dou moxibustion combined with other therapies; control group: Chinese medicine treatment without dou moxibustion therapy or other therapies.
2.1.4 Ending indicators
2.1.4.1 Clinical efficacy and efficiencyEvaluated with reference to the "Diagnostic and Efficacy Standards for Chinese Medicine Evidence" issued by the State Administration of Traditional Chinese Medicine[10]. Cured: disappearance of low back pain and lower limb radiological symptoms, free movement of the spine, straight leg elevation test ≥70°, no effect on daily work and life; effective: significant reduction of low back pain,disappearance of lower limb radiological symptoms, improvement of spinal movement, straight leg elevation test within 60°~70°,able to carry out daily work and life; effective: partial disappearance of low back pain symptoms, able to get out of bed and walk upright but with mild limitation of movement, straight leg elevation 30°~45°. Straight leg elevation 30°~45°. Ineffective: no significant improvement in symptoms and signs of low back pain after treatment, seriously affecting daily life and work, straight leg elevation test <30°. The number of "cured cases", "effective cases"and "effective cases" were combined into the number of effective cases, and the total effective rate = the number of effective cases/total number of cases×100%.
2.1.4.2 Visual Analogue Scale (VAS) score [14]VAS score is used to evaluate the patient's pain, where the patient marks the value that best represents the intensity of their pain on a scale of 10 cm in length, with values ranging from 0 (no pain) to 10(most severe pain), with higher values indicating more severe pain.
2.1.4.3 Japanese Orthopaedic
Association Scores (JOA) for lumbar spine assessment and treatment [15] , is used to assess the neurological function of lumbar spine disorders, and the score consists of four items: subjective symptoms, clinical signs, daily activities, and bladder function, with a total score of 29 points, and the degree of recovery of lumbar spine neurological function is positively correlated with the high score.
2.1.4.4 Oswestry Disability Index (ODI) [16]
ODI can better reflect the patient's condition and functional changes, the scale is mainly divided into pain (intensity of pain,the degree of pain interference with sleep), single function (lifting,walking, sitting, standing) and personal integrated function (daily living ability, Sexual life, social life, travel), each with a score of 0-5,with higher scores indicating more severe functional impairment.The higher the score, the more severe the dysfunction.
2.1.5 Exclusion criteria
① duplicate publications; ② original literature without control groups or unreasonable control group settings; ③ literature related to animal experiments, case reports, review literature, expert treatment experience type of literature; ④ included original literature with unclear content effect indicators; ⑤ original data were not adequately reported.
2.2 Search Strategy
2.2.1 Databases
Computer searches of China Knowledge Network (CNKI),Vipers (VIP), WanFang (WanFang Data), China Biomedical Abstracts Database (CBM), Web of ScienceTMCore Collection,Ebsco Medline, OVID, PubMed, The Cochrane Library, and other databases to collect relevant randomized controlled trials (RCTs) of Dude Moxibustion and Dude Moxibustion combination therapy for lumbar disc herniation. The search was limited to the period from the creation of the database to October 2021.
2.2.2 Search terms
The Chinese search terms were "dou moxibustion", "pave moxibustion", "spacer moxibustion", "spacer ginger moxibustion ","long snake moxibustion", "long dragon moxibustion", "fire dragon
moxibustion" and "lumbar intervertebral disc herniation ", "lumbar disc bulge", "lumbar disc prolapse", "lumbar disc herniation","intervertebral disc Fibrotic ring rupture", "lumbar protrusion","lumbar paralysis", etc. The English search terms are "Sciatica","Low Back Pain", "Lumbar Disc Herniation", "Intervertebral Disc Herniation", and "Intervertebral Disc Herniation". "Intervertebral Disc Degenerations", and "Moxibustion", "Du Moxibustion ", "Snake Moxibustion", "Dragon moxibustion", "Fire dragon moxibustion",the language of the search is not limited. According to the different characteristics of different databases, the corresponding advanced search was used, and a combination of subject terms and free words was adopted to collect all the relevant literature on randomized controlled trials or clinical controlled trials on the clinical efficacy of dou moxibustion in the treatment of lumbar disc herniation at home and abroad.
2.3 Risk of bias evaluation of included studies
RCTs included in the study were evaluated for risk of bias according to the risk of bias assessment tool recommended in the Cochrane systematic appraisal manual version[17] 5.1.0. The evaluation included (i) the correctness of the randomization method;(ii) whether allocation concealment was used correctly; (iii) whether blinding was used and who was blinded; (iv) whether the outcome data were complete and whether there were any missing visits or withdrawals; (v) whether the study results were reported selectively;and (vi) other sources of bias.
2.4 Statistical analysis
Statistical analysis was performed using Review Manage 5.3[18]provided by the Cochrane Collaboration Network. The results of the multiple included studies were first tested for heterogeneity using the chi-square test, while theI^2quantitative analysis of heterogeneity.If the heterogeneity of included studies was low (I^2≤50%), a fixed effect model was used; if the heterogeneity of the included studies was high (I^2 If the heterogeneity of the included studies was low ( >50%), the random effect model was used to find the source of heterogeneity and to deal with the factors that might lead to clinical heterogeneity by subgroup analysis or sensitivity analysis or descriptive analysis. The outcome indicators included in this Metaanalysis used relative risk (RR) when combining statistics if they were dichotomous variables, and mean difference (MD) as a statistic if they were continuous variables, while 95% confidence interval(CI) was calculated. The results of the Meta-analysis were displayed in the form of a forest plot, and an inverted funnel plot (funnel plot)was used to determine whether there was a potential publication bias and the magnitude of the bias. All statistical indicators were twosided, and differences were considered statistically significant if P <0.05.
3. Results
3.1 Literature search results
In this study, 480 documents were retrieved, 219 documents were removed after checking, 220 documents that did not meet the inclusion criteria were removed by browsing the titles and abstracts,the remaining 41 documents were read for full-text re-screening, 18 documents with incompatible outcome indicators or incomplete data were removed, and finally 24 documents met the inclusion criteria for a total of 2379 patients. The literature screening process and results are shown in Figure 1
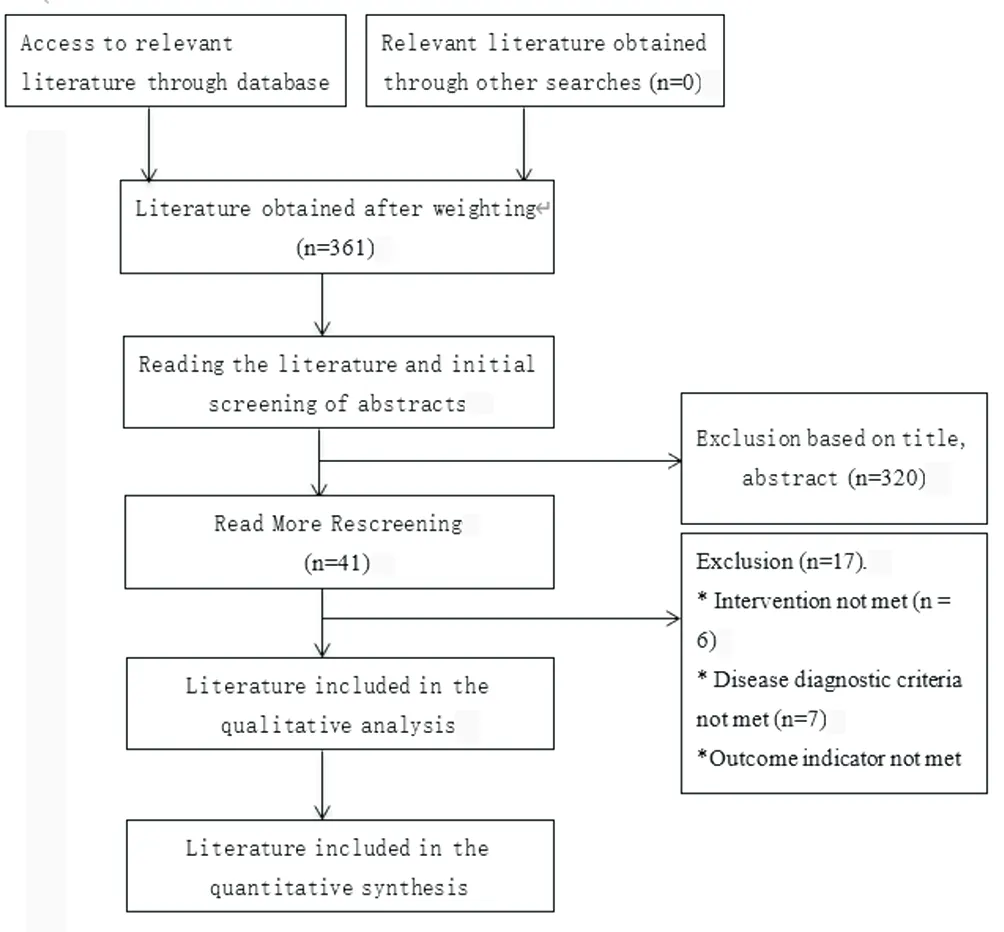
Figure 1 Study Selection Flow Chart.
3.2 Basic characteristics of included studies and evaluation of risk of bias
The 24 included studies[19-42] , involved a total of 2379 cases;published between 2013 and 2021; the mean age of the subjects was 48 years; the duration of the disease ranged from 3 months to 7 years; the treatment group was treated with doujinshi and the control group was treated with traction, moxibustion, massage, tui na,acupuncture, herbs, warm acupuncture, gua sha, and physiotherapy;and the duration of treatment ranged from 1 week to 12 weeks. The 24 included studies[19-42] all used clinical efficiency as an index for determining efficacy, nine studies[19, 21, 25, 28, 32, 34, 36, 38, 41] reported the JOA score, 14 studies[19-23, 25, 27, 29, 30, 32, 33, 35, 38, 42] used the VAS score, and 2 studies[30, 35] used the ODI score for evaluation.The basic characteristics of the included studies are shown in Table 1.
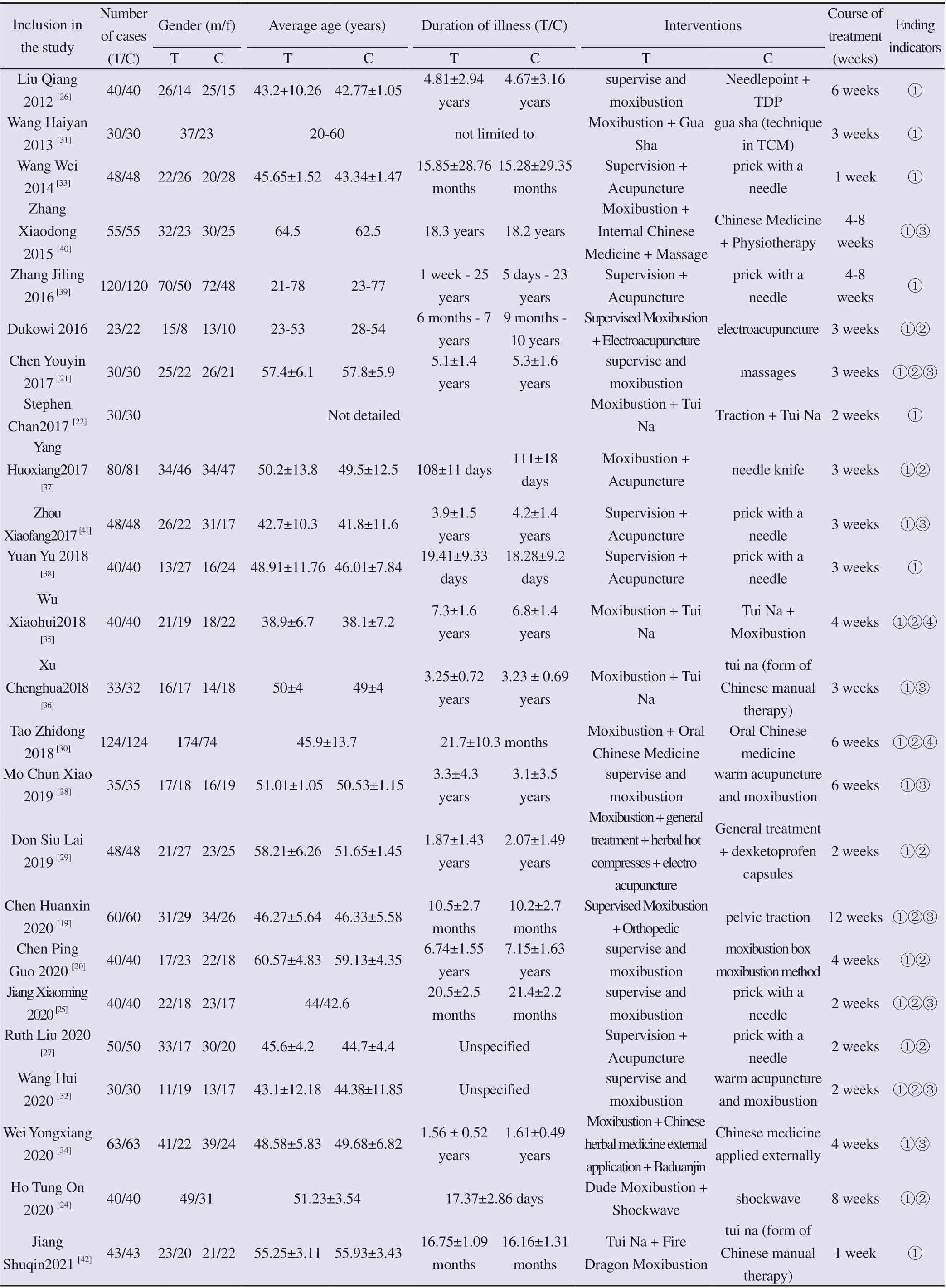
Table 1 Characteristics of the included RCTs
Twelve of the 24 RCTs included in the trial[19, 20, 22, 24-27, 29,30, 32, 37, 38] used a random number table method, 11 trials[21,28, 31, 33-35, 39-41] mentioned randomization but did not specify the randomization method, and 1 trial [23]used single and double numbers at the time of consultation for grouping; only 1 trial[21] used a double-blind method, and the remaining trials did not mention whether they used a blinded method and who was blinded; all trials did not specify whether they performed concealment of the random assignment scheme, and other biases had a high risk of bias. The results of the risk of bias evaluation are shown in Figure 2.
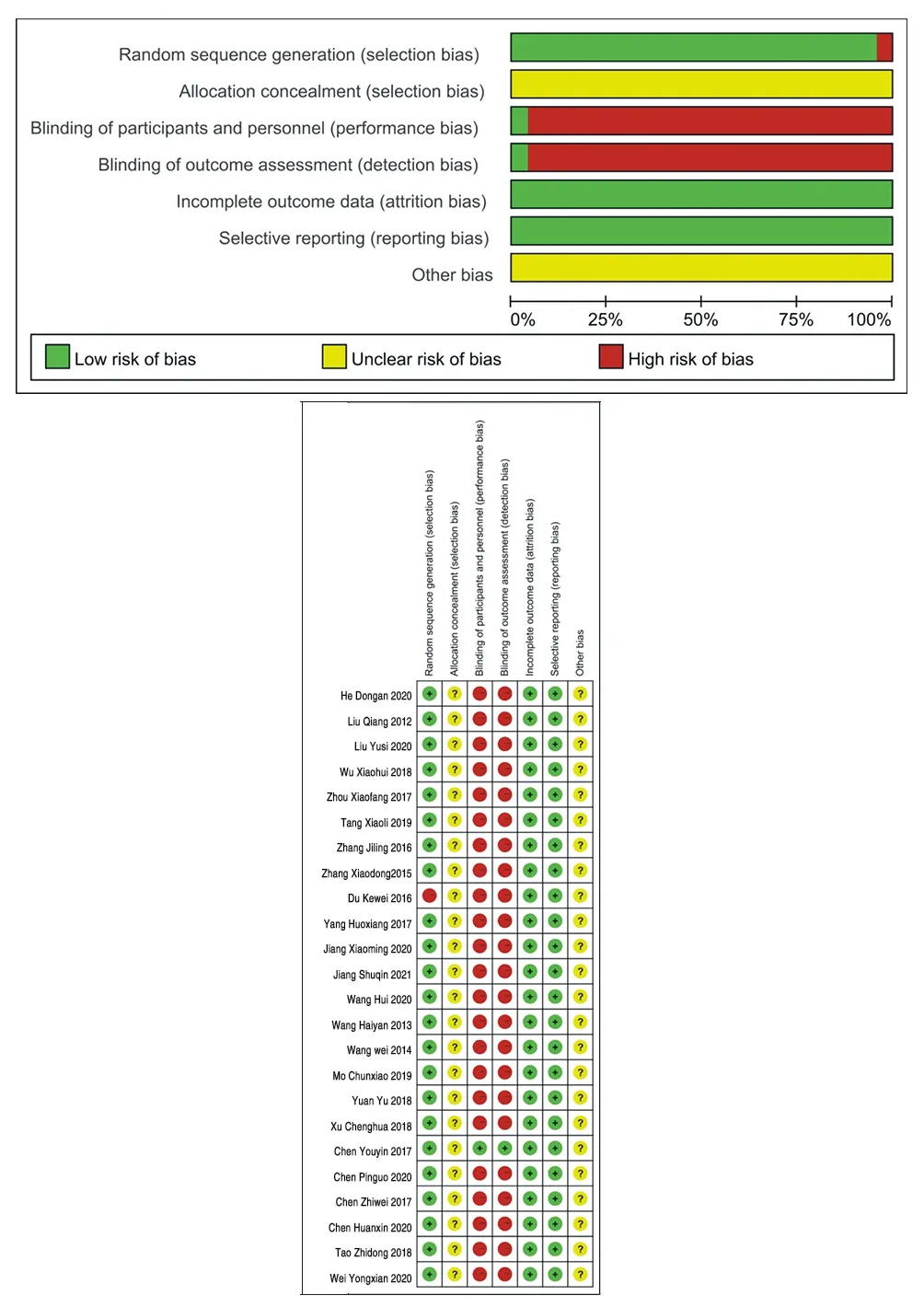
Figure 2 Percentage of included study that produced the risks of bias
3.3 Meta-analysis results
3.3.1 Results of total clinical effectiveness
Twenty-four RCT studies[19-42] A total of 2379 patients reported data on the total effective rate of treatment with dou moxibustion versus traction, moxibustion, massage, tui na, acupuncture, Chinese herbal medicine, warm acupuncture, gua sha, and acupuncture control groups, with 1190 in the test group and 1189 in the control group. The results of the fixed-effects model showed that treatment with dou moxibustion increased the clinical effectiveness rate compared with acupuncture, tui na, herbal tonics, gua sha,moxibustion, and electroacupuncture ([RR=1.17, 95% CI (1.17,1.20), P<0.00001]) with low heterogeneity in the included studies(I²=5%). This study demonstrated that treatment with doublestick moxibustion improved the clinical symptoms of patients with lumbar disc herniation. For details, see Figure 3-1.
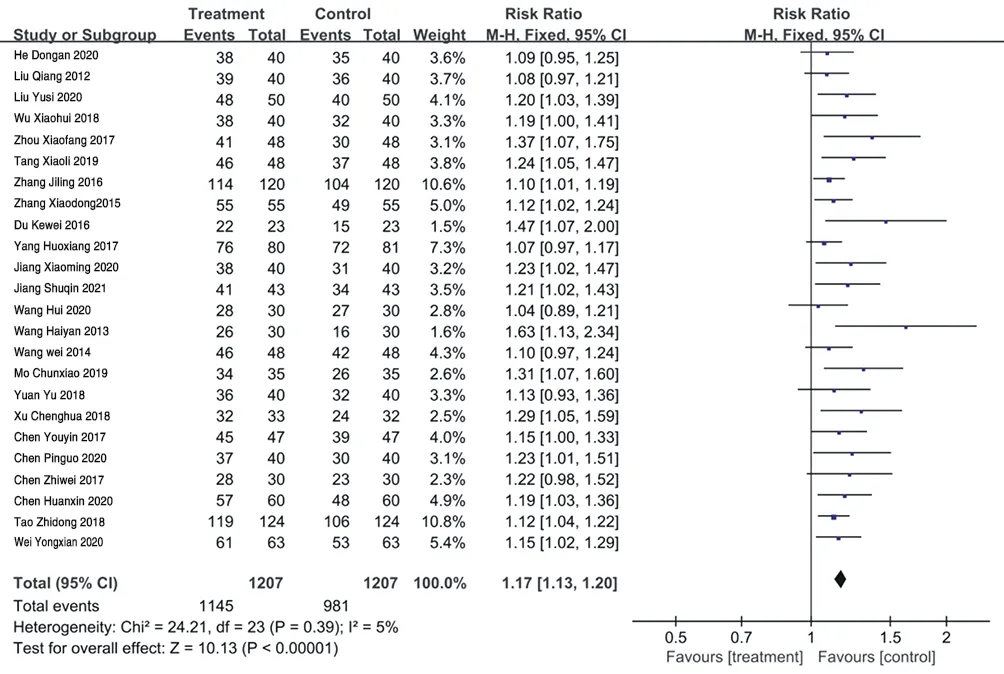
Figure 3-1 Forest map of meta-analysis of Total clinical efficiency
3.3.2 Visual pain simulation score (VAS) based analysis
Fourteen RCT studies[19-23, 25, 27, 29, 30, 32, 33, 35, 38, 42] (n=1326)reported on the improvement of pain in patients with lumbar disc herniation by supervised moxibustion therapy, and there was statistical heterogeneity among the findings (I²=93%; P<0.00001),so a random-effects model was chosen to combine the statistics;the results showed that VAS scores were lower in the treatment group than in the control group [MD=-1.56, 95% CI (-1.89, - 1.22),P<0.00001], suggesting that the effect of doujian moxibustion treatment in reducing pain was superior to traction, massage,moxibustion, warm acupuncture, acupuncture, and herbal soup treatment, as detailed in Figure 3-2.
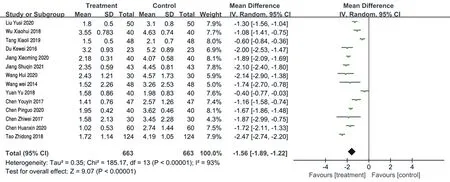
Figure 3-2 Forest map of meta-analysis of VAS
3.3.3 Analysis based on the Japanese Orthopaedic Association lower back pain score (functional score of the JOA scale)
Nine RCT studies[19, 21, 25, 28, 32, 34, 36, 38, 41] (n=791) recorded changes in JOA scores before and after treatment, with statistical heterogeneity between the nine studies (I²=85%; P<0.00001), so Meta-analysis was performed using a random-effects model, and the results suggested that the efficacy of the Dude Moxibustion treatment group in improving patients' JOA scores was significantly superior [MD=4.84, 95% CI (3.87 , 5.82), P<0.00001], as shown in Figure 3-3. compared with massage, warm acupuncture, and acupuncture, this indicates the definite efficacy of Dude Moxibustion therapy in promoting the degree of neurological recovery in patients with lumbar disc herniation.

Figure 3-3 Forest map of meta-analysis of JOA
3.3.4 Analysis based on Oswestry Dysfunction IndexTwo RCT studies[30, 35] compared the ODI scores after treatment,but the scoring criteria for the outcome indicators in these two studies were different and the data could not be combined, so descriptive analyses were performed. One of the studies, Tao Zhidong's study, [30]compared the changes in ODI scores after dou moxibustion combined with Chinese herbal medicine treatment and Chinese herbal medicine alone for lumbar disc herniation, and the results suggested that dou moxibustion combined with Chinese herbal medicine had an advantage in improving patients' lumbar spine function compared with pure Chinese herbal medicine [MD=-11.53, 95% CI [-13.05, -10.01), P<0.00001], and Wu Xiaohui's study The [35]results showed that doujian moxibustion combined with tui na treatment was significantly superior to the tui na combined with moxibustion group in terms of improving patients' functional impairment index. These two studies suggest that this advantage needs to be supported by a larger sample size. (See Figures 3-4).

Figure 3-4 Forest map of meta-analysis of ODI
3.3.5 Adverse eventsNone of the 24 RCTs included had any adverse events, indicating a good safety profile for supervised moxibustion therapy.
3.4 Publication bias
Funnel plot analysis of the 24 randomized controlled trials included shows asymmetric graphs (see Figure 4), suggesting that the potential publication bias in this study may be related to the small sample sizes of some of the trials and differences in quality across studies, and therefore the need to improve the quality of studies and expand study sample sizes to reduce the incidence of bias.
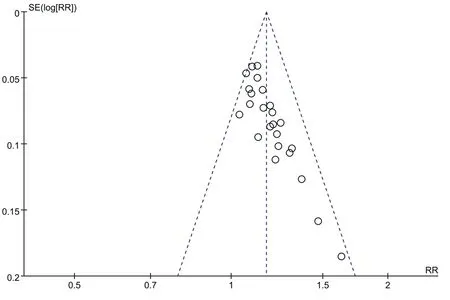
Figure 4 Publish bias funnel plots
4. Discussion
A total of 24 randomized controlled trials involving 2379 patients with lumbar disc herniation were included in this study. The results of the study showed that, compared with acupuncture, moxibustion,acupuncture, tui na, and traction treatment, Dude Moxibustion therapy has higher clinical efficacy; can promote nerve function repair; can effectively reduce patients' pain and lumbar spine dysfunction; can significantly improve patients' clinical symptoms and signs such as low back pain and lower limb radiating pain,thus improving patients' quality of life level; in terms of safety,none of the included studies mentioned that during the use of Dude Moxibustion In terms of safety, none of the included studies mentioned the occurrence of adverse events such as burns and skin allergies during the treatment.
In Chinese medicine, lumbar disc herniation belongs to the category of "lumbago" and "paralysis", which was first mentioned in "Su Wen - Pulse Essentials", "The waist is the house of the kidney, if it cannot be shaken, the kidney will be exhausted. "The main cause of the disease in Chinese medicine is that the body suffers from trauma or kidney deficiency, coupled with wind, cold, dampness and other evil attacking the meridians, fighting with qi and blood, resulting in blockage of the meridians, not pass is pain, so in clinical patients can be seen in the back pain, turn side unfavorable accompanied by lower limb discomfort and other symptoms. Modern medicine believes that the pathogenesis of lumbar disc herniation is mainly due to age, various mechanical injuries, cellular metabolic disorders,the body's autoimmune response and inflammatory chemical stimulation[43], and various mechanisms interact with each other,interlinking and acting together to accelerate the degeneration of the intervertebral disc, resulting in the protrusion of the disc.
Lumbar intervertebral disc herniation is a common disease in the orthopedic clinic, among the many treatment methods, nonsurgical therapy has the advantages of low price, high safety, small trauma, etc., and often becomes the preferred clinical method; and moxibustion therapy shows its unique advantages[44] due to its simple operation, low toxic side effects, significant effect of warming
Yang, and the action in the middle of the spine, a wide range of indications, and easy to be accepted by the majority of patients. It is easy for patients to accept. Therefore, moxibustion treatment can stimulate the body's Yang energy, regulate the meridians and internal organs, improve the body's positive energy, and drive away the cold evil in the body; moxibustion can also regulate the body's immune system and inflammatory indicators, inhibit the production of[45] IL-1β, TNF-α and other inflammatory factors; increase the expression of the[46] body's immune cell ratio CD+4CD+25Treg, CD+4Thl,and regulate the body's immune balance; delay the rise of bone destruction indicators In addition, moxibustion through the moxa velvet to warm the meridians, the role of moving Qi and blood,combined with the heat penetration of moxibustion, coupled with ginger rich in ginger phenolic ginger spicy elements to stimulate the skin, with local vasodilatation, improve blood circulation, promote metabolism, and at the same time there is the role of the meridians of the Governor to warm the internal organs, the transmission of essence [48]. In conclusion, the use of governor moxibustion treatment can play a comprehensive role of the governor vein,moxibustion and ginger to effectively improve the symptoms of patients with lumbar intervertebral disc herniation, and it is worth promoting the application in clinical practice.
The limitations of this study are: ①In evaluating the efficacy,most studies use subjective indicators such as VAS score, JOA score, and ODI, which makes the efficacy somewhat subjective;②Du moxibustion is an external treatment method, so it is difficult to do a blinded study, which is prone to implementation bias and measurement bias; in addition, du moxibustion is a characteristic therapy of Chinese medicine, so the literature included after screening is all in Chinese, which is prone to publication bias; (iii)the number of cases of adverse reactions reported in this study was small, and the sample size of the included studies was small and of average quality, with a certain risk of bias; (iv) the follow-up time of the randomized controlled trials included in this study was short, and the long-term efficacy of dou moxibustion in the treatment of lumbar disc herniation needs to be further clarified.
The above evidence suggests that the use of doujiao therapy is effective in the treatment of lumbar disc herniation and has significant significance in reducing patients' pain and improving other clinical signs and symptoms, which can provide a new reference basis for clinical treatment, but this conclusion still needs to be strengthened by clinical data from more scientifically sound and strictly standardized randomized controlled trials to verify the long-term effects of doujiao in the treatment of lumbar disc herniation.
Author’s Contribution
Shengyue Wen: first author, collected relevant literature for analysis, paper writing and revision.
Bo Chen: Corresponding author, supervised the writing of the paper and suggested revisions.Cao Yuelong, Zheng Yuxin, Zhan Hongsheng: Literature search screening and data collection and analysis.Zhang M, Du G, Pang J: Conducting a literature quality evaluation.The rest of the authors: revising the format of the paper
Conflict of interest The content of the article does not involve a relevant conflict of interest and the study did not involve direct or indirect financial or beneficial sponsorship by any manufacturer and related employers or other economic organizations.
 Journal of Hainan Medical College2022年13期
Journal of Hainan Medical College2022年13期
- Journal of Hainan Medical College的其它文章
- Study on key genes and pathways of myocardial fibrosis and prediction of effective traditional Chinese medicine
- Study on the clinical correlation between serum total IgE level and peripheral blood eosinophil count in patients with eczema
- Effect of Qingguangan Ⅱ on Rho/ROCK associated factors in the retina of DBA/2J mice
- Study on the correlation between Serum HDAC3, HMGB-1 and nonvalvular atrial fibrillation
- Effect of HK3 on immune invasion, proliferation and invasion of colon cancer cells
- Canagliflozin attenuates hypertension induced myocardial hypertrophy and fibrosis via RAS and TGF-β1/Smad pathway