
Social skills and psychopathology are associated with autonomic function in children:a cross-sectional observational study
2022-08-27 07:39ElisaCainelliLucaVedovelliDanieleBottigliengoDarioBoschieroAgneseSuppiej
中国神经再生研究(英文版) 2022年4期
Elisa Cainelli ,Luca Vedovelli ,Daniele Bottigliengo ,Dario Boschiero ,Agnese Suppiej
Abstract In recent years,the increase of psychopathological disorders in the population has become a health emergency,leading to a great effort to understand psychological vulnerability mechanisms.In this scenario,the role of the autonomic nervous system (ANS) has become increasingly important.This study investigated the association between ANS,social skills,and psychopathological functioning in children.As an ANS status proxy,we measured heart rate variability (HRV).Infants admitted to the neonatal intensive care unit of the University Hospital of Padova because of preterm birth or neonatal hypoxic-ischemic encephalopathy were sequentially recruited from January 2011 to June 2013 and followed long-term up to school age in this cross-sectional observational study.We recorded 5 minutes of HRV immediately before measuring performance in social abilities tasks (affect recognition and theory of mind,NEPSY-II) in 50 children (mean age 7.4 ± 1.4 years)with and without risk factors for developing neuropsychiatric disorders due to pre-/perinatal insults without major sequelae.Children also completed extensive cognitive,neuropsychological,and psychosocial assessment.Parents were assessed with psychopathological interviews and a questionnaire (CBCL 6-18).Analysis in a robust Bayesian framework was used to unearth dependencies between HRV,social skills,and psychopathological functioning.Social task scores were associated with HRV components,with high frequency the most consistent.HRV bands were also associated with the psychopathological questionnaire.Only normalized HRV high frequency was able to distinguish impaired children in the affect recognition task.Our data suggest that ANS may be implicated in social cognition both in typical and atypical developmental conditions and that HRV has cross-disease sensitivity.We suggest that HRV parameters may reflect a neurobiological vulnerability to psychopathology.The study was approved by the Ethics Committee of the University Hospital of Padova (Comitato Etico per la Sperimentazione,Azienda Opedaliera di Padova,approval No.1693P).
Key Words:affect recognition;autonomic nervous system;children;hypoxic-ischemic encephalopathy;impairment;neonatal;prematurity;psychopathology;recovery;theory of mind
Introduction
In 1996,the Global Burden of Disease revealed a health emergency around psychiatric disorders,which account for more than a quarter of all disabilities,a rate eight times greater than coronary heart disease and 20 times higher than cancer (Murray and Lopez,1996).Unfortunately,the understanding of etiopathogenesis and the role of environmental triggers remains rudimentary.
Most studies point to the importance of genetic,obstetrical,and traumatic factors (Burnett et al.,2011;Dorrington et al.,2014;Faa et al.,2016;Hartman and Belsky,2018),exerting their effects via inflammatory and epigenetic processes and determining unpredictable cascade effects.The consequences frequently only manifest after several years and with differing grades of severity,mostly depending on the stage of nervous system development at the time of the insult (Haensel et al.,2008;Murgatroyd and Spengler,2011).
The most crucial periods in which neuropsychiatric vulnerability is established are gestation and the early postnatal weeks (Faa et al.,2016),a phase of enormous quantitative and qualitative changes in the nervous system.In this period,neurodevelopment and later proficiency were programmed.Unsurprisingly,a high incidence of disorders affects children who experienced insults during this period,such as perinatal asphyxia or prematurity,also for those who suffered from only mild conditions (Cainelli et al.,2018).Furthermore,late-emerging minor impairments are increasing,different from the incidence of mortality and severe morbidity reduced thanks to the advancements in pre-/perinatal medicine (Marlow et al.,2005;Azzopardi et al.,2014).
To understand the underlying mechanism of these complex dynamics,accumulating evidence supports the contribution of the autonomic nervous system (ANS) and its interplay with the central nervous system.This hypothesis was first proposed by Porges (Porges,1995;Porges and Furman,2011),who theorized that the ANS has evolved to support social behavior through the recently developed myelinated branch of the vagus cranial nerve.Thayer et al.(2009) further expanded the theory,proposing that prefrontal-subcortical inhibitory circuits are crucial for self-regulation.From these original theories,the knowledge about this association has been further explored.The substrate underlying how physical and emotional experiences shape behavior,emotional,and neuropsychiatric health is the complex interplay between the central ANS (brainstem) and the limbic system.When a behavioral response or stress triggers the limbic system,ANS provides the physiologic output of emotions,with effects on heart,respiratory rate,and blood pressure (Mulkey and du Plessis,2019).
The empirical studies investigating the association between ANS development and neuropsychiatric health remain scarce,and most contributions offer only speculative or indirect findings.Recently,some experimental studies have investigated the mechanisms by which the ANS contributes to cognitive functions,such as executive function (Stenfors et al.,2016),using the non-invasive measure of heart rate variability(HRV;Shaffer and Ginsberg,2017),but studies remain still scarce (Christiansen et al.,2019;Krause-Utz et al.,2019;Morris et al.,2020).
In this study,we aimed to test the hypothesis of an association between HRV,as a proxy of ANS,with social cognition and emotional competencies (here,“social skills”),as measured with standardized tests of affect recognition and theory of mind,and with symptoms of psychopathology,as measured by a questionnaire of psychological functioning.We studied this association in a sample of 6-year-old children at high risk for neuropsychiatric disorders due to their history of pre-/perinatal complications (prematurity and neonatal hypoxicischemic encephalopathy [HIE]),and children without pre-/perinatal risk factors.The role of ANS abnormalities in the development of psychopathology and social skills is not easy to be tested:the origin of psychopathology is multifactorial and needs several years to become evident,years in which most variables may intervene.From a methodological point of view,furthermore,it is not possible to experimentally modify the variables considered.Therefore,the only ways to test the theories of the involvement of ANS in psychopathology is by performing retrospective studies,or,as us,by correlational/explorative investigations,which,however,do not allow us to infer a causal link between the variables.
We hypothesize that in children with a history of pre-/perinatal insults,social skills and HRV might highlight an interesting association.We excluded children who develop severe impairments,which may introduce biases in the interpretation of data.However,we think that children not developing severe disabilities are the most challenging group because the prognosis at birth is uncertain and subtle symptoms might be unrecognized.We chose to test the children at 6 years,an age that represents a phase of transition and challenge,requesting increased self-control and emotional regulation abilities.At this stage,cerebral complexity grows considerably,and increased environmental requests can make latent neurobiological vulnerability evident.
We considered the possibility that the selection of two peculiar populations could not allow generalization of results;therefore,we included a group of children without pre-/perinatal risk factors.We also measured cognitive,neuropsychological,and psychosocial functioning to control confounding variables.
Participants and Methods
Participants
In this cross-sectional observational study,children were sequentially recruited from January 2011 to June 2013 at the Children University Hospital of Padova according to the protocols of the Neonatal Brain Project,whose mission is a long-term follow-up (from birth up to school age) of infants admitted to the neonatal intensive care unit because of preterm birth (here,“premature”) or neonatal HIE (here,“HIE”).Membership was free and without compensation.Inclusion criteria for the recruitment of premature and HIE children are described in previous studies (Suppiej et al.,2017;Cainelli et al.,2018).Briefly,premature neonates were recruited when none of the following neurological risk factors were present:intrauterine growth restriction (defined as an estimated fetal weight below the 10thpercentile and umbilical artery pulsatility index greater than 2 standard deviations),craniofacial malformations,clinical evidence of neonatal encephalopathy,brain ultrasound evidence of intra-ventricular hemorrhage or periventricular cystic leukomalacia,occurrence of seizures,treatment with drugs (e.g.,sedatives) affecting the central nervous system.HIE neonates were recruited if they underwent therapeutic hypothermia,and inclusion criteria were:gestational age >36 weeks,any of the following:arterial umbilical cord or first blood gas analysis (within 1 postnatal hour) with pH <7.0,and base excess <12,or 10-minute Apgar score <5,or need for respiratory support at 10 minutes of life,moderate to severe encephalopathy within 6 hours of birth.
Children without pre-/perinatal risk factors (here,“healthy”)were recruited at birth from the hospital’s nursery and followed longitudinally by the same project.
For this study,we selected children of at least 6 years of age (range 6–9 years) with familial consent to participate in the study.Data were collected between 2017 and 2019 at the Children University Hospital of Padova.Exclusion criteria were the presence of major impairments(neurosensory impairments,cerebral palsy,and epilepsy);subsequent diagnosis of congenital malformations,inborn errors of metabolism,genetic syndromes or other medical comorbidities;intelligence quotient (IQ) <70;traumatic events or reported parental neglect;and invalidating parental pathologies that emerged during clinical follow-up.
Only data for children who underwent the complete assessment battery (HRV measurement,social skills,psychopathological questionnaire,neuropsychological,cognitive,and psychosocial evaluation) were analyzed for this study.
The study was carried out in accordance with The Code of Ethics of the World Medical Association (Declarationof Helsinki) for experiments involving humans.The ethics committee of our hospital approved the study (Comitato Etico per la Sperimentazione,Azienda Opedaliera di Padova,No.1693P).This study was reported according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement (Additional file 1).Parents provided written informed consent for their children to participate.The study flowchart Is shown inFigure 1.
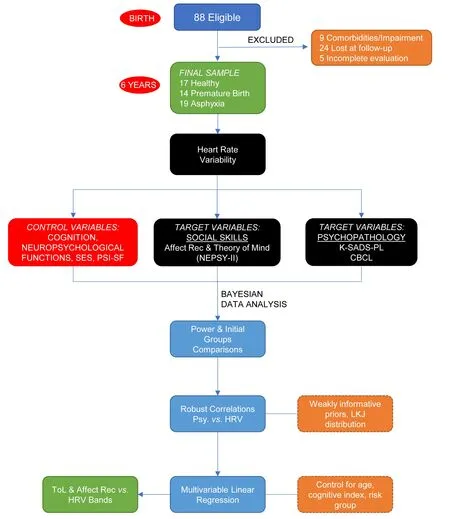
Figure 1|Study flowchart.
Procedure and assessment
A child psychologist and a child neurologist who were not aware of the medical status of the children assessed patients.Children came to our clinic twice,on successive days;several breaks were planned within each evaluation.Comfortable temperatures and a quiet environment were maintained throughout the assessments.
On the first day,children completed the cognitive assessment and neuropsychological tests.On the second day,as the child was more used to the setting,we first recorded ANS and then tested social skills and completed the remaining neuropsychological tests.All ANS recordings have been performed in the morning.
We also performed a psychological interview with children’s parents,who completed a questionnaire on their perceived level of stress from their parental roles and their child’s psychopathological profile.
HRV assessment
Data were recorded from photoplethysmography sensors using the PPG Stress Flow device software developed by BioTekna (Venice,Italy).HRV parameters were recorded for 5 minutes before the assessment when the child was still and at rest.Unfortunately,we had no control over the HRV detection algorithm since it was embedded in the measuring device.Nonetheless,the device is certified and based on published algorithms for detection and artifact detection,and it marks the measurements as unreliable even if few artifacts were detected.In this case,the analysis was repeated to obtain an artifact-free measurement.No individual was taken out of the analysis.If some problems occurred,we just re-performed the measurement.
The amplified signal was low-pass filtered (16 Hz) and digitized at 100 Hz.Collected data were exported for offline processing and analysis.These procedures were in line with the HRV analysis guidelines and focused on frequency domain analysis due to its better reliability on short recordings (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology,1996).For each segment,each arterial pressure wave was detected,and the so-called normal-to-normal (NN) intervals and the instantaneous heart rate were determined.Segments were analyzed as previously reported (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology,1996;Zong et al.,2003).Total spectral power (Tot Pow:0.0033–0.40 Hz),reflecting the global ANS activity,was recorded,as well as the three main spectral components distinguishable in the short term (5 minutes):the very low (VLF,0.003–0.04 Hz),intrinsically generated by the heart and modulated by the efferent sympathetic activity due to physical activity and stress responses,low (LF,0.04–0.15 Hz),reflecting a combination of sympathetic and parasympathetic nervous system activity,and high (HF,0.15–0.40 Hz),reflecting parasympathetic activity and corresponding to the heart rate variations related to the respiratory cycle,frequency bands.
Measurements of the VLF,LF,and HF power components were made in absolute values of power (ms2) and used as raw values or normalized to %HF.

Normalization minimizes the effect of changes in total power on the values of components (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology,1996).
Social skills tasks
For the evaluation of social skills,we used the Social Perception domain of the NEPSY-II (Korkman et al.,2007),which comprises two subtests measuring affect recognition and theory of mind.These tests are designed to measure several skills necessary for understanding others’ feelings,perceptions,and intentions.
The affect recognition subtest comprises four tasks,which assess the ability to recognize affect from photographs of children’s faces.Error scores are also provided for each of the emotions displayed in the subtest (Korkman et al.,2007).
The theory of mind subtest comprises two tasks (theory of mind A and theory of mind B),which assess the child’s ability to recognize facial affect,to understand how emotion relates to social context,and to recognize the appropriate affect given various social cues (Korkman et al.,2007).The tasks provide a Total score and two sub-scores (A and B).In task A,the child is read various scenarios or shown pictures and is then asked questions that require knowledge of another individual’s point of view to answer correctly.In task B,the child is shown a picture depicting a social context and asked to select a photograph from four options that depicts the appropriate affect of one of the people in the picture.
Psychopathological assessment
Each child’s psychopathological profile was explored by performing an in-depth and semi-structured psychological interview with the parents (the Kiddie Schedule of Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version [K-SADS-PL]) and by administering a questionnaire to the parents.The K-SADS-PL is a semistructured diagnostic interview designed to assess current and lifetime child psychiatric diagnoses,including diagnosisspecific ratings of impairment.It is appropriate for use in children and adolescents at 6–18 years of age (Kaufman et al.,1997).
Based on the presence (or absence) of a psychological disorder emerging from the psychological and structured interviews,we assigned a score of 0 (no disease) or 1 (presence of at least one clinically relevant psychological disorder).
The Child Behaviour Checklist (CBCL) is a multiaxial empirically-based set of measures that includes parent-,selfand teacher-report versions for assessing social competence and emotional/behavioral problems in children (Achenbach and Rescorla,2013).The parent-report version CBCL 6-18 comprises 118 items assessing the child’s emotional,behavioral,and social problems over the past six months.The items produce eight original empirically derived syndrome scales:Social Withdrawal,Somatic Complaints,Anxiety/Depression,Social Problems,Thought Problems,Attention Problems,Rule-Breaking Behaviour,and Aggressive Behaviour.It also produces two broadband scales:Externalizing Problems and Internalizing Problems.
Cognitive,neuropsychological,and psychosocial assessment
Given the importance of cognitive and psychosocial factors on the development of social abilities in children,we performed a comprehensive evaluation of these aspects,summarized in two indexes of risk (“Cognitive”and“Psychosocial”indexes).This methodology provides dichotomous values and is useful to quantify a wide range of abnormalities in a unitary measure.
The cognitive index was calculated from impairments of single functions.In essence,this was a binary classification:cognitive index=1 if a patient obtained an impaired score (<2 standard deviations) on at least two cognitive tasks or/and a borderline IQ (70 >IQ <85),and 0 otherwise.
We used the Wechsler Intelligence Scale for Children IV (WISCIV) (Wechsler,2003),standardized for the Italian population,to evaluate general cognitive performance.All results are expressed as age-standardized scores,with a population mean of 100 and a standard deviation of 15.
Neuropsychological domains were assessed as follows.For language,we used a naming test and a semantic verbal fluency test,which evaluate one’s ability to access the lexicon through a categorical cue (Bisiacchi et al.,2005).For attention,we used the visual and auditory attention tests of the NEPSYII (Korkman et al.,2007).For memory,we used the Corsi block-tapping test,which evaluates short-term verbal and visuospatial memory,and a word’s list and list recall,which evaluate learning and long-term verbal memory (Bisiacchi et al.,2005).To evaluate executive function,we used the Tower of London test,which evaluates planning and problem solving(Sannio Facello et al.,2006),the Coding test of the WISCIV (Wechsler,2003),and the Stroop Test,which evaluates inhibitory control (Marzocchi et al.,2010).Visuomotor functions were assessed using the visual-motor integration test (VMI;Beery and Beery,2004).
The Psychosocial Index was scored as 1 if at least two of the following events were reported in the in-depth anamnestic interview conducted with the parents:very low socioeconomic status (SES) as evaluated following the indications of Krieger et al.(1997),mild traumatic events (such as relocation,economic problems),conflictual relationship between parents,and/or a clinically relevant score on the Parent Stress Index-Short Form (PSI-SF).The PSI-SF (Abidin,2012) is a standardized tool that yields scores of parenting stress across four domains:parenting distress,difficult child,dysfunctional parent-child interaction,and total stress.
The Psychosocial Index was otherwise scored as 0.Severe events (parental death,neglect,invalidating pathologies,or substance abuse) were considered exclusion criteria (as described in Participant Section).
Statistical analysis
The statistical analysis was conducted and reported using the Statistical Analyses and Methods in the Published Literature(SAMPL) Guidelines for Biomedical Journals (Lang and Altman,2013).The full R code,models,raw data and all the results are available in a public repository (https://github.com/lucavd/HRV-and-social-skills).
Cognitive and neuropsychological results,and questionnaires
Scores for the social skills tasks and cognitive and neuropsychological instruments were age-corrected and converted into z-scores and scaled scores (neuropsychological tests),quotients (cognitive tests),or T scores (questionnaires),as appropriate,using published normative data.The z scores indicate the deviation from the mean population score,which is set to 0,standard deviation 1.A z score of–2 (or less) comprised 2.5% of the normal distribution and was considered to be significantly lower than average.Scaled scores indicate the deviation from the mean population score,which was set to 10,standard deviation 3.A scaled score of 4(or less) was considered to be significantly lower than average.The T scores indicate the deviation from the mean population score,which was set to 50,standard deviation 10.A T score of 70 (or more) indicates a clinical condition.
Results of the WISC-IV have been converted into standard scores having mean 100 and standard deviation 15.Impairment was defined as a standard score lying two standard deviations below the mean (<70).
Social tasks were also dichotomized:not impaired (for results>7 scaled scores),and impaired (for results <7 scaled scores,standard deviation <1).The Psychosocial Index was not included in the models because of the low incidence of scores of 1 (2/50 children).
Power analysis
The adequate sample size was determined based on group comparison,supposing a standardized difference of 0.5 in%HF for the impaired/not-impaired groups,corresponding to a medium effect size.We calculate the power of our analysis with a frequentist (classical) approach but in a Bayesian framework.We simulated 1000 distributions deriving from the comparison of a continuous variable (%HF) in impaired/notimpaired children.We then counted how many simulations did not contain zero in their 95%CI.Acceptable“score”was >80% of simulations with non-zero interval,corresponding to an 80%“power”,if calculated in a classical way.
We determined that a sample size of 50 children with a medium effect size (0.5) was sufficient to give a statistical power of 85%,comparing children with impaired/not-impaired social skills scores.To assess the degree of replicability of the results,we further extend the analysis to evaluate the power for decreasing effect sizes up to a minimum of 0.2,a small effect size (Quintana,2017),given the same sample size of 50 children.We found that a sample size of 50 children was not adequate to give a statistical power of at least 80% for effect sizes smaller than 0.5 (medium effect size).
Initial group comparisons of HRV bands,neuropsychological,and psychopathological results
Group comparison (similar to analysis of variance [ANOVA],in a classical framework) was conducted using a Bayesian linear regression model with Student’st-distribution to render it robust to outliers (Lange and Sinsheimer,1993).
Exploratory correlations
We evaluated simple,direct correlations between social skills tasks,cognitive,neuropsychological,psychosocial assessment with HRV bands (VLF,LF,HF,and %HF) and among each evaluated score.We performed the analysis in a Bayesian framework to avoid arbitrary multiple comparisons corrections and to minimize the false discovery rate by imposing weakly informative priors on the model’s parameters (Gelman et al.,2013).Specifically,we used Lewandowski-Kurowicka-Joe (LKJ) prior distribution (Lewandowski et al.,2009) on the correlation’s parameters with the concentration parameter equal to 4.Such a prior distribution,highly concentrated around zero,minimizes the risk of observing non-zero correlations that may arise only by random chance,as often occurs with small sample sizes like the one in this study.
Multivariable linear regression
We used Bayesian robust multivariable regression to assess the ability of HRV bands to predict affect recognition and theory of mind total scores controlling for age,cognitive index,and risk group (premature,HIE,and healthy children).To implement a model robust to unusual and influential cases,we used a Student’st-distribution with a gamma prior distribution (k=4,Ɵ=1) on the degrees of freedom parameter.This prior gives a higher probability of degrees of freedom values between 2 and 5,which corresponds to a Student’s t-distribution with heavier tails than a normal distribution,thus more robust to outliers.
Comparison of impaired/not-impaired children
For consistent analysis,we performed group comparison between impaired/not-impaired patients (similar to the classical“t-test”) in a Bayesian framework using a robust linear model with Student’st-distribution and flat priors.Bayesian estimation for the two groups comprises distributions of credible intervals (CI) for the effect size,group means and their difference,standard deviations and their difference,and the normality of the data (Kruschke,2013).
For all models above,results whose CIs do not contain zero,i.e.,the value of no correlation,were identified as“significant.”Sampling from the posterior distribution of the model’s parameters was carried out using the Hamiltonian Monte Carlo (HMC) algorithm with Stan software for Bayesian inference (Carpenter et al.,2017).The algorithm was run with 4 chains and 2000 iterations,of which 500 were discarded as a warm-up.The convergence of the algorithm was assessed using trace plots and an improved version of the R-hat parameter (Gelman et al.,2013).
We implemented all statistical analyses in R software for statistical computing (version 3.6.3).The {brms} package was used to fit the models (version 2.12.0;Bürkner,2020).
Results
Descriptive results
At the time of the study,88 children were eligible by age(almost 6 years old;19 healthy,29 premature,40 HIE),though 9/88 were excluded because of major impairments or comorbidities (2 premature,7 HIE) and 24/88 were lost at follow-up or declined to participate (2 controls,11 premature,11 HIE);finally,5/55 did not complete the evaluations (2 premature,3 HIE).The final sample population consisted of 50 patients,aged 7.4 ± 1.4 months,31 (62%) males,4 (8%) born in Italy from a foreign family (3 Slavic,1 North African),and fluently speaking the Italian language.Seventeen were healthy(34%),14 premature (28%),and 19 HIE (38%) children.
Social task results
Considering individual impairments in social abilities tasks,affect recognition indicated impairment in 8 children (16%)and was borderline in 10 (20%);theory of mind total score indicated impairment in 4 children (8%) and was borderline in 7 (14%);theory of mind A indicated impairment in 2 children (4%) and was borderline in 8 (16%);theory of mind B indicated impairment in 4 children (8%) and was borderline in 6 (12%).Details on results in the different groups are shown inTable 1.
Psychopathology results
Globally,the administration of the semi-structured diagnostic interview K-SADS-PL,evaluating current and lifetime child psychiatric diagnoses,and including diagnosis-specific ratings of impairment,revealed that children met the criteria for six disorders (attention deficit hyperactivity disorder,separation anxiety,generalized anxiety,specific phobias,depressive mood,and encopresis).Details on results in the different groups are shown inTable 1.

Table 1|Number and percentage of impaired and borderline scores for social skills tasks,and children with clinically relevant scores at the psychopathological/behavioral questionnaire,diagnoses at the structured interview,and alteration in the cognitive and psychosocial risk indexes
From the administration of the parent-report CBCL 6-18,none of the children in the healthy group exhibit high scores in the internalizing and externalizing scores.However,one child had high scores for anxiety/depression and thought domains,and another for attention and social problems and thought problems.Among the premature children,one exhibited high scores in the internalizing and total scores,with particularly high scores in the withdrawal,anxiety/depression,and somatic complaints domains.Three children reported high scores in anxiety/depression and somatic complaints domains.Among HIE children,one exhibited high scores in the internalizing,externalizing,and total scores,with high scores in all domains except withdrawal and somatic complaints,and one other exhibited attention and thought problems.Two had somatic complaints,one attention problems,and one exhibited withdrawal.Further details are provided inTable 1.
Social tasks and psychopathology correlations
We found an association between affect recognition and the presence of psychopathology:children with better performance in this task had a lower incidence of psychological disease (correlation coefficient–0.28,95%CI:–0.51 to–0.01).Furthermore,better performance on theory of mind tasks was associated with lower scores on the withdrawal subscale of the CBCL 6-18 questionnaire(correlation coefficient–0.30,95% CI:–0.53 to–0.01).
Cognitive,neuropsychological,and psychosocial results
The cognitive index was positively assigned to eight children(16%).Only two children (4%) had a non-zero psychosocial risk index.Details are shown inTable 1.
The mean cognitive and neuropsychological scores of all explored domains were within the average of normality for the tests.Mean scores did not differ significantly between groups,except for IQ and memory (word list) scores,which were significantly lower in premature than healthy children.Mean scores obtained from the cognitive and neuropsychological examination are shown inAdditional Table 1.
HRV results
The mean absolute and relative power results obtained from HRV components did not differ between groups (healthy,premature,and HIE children).Details are shown inAdditional Table 2.
Correlations
We first conducted simple correlations between social skills tasks,cognitive,neuropsychological,psychosocial assessment,and HRV bands (Table 2).
Social task scores were significantly and directly correlated with HF and %HF.No other significant correlations were found.Interestingly,for the psychopathological questionnaire,a significant correlation was observed with the VLF HRV band(for somatic complaints) but not with HF or %HF (Table 2).
Comparisons of impaired/not-impaired children
We then dichotomized social skills tasks scores (>7 or ≤ 7) in order to assess HRV components’ values in impaired children(i.e.,those with a pathologic score).All HRV components were reduced in children with impairment of both social abilities tasks scores,but the only %HF was able to significantly distinguish impaired children,and only in the affect recognition task (correlation coefficient–0.69,95% CI:–1.26 to–0.13;Figure 2andAdditional Table 3).
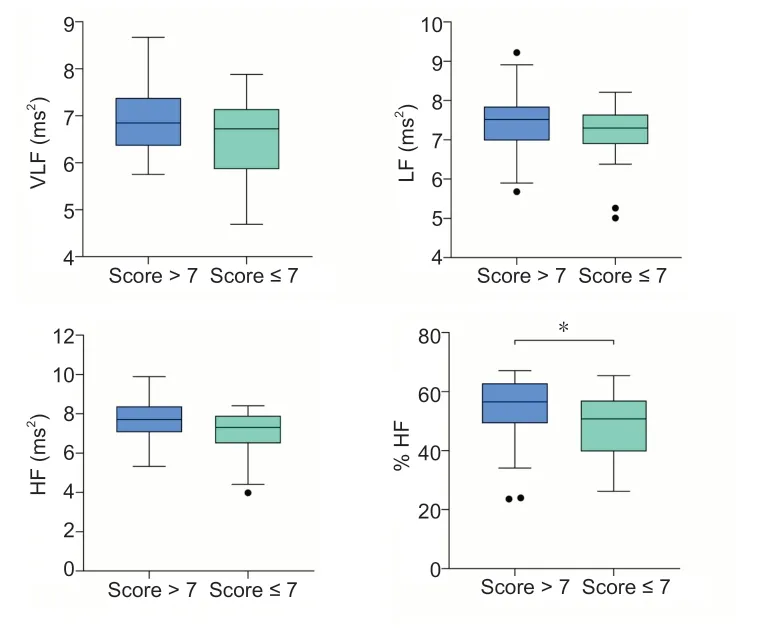
Figure 2|HRV bands comparison between children with impaired (≤7 scaled scores) and not impaired (>7 scaled scores) scores in affect recognition with a Bayesian linear model (i.e.what in a frequentist approach would have been a t-test).
Multivariable regressions of social tasks scores
We conducted a multivariable linear regression analysis to assess single HRV bands’ correlation with social skills scores,adjusting for potential confounders.The following predictors were considered in the models in addition to HF:cognitive index,age at assessment,and risk group (Table 3).
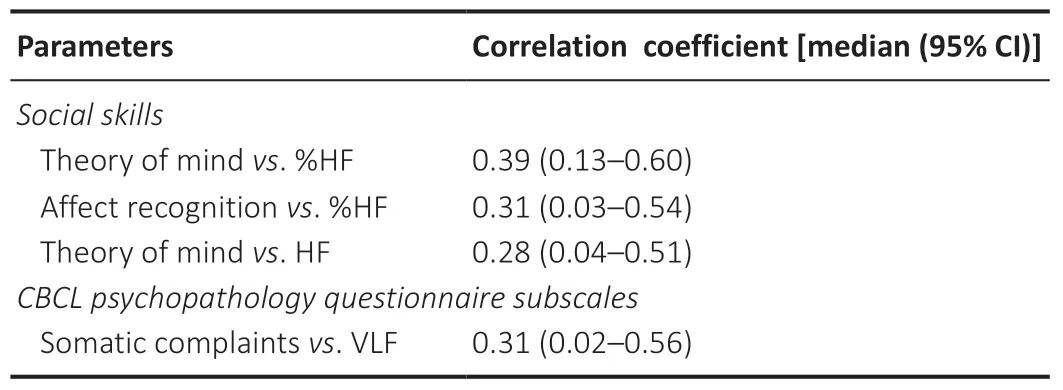
Table 2|Non-zero correlations of social skills (ordered by strength of the correlation coefficient)
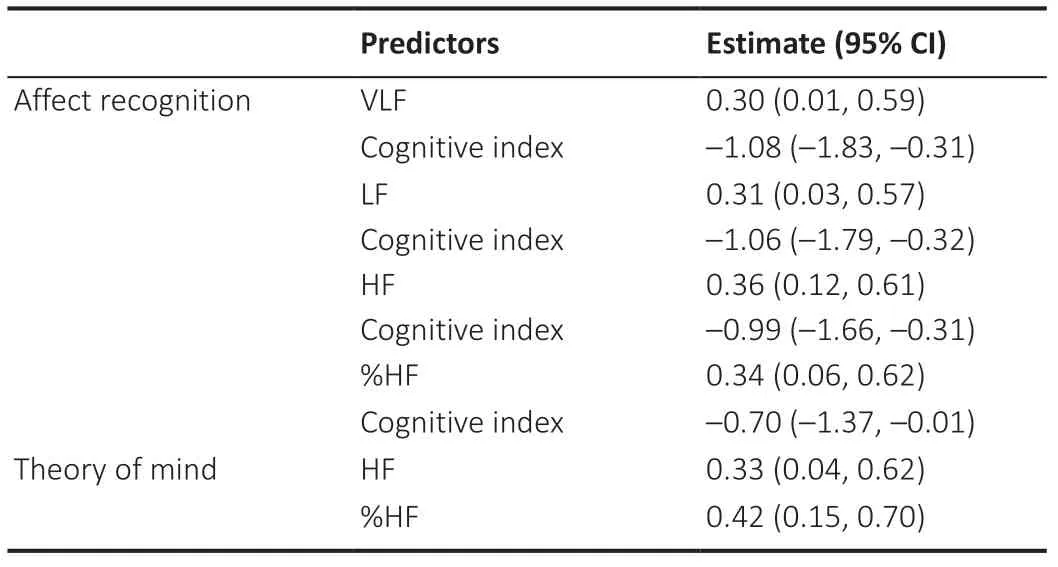
Table 3|Significant predictors of social skills tasks identified with multivariable regressions
In fact,when the other variables were kept constant,all four HRV components were significant predictors of affect recognition scores,with HF the most consistently predicted band.Theory of mind scores were significantly predicted only by HF and %HF.Affect recognition scores were also significantly associated with cognitive index,while the theory of mind scores were not.
Discussion
We investigated the association between HRV parameters,as a proxy of ANS status,and social functioning,as measured by standardized tasks and a psychopathological evaluation.We chose three groups:two groups of children at high risk to develop neuropsychiatric disorders due to their history of pre-/perinatal insults (premature birth and neonatal HIE) who showed low cognitive vulnerability and no major impairments(cognitive disability,cerebral palsy,neurosensorial deficits),and a sample of children without pre-/perinatal risk factors.
As expected,deficits in social skills are mainly represented in children with a history of pre-/perinatal insults.Given the relatively high percentage of children with impaired scores for social tasks,we tested the clinical significance of our results by comparing HRV components between children with scores indicating impairment/not impairment.The metric of %HF was the only able to significantly distinguish impaired children in the affect recognition task,even though all HRV components were reduced in the impaired children group.
Furthermore,we found that specific HRV parameters were associated with both social skills tasks,affect recognition,and theory of mind:stronger abilities were associated with higher HF.Multiple regression analyses confirmed the HF component was the best parameter to predict social skills after controlling for other cognitive and psychosocial risk factors,regardless of the neurodevelopmental risk group.By contrast,the other HRV parameters weren’t associated with the social tasks.
Our results are in line with previous research showing associations between higher power for the HF component and better performance of prefrontal functions (Thayer et al.,2009;Stenfors et al.,2016).The prefrontal cortices are part of a complex interplay comprising the limbic system (thalamus,fornix,olfactory cortex,hippocampus,hypothalamus,and cingulate gyrus),central ANS (brainstem),and other highorder cerebral areas and white matter tracts,which determine the underlying substrate of social behavior.As in our work,most previous empirical research found associations between cognitive tasks and HF,and not other HRV components,in line with the hypothesis based on Porges and Thayer theories on the role of the vagal nerve in the prefrontal functions,but also with knowledge about the generators of the different measurements (Shaffer et al.,2017).
Although social competence is an ambiguous concept,social behavior is based on a constellation of cognitive,behavioral,and emotional factors.We choose to investigate two central skills of social competence:theory of mind and affect recognition.Theory of mind can be considered the cognitive dimension of social skills.It develops early in childhood,emerging from the capacity for symbolic play through the understanding of others’ points of view to an eventual understanding of other people’s mental states (Szumski et al.,2019).Affect recognition is the ability to infer emotional states from the faces of others.The face is an essential source of information in social interaction;thus,the ability to appropriately read and respond to the facial expression of others is essential for successful participation in everyday social life (Morris et al.,2020).
Abnormal responses in the theory of mind and affect recognition are implicated in several neuropsychiatric disturbances,ranging from autism spectrum disorder to schizophrenia (Szumski et al.,2019).In fact,our cohort of children exhibits a high percentage of psychological and behavioral problems,particularly internalizing disturbances,such as anxiety and somatic complaints,and attention deficit hyperactivity disorder.As expected,these disorders are associated with performance in social skills tasks (with lower performances found in children with psychopathology).
Interestingly,we also found an association with HRV:children with higher levels of VLF activity exhibited higher scores on subscales of somatic complaints.Epidemiologic studies have shown an increase in the prevalence of somatic complaints (up to 5–30% of children at 8–16 years of age) (Gini et al.,2009).It has been suggested that a limited ability to identify and express emotions is the main characteristic of individuals with somatic complaints (van der Veek et al.,2012),determining the use of maladaptive coping strategies and somatization.Interestingly,stress situations may modulate the VLF component of HRV (Shaffer and Ginsberg,2017).High levels of VLF may reflect an imbalance between parasympathetic and sympathetic activity,with a consequent reduction of inhibition on VLF,predisposing to stress vulnerability.A vulnerability to further stressful life events in the child’s daily life may,in turn,trigger incongruous bodily responses within the broad spectrum of somatic symptoms (Rees,2014).Moreover,the different levels of social behavior evaluated in this study were associated with different components of HRV:HRV is a mixed measure,and its components likely reflect different aspects of the complex mechanisms underlying social behavior.Probably this is also the reason because we did not find associations with HRV components,and especially HF,and between HRV measures and other psychological domains.However,this also points to our yet immature understanding of HRV and its contribution to cognition/psychology.
Social behavior crucially influences psychopathology.Emotional competencies and social cognition are essential functions for mental health,and they are the core feature of several neuropsychiatric disorders.Social skills deficits have been related to many disorders,including depression,anxiety,autism,and attention deficit hyperactivity disorder (Gazelle et al.,2005;Deschamps et al.,2015).Such deficits can be studied early in childhood,long before neuropsychiatric diseases are fully established.Therefore,social skills are a good candidate to study the origin and development of psychopathology.In essence,they allow the operationalization of a common dysfunctional mechanism,which may subsequently allow consolidation of the broad range of symptoms of different disorders.
In our study,findings on the association between HRV and social skills held irrespective of group,suggesting an ANS contribution to conditions of both typical and atypical development.From another point of view,HRV shows cross-disease sensitivity,despite the different causal factors implicated in the onset of social difficulties.We are tempted to hypothesize that the ability of HRV parameters to discriminate children with poor social abilities may be the consequence of an alteration in the developmental trajectory of ANS.
ANS is thought to be programmed in utero and the early postnatal months to prepare children for their environment(Shonkoff et al.,2012).Early in brain development,limbic structures develop multiple interconnections,including those to the ANS brainstem centers.At birth,the system lacks specificity:so,circuitry with evolutionary roles of ensuring efficient responses to“predators”might be influenced by antenatal stress or unpredictable pain and hyper-stimulation under neonatal intensive care.The consequence may be ANS dysregulation,transforming adaptive responses into inflexible and counterproductive behaviors.Function adapted to“emergency”conditions will be unhelpful if it becomes fixed (Rees,2014).The functional connections established during pregnancy and the first months of postnatal life are modulated throughout life by several other environmental factors,particularly in the early years (Faa et al.,2016).The few available data suggest that premature birth and neonatal HIE may predispose children to neonatal ANS abnormalities(De Rogalski Landrot et al.,2007).Furthermore,followup studies in former preterm and HIE children showed that these abnormalities may persist in the long term (De Rogalski Landrot et al.,2007;Suppiej et al.,2020).Because ANS has widespread effects in multiple systems,its clinical manifestations can vary widely,explaining the high interindividual variability (Ming et al.,2011).
Unlikely,historically,studies interested in high-order human functions paid scarce attention to“other”systems,such as white matter,subcortical grey assemblies,and autonomic nervous system.Pathophysiological mechanisms underlying contribution to abnormal cognition and psychopathology are only partially understood,but probably most of them involve oligodendrocytes and myelin formation.Glial cells and myelinated axons determine the speed and coordination of action potential propagation along with neuronal fibers and among neurons (Salami et al.,2003).However,the direct link between altered neurobiological patterns and the functional counterpart is still missing.
We hypothesize that the large variability in the neurodevelopment abilities of our children might better be explained by abnormal ANS functioning and altered ANS-CNS integration than by any specific pre-/perinatal pathological condition.Therefore,it would be important to move beyond the isolated system and start to evaluate the efficacy of possible neuroprotective and rehabilitative interventions(Cainelli et al.,2020).A similar shift in perspective might be a crucial perspective in understanding factors that drive traininginduced changes (Caeyenberghs et al.,2016).The ability to improve the underlying circuitries reveals the considerable potential of behavioural assistance and rehabilitation programs,providing possible remediation for children at risk for neurodevelopmental impairments.
Strengths and Limitations
The results of our study should be interpreted considering several strengths and limitations.Our principal aim was to investigate an association between social skills measures and HRV.We chose to test children with a history of pre-/perinatal insults,given their high vulnerability to neurodevelopmental sequelae,even in the absence of overt brain damage.To avoid specific biases due to the samples selected,we also included a group of low-risk,apparently healthy children.Our study is prospective and longitudinal:our participants were enrolled sequentially and followed rigorously from birth until school age.
For the same reason,we choose a correlational analysis weighted for groups and not a comparative analysis between groups to be the core of our analysis.Our sample size was adequate,as showed by the power analysis.A strength of our study is that we have evaluated the association while adjusting for potential confounding predictors.Given the complexity and the numerous factors involved in the development of the personality,we tried to include several variables that encompassed environmental and parental factors.
We performed the statistical analysis in a Bayesian framework to address issues that might have arisen with frequentist analysis given the small sample size and multiple outcomes settings of our study (McNeish,2016).Indeed,the use of weakly informative priors decreases the likelihood of observing significant differences by chance alone,as would have occurred with classical frequentist methods (Gelman et al.,2017).
A limitation of our study is that the short HRV recordings suggest caution in the interpretation of the HRV VLF component.Furthermore,HRV components are strictly interconnected,and the interpretation of HRV parameters requires an overall evaluation of the components in a broader framework,as occurs in the clinical setting.Considering these cautions,we aimed to identify the association between HRV and social measures to investigate the involvement of the ANS in social development,without a specific focus on the components,which would require more controlled conditions.A strong limitation of our study is the small sample size.We implemented conservative and robust analytical methods,but the generalization of our results could be difficult in the absence of wider studies.To address this point,we evaluated the power of the study for lower effect sizes and we found that the sample size of our study might not be adequate to reach a power of at least 80% for effect sizes lower than 0.5(medium effect size).Future research would also benefit from the use of other ANS measures,such as skin conductance and respiratory sinus arrhythmia,which could sustain HRV findings and provide additional information about sympathetic and parasympathetic involvement.
Finally,even if our group of children has been followed longitudinally from birth to the age of the evaluations,both the HRV recordings and the social skills have been performed at the same age,in a cross-sectional way.Such a design,together with the observational nature of the study,does not allow to exclude the possibility that the two variables are associated because both are caused by a“third variable.”Additional information would have been useful if we could have made repeated HRV recordings from birth until followup.In any case,the hypotheses remain a complex topic to investigate given the limited possibilities to manipulate and intervene on the variables of interest.
Conclusion
We reported a possible association between HRV activity and social skills in children,irrespective of their pre-/perinatal risk factors.We have hypothesized that the ANS might provide the substrate for psychological vulnerability,both under typical and atypical developmental conditions.Injuries in the developing brain have no easy management nor magic bullet for an assured cure.In this scenario,it would be worthwhile to obtain a deeper understanding of the predictive potential of HRV assessment,also given their cost-effective and easy to use nature,which makes it usable even in low-income countries.The same flexibility that renders ANS difficult to study also offers a great possibility to intervene on it,as the promising results of lifestyle and diet programs on ANS function have been shown (Reginato et al.,2020).The prolonged critical period for ANS development increases its vulnerability;fortunately,this feature also extends the window during which developmental plasticity may be exploited to promote normal ANS development even after initial pre-/perinatal distress(Mulkey and du Plessis,2019).
Author contributions:Substantial contribution to conception and design;substantial contribution to the acquisition and analysis of data;drafting:EC.Substantial contribution to the acquisition and analysis of data;critically revising the manuscript:LV.Substantial contribution to the analysis of data;critically revising the manuscript:DBottigliengo.Substantial contribution to conception and design;substantial contribution to the interpretation of data‚critically revising the manuscript:DBoschiero.Substantial contribution to conception and design;critically revising the manuscript:AS.All authors approved the final version of the manuscript.
Conflicts of interest:Dario Boschiero is the scientific director of BIOTEKNA Biomedical Technologies.All the other authors declare no conflict of interests.
Financial support:None.
Institutional review board statement:The study was approved by the Ethics Committee of the University Hospital of Padova (approval No.1693P).
Declaration of patient consent:The authors certify that they have obtained all appropriate patient consent forms.In the forms the patients have given their consent for their children’s images and other clinical information to be reported in the journal.The patients understand that their children’s names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement:This study followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
Biostatistics statement:The statistical methods of this study were implemented and reviewed by two biostatistician (DBottigliengo and LV)‚Unit of Biostatistics‚Epidemiology and Public Health‚Department of Cardiac‚Thoracic‚Vascular Sciences‚and Public Health‚University of Padova‚Padova‚Italy.
Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement:Anonimyzed full raw data‚code‚and raw results are immediately‚indefinitely‚and freely available with MIT license at this public repository https://github.com/lucavd/HRV-and-social-skills.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access journal‚and articlesare distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License‚which allows others to remix‚tweak‚and build upon the work non-commercially‚as long as appropriate credit is given and the new creations are licensed under the identical terms.
Additional files:
Additional file 1:STROBE checklist.
Additional Table 1:Mean and standard deviation of cognitive and neuropsychological scores in the three groups.
Additional Table 2:Absolute and relative power of the HRV bands in the three groups.
Additional Table 3:HRV bands measures in impaired/not-impaired children for social skills.
- 中国神经再生研究(英文版)的其它文章
- Towards a comprehensive understanding of p75 neurotrophin receptor functions and interactions in the brain
- Microglia regulation of synaptic plasticity and learning and memory
- Stroke recovery enhancing therapies:lessons from recent clinical trials
- Functional and immunological peculiarities of peripheral nerve allografts
- MicroRNA expression in animal models of amyotrophic lateral sclerosis and potential therapeutic approaches
- Significance of mitochondrial activity in neurogenesis and neurodegenerative diseases