
Quantitative alpha-defensin testing: ls synovial fluid dilution important?
2022-08-19 08:15RodrigoCalilTelesAbdoRiccardoGomesGobbiChilanBouGhossonLeiteSandraGofinetPasotoElainePiresLeonAnaLuciaLeiMunhozLimaEloisaBonfaJosRicardocoraMarcoKawamuraDemange
World Journal of Orthopedics 2022年8期
lNTRODUCTlON
Periprosthetic joint infection (PJI) is an increasingly common and devastating complication that can lead to significant morbidity and mortality[1,2]. Since neither clinical examination nor laboratory tests are always trustworthy, the diagnosis of PJI remains a challenge[3]. Indeed, there is no gold-standard method for its diagnosis[4]. Therefore, several groups around the world have attempted to refine the diagnostic criteria of PJI[2,5,6]. The criteria score proposed (and later updated) by the Musculoskeletal Infection Society (MSIS) is the one most used by orthopedic surgeons[2].
Regarding the different strategies to improve the diagnosis of PJI, the use of biomarkers has been extensively studied in recent years[1,7,8]. Alpha-defensin has gained attention as one of the most reliable markers[9,10]. Defensins are antimicrobial peptides that act as part of the host's innate immune response against pathogen invasion and are produced in increased numbers during septic inflammation[11,12]. Thus, synovial-fluid alpha-defensin has shown excellent results in diagnosing PJI[13,14]. Two different modalities are available to measure synovial alpha-defensin: The qualitative alpha-defensin lateral flow test and the quantitative enzyme-linked immunosorbent assay (ELISA)[15]. Particularly, the ELISA method has presented the best results, so it was included as a criterion in the new International Consensus on Orthopedic Infections 2018 consensus[6].
As soon as they were cooked the old dame39 took a pair of scales and a morsel40 of bread from the cupboard, and was just about to divide it when Prince Vivien, who really could wait no longer, seized the whole piece and ate it up, saying in his turn, Patience
Despite the importance and the many studies about alpha-defensin in synovial fluid[15,16], there is a lack of detailed information regarding the ELISA technique[13]. In fact, some crucial information about the reproducibility of the test and the standardization of specific cutoff values are unclear. Dilution of the synovial fluid sample is necessary for the test, but the ideal ratios are not known.
the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), No. 2017/25540-9.
Therefore, this study aimed to evaluate the potential influence of dilution on the quantitative alphadefensin ELISA test for the diagnosis of PJI in the synovial fluid of patients undergoing total knee arthroplasty (TKA). We hypothesized that changes in the dilution of the joint fluid would influence the test performance for the diagnosis of PJI.
MATERlALS AND METHODS
The study was approved by the local ethics committee (No. 71039317.3.0000.0068). All the included patients signed the consent form.
Another interesting consideration relates to the prozone phenomenon. The prozone phenomenon, also known as the hook effect, is a false-negative response that occurs in immunological tests as a consequence of an excess of either antigen or antibody[20]. In an alpha-defensin test, if the amount of antigen (alpha-defensin) is greater than the amount of antibody, the secondary antibody (peroxidase) will not bind properly, and the test will present a false result. This could be the reason for some false-negative values during the alpha-defensin assay. In this study, we did not directly assess the influence of dilution on the prozone phenomenon, but since lower dilutions are more likely to exhibit the prozone effect, the latest dilutions may be helpful to overcome this phenomenon[21], potentially allowing a more precise differentiation between TKA infection and asepsis.
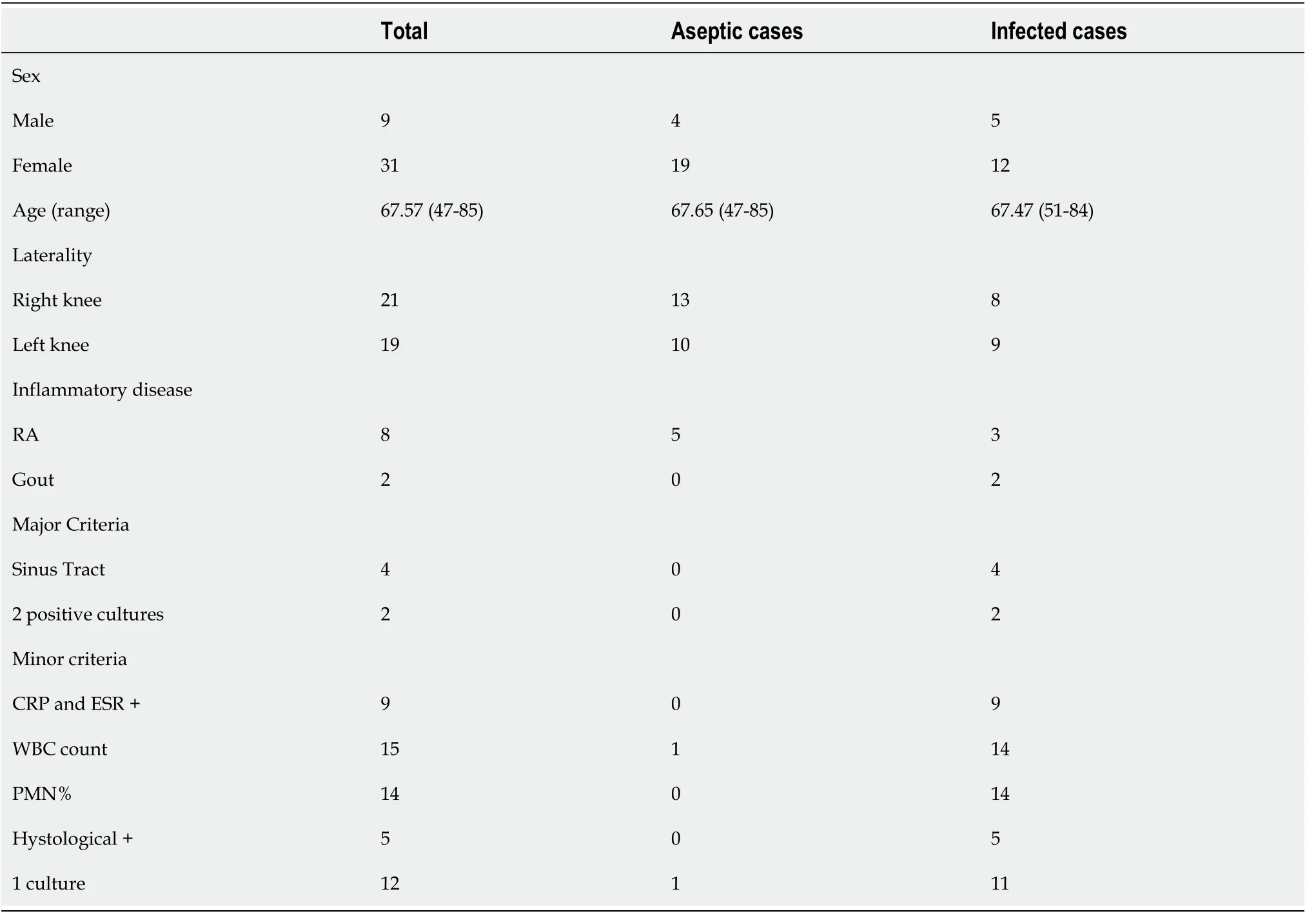
Between January 2017 and December 2018, this study enrolled patients with primary TKA and any suspicious signs or symptoms of chronic infection, as follows: more than three months of persistent knee pain, effusion or local heat, presence of a draining sinus, early failure of the prosthesis (less than 5 years), fever and malaise. Patients who had used antibiotic therapy for at least four weeks before the evaluation or had an insufficient volume of synovial fluid during knee aspiration were excluded. Fortyfive patients were assessed for recruitment. Of these, five did not have enough synovial fluid and were excluded from the study. The other 40 patients were included. They were divided into two groups: infected and noninfected (aseptic painful). Seventeen (42.5%) patients were considered to have infection, and 23 (57.5%) patients were classified as having aseptic painful TKA. Positive infection was confirmed if the MSIS criteria for PJI were fulfilled[17], as follows: presence of a draining sinus communicating with the joint or at least two positive cultures of the same microorganism, or if three out of the following five criteria were present: elevated serum C-reactive protein and erythrocyte sedimentation rate, elevated synovial white blood cell count, elevated percentage of synovial polymorphonuclear leukocytes (PMNs), positive histological analysis of periprosthetic tissue and a single positive culture of synovial fluid or periprosthetic tissue. For chronic PJI, synovial cell count and differential cutoff values were 3.000 cells/μL, 80% PMN.
Never had Sir Red been so eaten up with envy as he was now, and he racked his brain day and night to find something quite impossible to demand from the brothers
We next evaluated all of the remaining samples using these dilution ratios. The results of the alphadefensin tests including all patients are displayed in Table 3 and Figure 2. At a dilution of 1:1000, statistical analysis indicated a sensitivity of 88.2% (95%CI, 66%-98%), a specificity of 95.7% (95%CI, 79%-99%), a positive predictive value of 93.8% (95%CI, 72%-99%) and a negative predictive value of 91.7% (95%CI, 74%-99%). In this situation, one false positive and two false negatives were found.
Determination of synovial alpha-defensin concentrations
Statistical analysis was performed using GraphPad Prism version 8 (GraphPad Software, La Jolla, CA). The results of the alpha-defensin synovial fluid are expressed as mean and range. Differences between the two groups were compared using the Mann-Whitney test. To assess the performance of the test using 1:1000 and 1:5000 dilutions, the sensitivity, specificity, positive predictive value and negative predictive value were evaluated through the Wilson-Brown method. The 95% confidence interval (95%CI) was also calculated.< 0.05 was considered to be statistically significant.
Initially, ten out of 40 cases were selected to define which dilutions would provide the best performance. After detecting which dilutions performed better, we expanded the analysis to all other cases. All samples were tested with the selected dilution ratio, following the same procedures as described above except for the serial dilution.
Statistical analysis
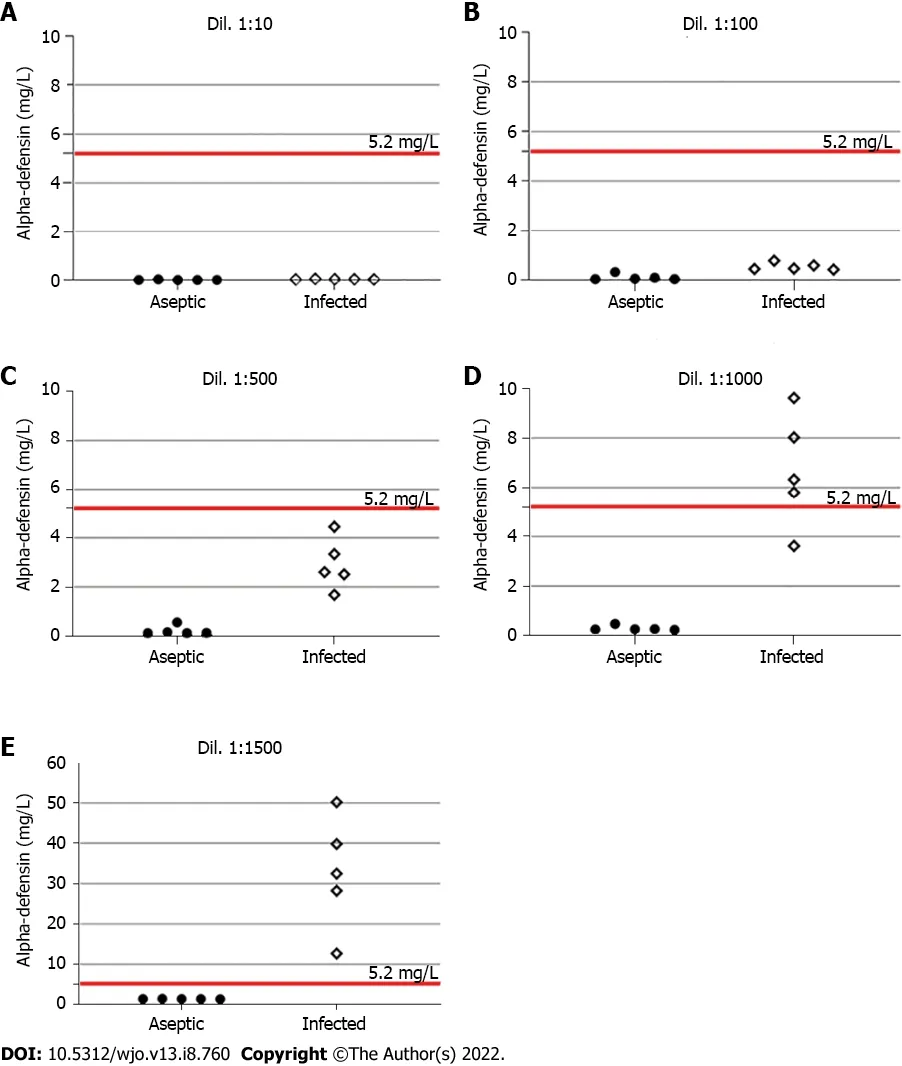
Reagents from the commercially available ELISA test kit (Hycult Biotech, Uden, The Netherlands) were used according to the manufacturer’s instructions. However, as anticipated, there was no manufacturer recommendation for synovial fluid dilution. In this study, ten samples (five from each group) were randomly selected and diluted in the buffer included in the kit at 1:10, 1:100, 1:500, 1:1000 and 1:5000. All dilutions were tested in duplicate. The reactions were read at 450 nanometers in an ELISA SpectraMax 190 reader (Molecular Devices, San Jose, United States) in accordance with the package insert instructions. The results of spectrophotometry were obtained in optical density (OD) units. The OD values were plotted on the vertical axis, and the corresponding concentrations were plotted on the horizontal axis (logarithmic scale). The concentration was multiplied by the dilution factor to obtain the actual alpha-defensin value in mg/L. A cutoff value of 5.2 mg/L was used since the same value was used as the cutoff in previous studies[13,18].
RESULTS
Table 1 shows the demographic and laboratory results of the included patients. Regarding the initial assessment, five samples from each group were tested using different dilutions. In the infected group, a gradual increase in synovial fluid dilution resulted in an equivalent elevation of alpha-defensin levels. The same response was not observed in the aseptic group (Figure 1). In addition, the best diagnostic performance of the test was obtained at 1:1000 and 1:5000 dilutions. Table 2 summarizes these findings.

Synovial fluid was collected from each patient. Using a sterile technique, the lateral suprapatellar approach was performed, and a 20-mL syringe with a 21-gauge needle was used to aspirate the joint fluid. A minimum of 0.5 mL was aspirated and stored in a tube with ethylenediaminetetraacetic acid (EDTA). The tubes were transported to the laboratory within one hour after aspiration at room temperature. Previous studies have estimated the stability of alpha-defensin levels in synovial fluid for a minimum of 48 h at room temperature[13]. The fluid was centrifuged for ten minutes at 2000 rpm according to our laboratory standardization, and the supernatant was frozen at -80°C until use[13].

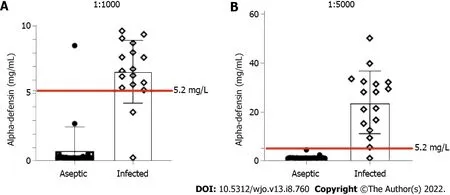
At the 1:5000 dilution, a sensitivity of 94.1% (95%CI, 73%-99%), a specificity of 100% (95%CI, 86%-100%), a positive predictive value of 100% (95%CI, 81%-100%) and a negative predictive value of 95.8% (95%CI, 80%-99%) were observed. Only one false-negative result was identified within the infected group. This misdiagnosed case presented with a draining sinus and had positive intraoperative cultures.
DlSCUSSlON
To the best of our knowledge, there is a lack of studies detailing and testing the influence of different dilutions on the synovial fluid alpha-defensin ELISA test for the diagnosis of TKA infection. The novel results of this laboratory study support our hypothesis that the right synovial fluid dilution is crucial for a high diagnostic accuracy of the alpha-defensin ELISA test. Here, we found positive results using dilutions of 1:1000 and 1:5000, the best results occurring with a 1:5000 dilution ratio.
As mentioned above, in one of the first studies of synovial fluid alpha-defensin, a cutoff value of 5.2 mg/L of alpha-defensin was defined as the threshold for the diagnosis of PJI[19]. However, the dilutions applied to obtain this cutoff value were not described, making it hard to replicate the methods, even using the same alpha-defensin ELISA kit. In our study, using a 5.2 mg/L cutoff, the most effective dilution to distinguish between infection and noninfection was 1:5000. Using this dilution ratio, only one false-negative result was found. Similar to other patients[10,13], this patient presented with a drainage sinus, though our patient had positive intraoperative cultures, which was not seen in that other series. We also showed that although a dilution of 1:1000 had satisfactory results for detecting infected cases, it had lower sensitivity and specificity.
Judge of her astonishment35 when she saw that he was holding in his hand a portrait of herself! In vain did she puzzle over the apparent contradictoriness36 of his behaviour
Some limitations of our study must be considered. The small sample size may underpower the study. However, the consistent findings with different dilutions and the excellent results using a 1:5000 dilution reduced the need to increase the sample size. In addition, despite the exciting progressive improvement in the test performance with serial dilutions, we did not demonstrate the actual reason why it occurs. Further studies are necessary to answer this question. Even so, we describe in detail the analysis of synovial fluid alpha-defensin by ELISA, including the best dilutions for the most accurate diagnosis of knee PJI. Moreover, the information provided herein may ensure the reproducibility of the test across the laboratories, with more precise data.
CONCLUSlON
All study participants, or their legal guardian, provided written consent prior to study enrollment.
Strangers who had heard of the marvels2 which the king had collected, and made long journeys to see them, were, however, surprised to find the most splendid stall of all occupied by a donkey,1 with particularly large and drooping3 ears. It was a very fine donkey; but still, as far as they could tell, nothing so very remarkable4 as to account for the care with which it was lodged5; and they went away wondering, for they could not know that every night, when it was asleep, bushels of gold pieces tumbled out of its ears,2 which were picked up each morning by the attendants.
ARTlCLE HlGHLlGHTS
Research background
Periprosthetic joint infection (PJI) is a serious complication post-surgery that is associated with substantial morbidity and financial burden to the healthcare system. The alpha-defensin quantitative enzyme-linked immunosorbent assay (ELISA) is one of the most useful methods to investigate PJI.
Research motivation
Although the alpha-defensin ELISA is currently the most reliable test to diagnose PJI, there is a lack of detailed information regarding its proper laboratory technique, including the best sample dilution.
Research objectives
This study aimed to assess the influence of dilution in the synovial fluid during ELISA for the diagnosis of knee PJI and determine which dilution presents a better performance.
Research methods
In this prospective study, 40 cases of total knee arthroplasty were evaluated: 17 classified as PJI and 23 classified as aseptic knees. Initially, 5 synovial fluid samples from each group were assessed by ELISA using different dilution ratios (1:10, 1:100, 1:500, 1:1000 and 1:5000). The dilutions had better performance were used to compare the results of all samples.
Research results
For infected cases, a gradual increase in the synovial fluid dilution led to an equivalent increase in alpha-defensin level, which was not seem in the aseptic cases. Both 1:1000 and 1:5000 dilutions presented satisfactory results to differentiate infected and aseptic cases. Further analyses were performed using 1:1000 and 1:5000 for all 40 samples. The 1:1000 dilution resulted in a sensitivity of 88.2% (95%CI, 66%-98%) and specificity of 95.7% (95%CI, 79%-99%), whereas the 1:5000 dilution presented a sensitivity of 94.1% (95%CI, 73%-99%) and a specificity of 100% (95%CI, 86%-100%).
Research conclusions
Synovial fluid dilution appears to influence the alpha-defensin ELISA results. Dilutions of 1:5000 showed the best performance for the diagnosis of knee PJI.
Research perspectives
The results of this current study may set the basis for more reliable and reproducible alpha-defensin ELISA during PJI investigation, contributing to the expansion of this technique in different treatment centers worldwide.
FOOTNOTES
Abdo RCT collected the samples; Leite CBG wrote the article; Abdo RCT, Leite CBG, Lima ALLM and Bonfa E contributed to the data analysis; Abdo RCT, Gobbi RG, Lima ALLM, Bonfa E, Pécora JR and Demange MK contributed to the intellectual concept and design of the study; Pasoto SG performed the laboratory tests and contributed to the strategy for alpha-defensin analysis according to its dilution; Leon EP conducted the laboratory tests; Gobbi RG reviewed the article.
I am going to break it, answered the little hare; but of course he had done it on purpose, as he wanted to fix Big Lion s tail so firmly to the hut that he would not be able to move
The study was approved by the local Institutional Review Board, No. 71039317.3.0000.0068.
Changes in synovial fluid dilution for ELISA had an important influence on the determination of alphadefensin levels. Based on the cutoff value of 5.2 mg/L, dilutions of both 1:1000 and 1:5000 were adequate to support the diagnosis of TKA infection. The 1:5000 dilution showed the best performance in separating the infection and the aseptic cases, making it the most reliable dilution during knee PJI investigation. Therefore, the results of this study lay the foundation for a more reliable and reproducible alpha-defensin ELISA during the investigation of PJI, contributing to the expansion of this technique to different treatment centers worldwide.
As the bamboos became thinner, he found himself opposite to a beautiful garden, in the centre of which stood a tiny spick-and-span little house, and out of the house came a lovely maiden10, who unlatched the gate and invited him in the most hospitable11 way to enter and rest
All authors report no relevant conflict of interest for this article.
There is no additional data available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Brazil
Rodrigo Calil Teles Abdo 0000-0002-9423-6246; Riccardo Gomes Gobbi 0000-0002-1715-4343; Chilan Bou Ghosson Leite 0000-0002-8386-3121; Sandra Gofinet Pasoto 0000-0002-7343-6804; Elaine Pires Leon 0000-0001-9457-3317; Ana Lucia Lei Munhoz Lima 0000-0002-2396-9880; Eloisa Bonfa 0000-0002-0520-4681; José Ricardo Pécora 0000-0003-1621-5252; Marco Kawamura Demange 0000-0003-1999-9478.
Wu YXJ
How beautiful it looks with its tongue stretched out like that! It was a long night, but the Snow-man did not find it so; there he stood, wrapt in his pleasant thoughts, and they froze, so that he cracked
A
But, good heavens, it s nothing but a donkey! A donkey! repeated Simon, you don t mean to say so; if a single other person tells me that, I ll make him a present of the wretched animal
The smith took his sentry coat and wrapped it round her; then she dried her tears, and took his hand and thanked him, and said that he had now freed her from all the sorcery that had been in her from her birth, and which had come over her again when her father broke the command against seeing her until she had completed her fourteenth year
Wu YXJ
 World Journal of Orthopedics2022年8期
World Journal of Orthopedics2022年8期
- World Journal of Orthopedics的其它文章
- Anterolateral complex of the knee: State of the art
- Social media growth of orthopaedic surgery residency programs in response to the COVlD-19 pandemic
- Fluctuation of visual analog scale pain scores and opioid consumption before and after total hip arthroplasty
- Functional and clinical outcome with modified lateral approach total hip arthroplasty in stiff hips with ankylosing spondylitis
- Higher cost of arthroplasty for hip fractures in patients transferred from outside hospitals vs primary emergency department presentation
- Risk modeling of femoral neck fracture based on geometric parameters of the proximal epiphysis