
Epidemiology of inflammatory bowel diseases in the state of Rio Grande do Sul, Brazil
2022-08-13 07:04:52EpidemiologyofinflammatoryboweldiseasesinthestateofRioGrandedoSulBrazil
World Journal of Gastroenterology 2022年30期
Epidemiology of inflammatory bowel diseases in the state of Rio Grande do Sul, Brazil
Abstract
Key Words: Inflammatory bowel diseases; Crohn’s disease; Ulcerative colitis; Epidemiology; Incidence;Prevalence
lNTRODUCTlON
Inflammatory bowel diseases (IBDs) are characterized by a chronic inflammatory process that compromises the digestive tract. The main presentations are Crohn’s disease (CD) and ulcerative colitis(UC), which are chronic idiopathic diseases causing inflammation of the gastrointestinal tract, with individual clinical and pathophysiological characteristics[1-3]. Children and young adults are more commonly affected[4]. Although uncommon, the chronicity, severity, progression, and morbidity of IBDs can significantly affect the patient’s quality of life and are associated with an increased risk of hospitalizations and surgery[3,4].
IBDs are contemporary health conditions of industrialized societies. The prevalence of IBDs continues to increase steadily in Western countries, and their incidence is growing in newly industrialized countries. The global spread of IBDs seems to be associated with the Westernization of human diets and environments, affecting the gut microbiota and increasing the risk of IBDs in genetically susceptible individuals. It is therefore important to deepen our understanding of these events to delay the progression of IBDs[5].
Despite the paucity of population-based studies from low- and middle-income countries, epidemiological studies of IBDs have shown increased incidence and prevalence of CD and UC in different parts of the world. The increasing epidemiology of IBDs in newly industrialized countries in Latin America resembles that of high-income countries. Although a stabilization of incidence rates has been observed in many Western countries, the global burden of IBDs is still high, with an estimated prevalence exceeding 0.3% of the population in North America and Europe and 0.7% in Canada in 2018[6].
In newly industrialized countries, obstacles to conducting epidemiological studies of IBDs include the lack of disease surveillance systems and reliable unified health care databases, which are available in high-income countries. In countries of continental dimensions with economic problems such as Brazil,an additional challenge is the country’s generally disorganized health care system, which can result in inadequate records and, consequently, few population-based studies[6]. In this respect, Rio Grande do Sul (RS), the southernmost state of Brazil with the country’s fifth largest population, still does not have a specific study on the epidemiology of IBDs. Therefore, the purpose of this study was to estimate the incidence and prevalence of IBDs in the state of RS.
MATERlALS AND METHODS
Study design
This is a cross-sectional descriptive observational study. All patients who had initiated treatment for IBD and met the inclusion criteria for the free drug distribution program of the state of RS between 2014 and 2019 were included. Drugs for the treatment of CD and UC are dispensed by the specialty pharmacy [Farmácia de Medicamentos Especializados(FME), or FME for short, in Portuguese] according to clinical protocols and therapeutic guidelines published by the Brazilian Ministry of Health. In Brazil,access to care is provided through private health insurance or the Unified Health System, which is a universal health care system funded by federal taxes and operated by state or municipal governments that includes the public provision of core physician and hospital services without copayments or patient charges. Approximately 22% of the population in the state of RS have private health insurance and only occasionally use the public health system. Therefore, because the FME is a government program within the Brazilian Unified Health System, it is responsible for supplying specialty medications to approximately 78% of the state population, all of them users of the public health system. Data from private health insurance companies are not included in this study.
Demographic characteristics and incidence and prevalence data were obtained from registration or renewal records of the FME. We requested from the State Health Department and its affiliated School of Public Health the data of patients included in the specialty medication distribution programs of the FME, which were provided through administrative and judicial means[7].
As variables to be analyzed, we included CD or UC diagnosis using International Classification of Diseases codes K50 and K51, date of treatment initiation, sex, and age.
Data analysis
Quantitative variables, such as age, were described using mean, standard deviation, and range.Categorical variables were expressed as counts and percentages. Disease prevalence and incidence were estimated by dividing the annual case notifications by the total estimated population of that year and presented as cases per 100000 population. Binomial distribution was used for obtaining 95% confidence intervals. All comparisons between rates assumed the binomial distribution and were based on the chisquare test. Findings withP≤ 0.05 were deemed statistically significant. All estimates of incidence and prevalence were calculated considering the population of the state of RS between 2014 and 2019[8]. Data analysis was conducted using IBM-SPSS, version 25.0.
Ethical considerations
This study did not involve the collection of biological material from participants. Data obtained with the data collection instrument were coded to preserve the participants’ privacy and anonymity. All investigators signed a data use agreement.
The study was conducted after approval by the Research Ethics Committees of Pontifícia Universidade Católica do Rio Grande do Sul, Certificate of Presentation for Ethical Appreciation No. 25551019900005336, and of the State Health Department and its affiliated School of Public Health, Certificate of Presentation for Ethical Appreciation No. 25551019930015312. The study followed the guidelines of Resolution No. 466/12 of the Brazilian National Health Council and the Brazilian General Data Protection Law No. 13709.
RESULTS
This study involved 1082 patients with IBD of a total population of 11377239 people. Of these, 784(72.45%) had CD and 298 (27.54%) had UC.
Age
Patient age ranged from 1 to 91 years, with a mean of 41 years and standard deviation of 15 years. The highest IBD incidence was between 20 and 60 years of age, and patients were mostly aged 30-40 years(Figure 1A). The highest incidence occurred between the ages of 30 and 40 years for CD, and between the ages of 50 and 60 years for UC. UC affected a higher percentage of people aged 40 years or more (P<0.01), whereas CD affected a higher percentage of people under 40 years of age (P< 0.01) (Figure 1B).
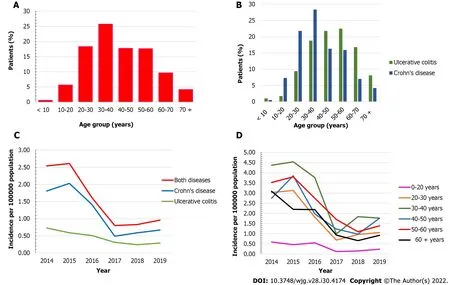
Figure 1 Age distribution and incidence rates of patients with inflammatory bowel diseases. A: Age distribution of patients with inflammatory bowel diseases (IBD) (n = 1082), state of Rio Grande do Sul, Brazil, 2014-2019; B: Age distribution of patients with Crohn’s disease (n = 784) and ulcerative colitis (n = 298),state of Rio Grande do Sul, Brazil, 2014-2019; C: Annual IBD incidence rates, new cases per 100000 population/year in the state of Rio Grande do Sul (Brazil), 2014-2019; D: Annual IBD incidence rates by age group, new cases per 100000 population/year in the state of Rio Grande do Sul (Brazil), 2014-2019.
Sex
Of all patients with IBD, 622 (57.5%) were female and 460 (42.5%) were male (female-to-male ratio of 1.35:1.00;P< 0.001).
Considering CD only, 432 (55.10%) patients were female and 352 (44.89%) were male (female-to-male ratio of 1.23:1.00;P< 0.001). For UC, 190 (63.75%) were female and 108 (36.25%) were male (female-tomale ratio of 1.76:1.00;P< 0.001).
Incidence and prevalence
Overall, IBD prevalence was 9.51 per 100000 population during the study period (2014-2019), of which 6.89 corresponded to CD and 2.62, to UC. Table 1 shows the sex distribution of prevalence for each disease.
Figure 1C shows the annual incidence rates of IBD in the state of RS. The mean incidence rate was 1.61, of which 1.17 corresponded to CD and 0.44, to UC.
Table 2 shows annual incidence percentages. There was a 62% reduction in the accumulated incidence between 2014 and 2017 (P< 0.015). A statistically significant reduction in incidence was observed when comparing 2014 and 2019 (P< 0.001).
Figure 1D shows that, when listing annual incidence rates by age group, all groups showed reductions in 2017, with increases in the following years.
DlSCUSSlON
Historical data on the geographical distribution of IBDs worldwide have shown higher incidence and prevalence rates in high-income countries with predominantly White populations. More recently, IBDs have shown an increasing frequency in all continents, including low- and middle-income countries[2].
In Brazil, IBDs are not notifiable diseases. Therefore, data on the incidence and prevalence of CD and UC are scarce, and health systems lack adequate records. These data would be useful for better organization and political and economic planning of the public health system[9,6].

Table 1 Prevalence of inflammatory bowel diseases in the state of Rio Grande do Sul between 2014 and 2019 (per 100000 habitants)
Table 2 Annual percentages of incidence rates
In North America, 6.30 to 23.82 new cases per 100000 population are estimated per year for CD, and 8.8 to 23.14 new cases per 100000 population for UC. Prevalence rates are far higher than those in Brazil,with 96.3 to 318.5 cases/100000 population for CD and 139.8 to 286.3 cases/100000 population for UC[1,10].
A cohort study published in the United Kingdom reported incidence and prevalence rates much higher than those in Brazil between 2000 and 2018. The study estimated incidence rates of 28.6, 10.2, and 15.7/100000 population for IBD, CD, and UC, respectively, and prevalence rates of 725, 276, and 397/100000 population[11].
In the state of RS, we observed a predominance of CD during the study period (CD 72.54% and UC 27.54%), which differs from previous studies published in Brazil reporting a predominance of UC[2,3,12,13]. This is consistent with a study conducted in the Southeast region of Brazil by Souzaet al[14], who reported an increase in CD cases in comparison with UC. These differences between countries and regions may reflect differences in environmental risk factors and genetic predispositions, such as those observed in Europe, where the incidence of NOD2 mutations appears to be higher in the central part of the continent, corresponding to areas with a higher proportion of CD cases[15].
According to the present study, the state of RS had a mean annual IBD incidence rate of 1.61 new cases per 100000 population/year (CD = 1.17 and UC = 0.44 new cases per 100000 population/year)between 2014 and 2019, which is consistent with the results reported by Kaplanet al[5] in a systematic review considering 147 studies on IBD worldwide. This comprehensive review demonstrated a CD incidence of 0-3.5 new cases per 100000 population/year, and an UC incidence of 0.19-6.76 new cases per 100000 population/year in Brazil[1]. In comparison, the systematic review by Selvaratnamet al[16]on the epidemiology of IBD in South America showed higher incidence rates, ranging from 4.3 to 5.3 per 100000 population/year for UC and from 0.74 to 3.5 per 100000 population/year for CD between 1990 and 2018. Similarly, a Brazilian study conducted in the state of Sao Paulo reported higher incidence rates than those found in the state of RS, with rates of 6.14 for CD and 7.16 for UC (per 100000 population/year)[3].
Regarding IBD prevalence, the mean rate observed during the study period (2014-2019) was 9.51 cases per 100000 population, of which 6.89 corresponded to CD and 2.62, to UC. Prevalence in the state of RS was higher than that reported for Brazil in a systematic review by Nget al[1], with rates ranging from 0.9 to 6.75 cases/100000 population for CD and from 2.42 to 21 cases/100000 population for UC.Prevalence was also higher in a systematic review on IBD epidemiology conducted in South America,reaching 15-24.1/100000 population for UC and 2.4-14.1/100000 population for CD[16]. Similarly, in the Brazilian study by Gaspariniet al[3], overall prevalence rates were 24.3 for CD and 28.3 for UC per 100000 population.
If we were to analyze the state of RS according to the epidemiological transition theory proposed by Gilaad G Kaplan and Joseph W Windsor in 2021, where each region of the world is at an epidemiological stage (Emergence, Acceleration in Incidence, Compounding Prevalence, and Prevalence Equilibrium), RS would be in the Compounding Prevalence stage, where a steady increase in the population living with IBD is observed despite stabilization or even a decrease in incidence[17].
Regarding patient age, studies show a clear predominance of IBD in individuals aged 20 to 50 years.In our study, the mean age was 41 years. The highest IBD incidence was between 20 and 60 years of age,and patients were mostly aged 30-40 years. The highest incidence was at 30-40 years of age for CD, and at 50-60 years of age for UC. UC showed a trend toward an increased incidence among patients aged 50 to 60 years, and these results are consistent with those of national and international studies[3,11]. A limitation of this variable is that patients were selected through the FME, which provides the age that the patients begin to receive the free specialty medications rather than their age at diagnosis.
Regarding the sex distribution of patients with IBD, we observed a predominance of female patients for both CD and UC, which is consistent with the Brazilian studies conducted by Victoriaet al[12] in the state of Sao Paulo and Lima Martinset al[13] in the state of Espírito Santo. However, our findings differ from those reported in the state of Piauí by Parenteet al[2], who found a male-to-female ratio of 1.2:1.0 for patients with CD, but with no significant association when considering sex in statistical analyses.Patients with UC, on the other hand, were mostly female (male-to-female ratio of 1.8:1.0, statistically significant)[2].
CONCLUSlON
Based on the methodology used in this study, our results demonstrated an IBD prevalence of 9.51% and incidence of 1.61 per 100000 population in the state of RS between 2014 and 2019. The patients were predominantly female, and CD was more prevalent than UC. Our prevalence rate was similar to that reported in previous Brazilian studies. Mean CD and UC incidence rates were, respectively, 1.17 and 0.44 new cases per 100000 population, decreasing until 2017 and increasing afterwards. Women were more affected than men by both CD and UC. IBD occurred more frequently in major urban centers,where the referral centers that care for patients with IBD are often located. The highest IBD incidence was observed in patients aged 20 to 60 years, predominantly between the ages of 30 and 40 years; this was slightly higher than the mean values reported in previous studies.
This is the first study to estimate IBD incidence and prevalence in the state of RS. Our findings suggest that detailed studies in this field are needed to properly understand in which epidemiological stage the state of RS currently is. We believe that the difficulty in keeping accurate epidemiological records and the consequent underestimation of disease burden result from a disorganized health care system, associated with economic problems, inadequate records, lack of population-based studies, and the inaccurate diagnosis of IBD as an infectious disease before the proper knowledge of CD and UC.
ARTlCLE HlGHLlGHTS
Research conclusions
The most relevant of the following questions should be briefly answered: What are the new theories that this study proposes? This study showed a similar IBD prevalence to other Brazilian studies and a decreasing incidence. What are the new methods that this study proposed? We propose that studies covering patients from both public and private health sectors should be conducted.
Research perspectives
Future studies should include a larger sample to provide a more reliable understanding of the real epidemiology of IBDs in the state of RS.
ACKNOWLEDGEMENTS
We thank the RS State Health Department pharmacy and its affiliated School of Public Health for making their data available, and CAPES for the funding that contributed to the improvement of higher education.
FOOTNOTES
Author contributions:Cassol OS contributed to data collection, investigation, writing-original draft, and statistical analysis; Zabot GP, Saad-Hossne R, and Padoin A contributed to writing-review and editing.
Supported bythe Coordenação de Aperfeiçoamento de Pessoal de Nível Superior-Brasil (CAPES)-Finance Code 001.
lnstitutional review board statement:This study was performed after approval by the Research Ethics Committee of Pontifícia Universidade Católica do Rio Grande do Sul, Certificate of Presentation for Ethical Appreciation No.25551019900005336; and the ESP/SES/RS Research Ethics Committee, Certificate of Presentation for Ethical Appreciation 25551019930015312; this work respected the guidelines of Resolution No. 466/12 of the National Health Council and Law No. 13709 of the General Personal Data Protection Law.
lnformed consent statement:This study did not involve the collection of biological material from participants. Data obtained with the data collection instrument were codified, aiming to preserve the participants’ privacy and anonymity. A data use agreement form was signed.
Conflict-of-interest statement:There are no conflicts of interest to report.
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Brazil
ORClD number:Ornella Sari Cassol 0000-0003-0867-6593; Gilmara Pandolfo Zabot 0000-0002-1253-4945; Rogerio Saad-Hossne 0000-0002-8166-0304; Alexandre Padoin 0000-0002-9754-4818.
S-Editor:Chen YL
L-Editor:A
P-Editor:Chen YL
 World Journal of Gastroenterology2022年30期
World Journal of Gastroenterology2022年30期
- World Journal of Gastroenterology的其它文章
- Alcohol-related diseases and liver metastasis: Role of cell-free network communication
- Benefits of minimally invasive surgery in the treatment of gastric cancer
- Contrast-enhanced ultrasound of a traumatic neuroma of the extrahepatic bile duct: A case report and review of literature
- ANGPT: Angiopoietin; VEGFA: Vascular endothelial growth factor; PGF: Placental growth factor; AFP: Alpha-fetoprotein; IQR: Interquartile range; SD:Standard deviation, SE: Standard error.
- Network meta-analysis of randomized controlled trials on esophagectomies in esophageal cancer: The superiority of minimally invasive surgery
- Hepatocellular carcinoma, decompensation, and mortality based on hepatitis C treatment: A prospective cohort study