
Factors influencing physician's behavioral intention to use Traditional Chinese Medicine to treat coronavirus disease 2019 based on the theory of planned behavior
2022-07-20 08:19:34CHENHuangSHILushaoboSHIZengpingXIAYiWANGDong
CHEN Huang,SHI Lushaobo,SHI Zengping,XIA Yi,WANG Dong
CHEN Huang,General Office,the People’s Government of Guangdong Province,Guangzhou 510045,China;the Public Health Service System Construction Research Foundation of Guangzhou 510515,China
SHI Lushaobo,SHI Zengping,XIA Yi,WANG Dong,School of Health Management,Southern Medical University,Guangzhou 510515,China;the Public Health Service System Construction Research Foundation of Guangzhou,Guangzhou 510515,China
Abstract OBJECTIVE:To explore the factors influencing physicians' intentions to use Traditional Chinese Medicine (TCM) to treat coronavirus disease 2019(COVID-19).METHODS:A cross-sectional,self-report online survey was conducted from March 16,2020,to April 2,2020,in China.Participants were recruited through convenience and snowball sampling.Data were collected by using a self-designed questionnaire based on the Theory of Planned Behavior.Structural equation modeling was used for data analysis.RESULTS:A total of 494 physicians were enrolled in this study.Overall,the model explained 75.4% and 75.5% of the total variance in intention and attitude,respectively.Specifically,attitudes (β=0.467,P <0.001),past behavior (β=0.384,P <0.05),subjective norms (SN) (β=0.177,P <0.001),and perceived behavioral control(PBC) (β=0.133,P <0.05) significantly affected physicians' intention to use TCM.Cognition (β=0.606,P<0.001) and PBC (β=0.569,P <0.01) significantly influenced physicians' attitudes toward using TCM.SN (β=0.064,P=0.263) was not a factor affecting attitude.CONCLUSION:Physicians’ intention to use TCM was significantly associated with attitude,past behavior,PBC,and SN.The findings may not only be useful for understanding the influencing factors and paths of physicians’ intention to use TCM to treat COVID-19 but also provide a reference for health authorities and policymakers to promote physicians to utilize TCM.
Keywords:COVID-19;Medicine,Chinese Traditional;physicians;intention;behavior control
1.INTRODUCTION
Coronavirus disease 2019 (COVID-19),caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),has affected millions of people and was defined as a pandemic by the World Health Organization (WHO).1Currently,the disease has become one of the leading causes of death worldwide and has imposed a heavy toll on public health as well as the global economy.2The symptoms of COVID-19 include fever,dry cough,and general fatigue.3A key goal to control the disease is to achieve an increased cure rate and reduce mortality by providing effective treatment.To date,no specific therapeutic agents or effective treatments for COVID-19 have been reported.However,numerous clinical practices have suggested that traditional Chinese medicine (TCM) plays an important role in the prevention and treatment of COVID-19.4–6Generally,TCM enhances human resistance to epidemics by regulating internal functions of the body.It's worth noting that the TCM scheme has been officially included in China’s National COVID-19 Diagnostic and Treatment Guideline.7
Physicians are key providers of frontline medical services and are directly involved in the treatment of COVID-19 patients.If they do not have a comprehensive understanding of TCM,or have no awareness of using TCM,it is difficult to fully understand the role of TCM in the prevention and treatment of COVID-19.Because of this,the key to promoting the application of TCM lies in physicians.Only when physicians can correctly understand,believe,and use TCM,can the promotion and application of TCM be promoted.Although physicians' attitudes (ATT) toward TCM have been reported in other research,8-11our understanding of physicians’ intentions and attitudes regarding TCM to treat COVID-19 remains limited.To promote the rational use of TCM for COVID-19,it is necessary to explore the factors that influence physicians' intention to use TCM.
One way to achieve this goal is to apply a (TPB).TPB is a theory that indicates that an individual’s actual behavior is affected by behavioral intention,which is measured by three basic components:attitudes (i.e.,positive or negative evaluation of behaviors),subjective norms (SN) (i.e.,perception of social pressure from general or specific important persons),and perceived behavioral control (PBC) (i.e.,perceived ease or difficulty of performing a particular behavior).12In addition,attitude,as we know,is affected by SN and PBC in the TPB model.13-15Currently,TPB is a classic theory that explains behavioral mechanisms.It has been widely used in transportation,agriculture,16-18and healthrelated fields.19–22For example,TPB was used as the theoretical basis to explore the behavioral determinants associated with vaccination uptake in the population.23Here,we aimed to investigate the mechanism and influencing factors for physicians’ intentions to use TCM based on TPB.The findings may not only be useful for understanding the influencing factors and paths of physicians' intention to use TCM to treat COVID-19,but also provide a reference for health authorities and policymakers to promote physician utilization of TCM.
2.METHODS
2.1.Study design and participants
A web-based cross-sectional self-report survey using the‘Questionnaire Star’ platform (https://www.wjx.cn/) was conducted between March and April 2020.The inclusion criteria were as follows:(a) licensed physicians and (b)had access to the Internet via a cell phone or computer.The exclusion criteria were as follows:(a) incomplete questionnaire;(b) answers with logical errors,for example,the answers to all items were the same.To improve response rates,participants who shared questionnaire website links with others were offered a chance to receive a red envelope reward.In addition,sample size calculations were based on Hairet al.'s24recommendation of 15-20 observed values per research variable.This study consisted of six constructs (totaling 25 items),so the minimum sample size was 375 (25 ×15).The paired sampling method was used.A total of 550 participants completed the questionnaire;among them,29 Western medicine physicians and 27 TCM physicians were excluded due to the inclusion and exclusion criteria.At the end,data from 494 participants were used in the analysis.The study was approved by the Ethics Committee of the Southern Medical University(Ref ID:NFYKDX002).
2.2.Conceptual model and Hypotheses
The conceptual model used in this study was based on the TPB (Figure 1).The dependent variable was physicians’ intentions to use TCM.Furthermore,we defined physicians’ cognition of TCM as a cognition (C)variable,which affects their attitudes toward TCM.In other words,if they believe that TCM is helpful,physicians will be inclined to choose it to treat COVID-19.Additionally,past behavior (PB) has been shown to exert significant effects on future behavior.25Therefore,with the help of the TPB structure,ATT,SN,PBC,PB,and cognition were incorporated into the conceptual model as the dependent variables.Based on these models and variables,the following six hypotheses are proposed:Hypothesis 1 (H1):C positively affects physicians’attitudes toward TCM.
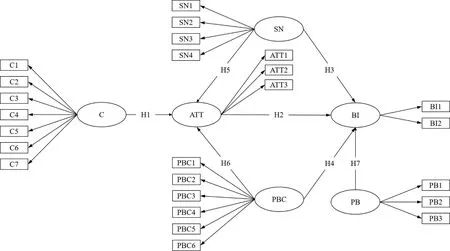
Figure 1 Constructs of conceptual model
Hypothesis 2 (H2):Attitude positively affects physicians’intentions to use TCM.
Hypothesis 3 (H3):SN positively affects physicians’intention to use TCM.
Hypothesis 4 (H4):PBC positively affects physicians’intentions to use TCM.
Hypothesis 5 (H5):SN positively affects physicians’attitudes toward TCM.
Hypothesis 6 (H6):PBC positively affects physicians’attitudes toward TCM.
Hypothesis 7 (H7):PB positively affects physicians’intentions to use TCM.
2.3.Measurement
In our study,the self-designed questionnaire based on the TPB consisted of two parts:demographic characteristics data and data related to the intention to use TCM.The scope and precision of the questionnaire were evaluated by a panel of experts in TCM,public health,and psychology.According to the suggestions,three questions on the attitude dimension and two questions on the subjective norms dimension were deleted.The questionnaire was then pilot tested among 20 physicians,and the internal consistency of the questionnaire was assessed using Cronbach's α.
Finally,there were 25 items in the questionnaire,of which seven were assigned to measure physicians’cognition of TCM (C1-C7),three items were assigned to measure physicians’ attitude towards TCM (ATT1-ATT3),four items were assigned to measure subjective norms of TCM (SN1-SN4),six items were assigned to measure perceived behavior control of TCM (PBC1-PBC6),three items were assigned to measure past behavior of TCM (PB1-PB3),and two items were assigned to measure behavioral intention (BI1-BI2).The construct was measured on a multi-item,five-point Likert scale,ranging from 1 (strongly disagree) to 5(strongly agree).
2.4.Data analysis
After deriving the electronic questionnaire data,statistical indicators,including the frequency,standard deviation,and mean,were calculated to describe the sample characteristics.Subsequently,a Cronbach's α test was conducted to measure the reliability and validity of the questionnaire.In addition,confirmatory factor analysis was used to measure the model´s convergence and discriminant validity.Structural equation modelling(SEM) was used to test the conceptual model and hypotheses.Descriptive statistical analyses and Cronbach's α tests were performed using SPSS version 25 (IBM Corp.,NY,USA).Confirmatory factor analysis and SEM were performed using AMOS version 22 (IBM Corp.,Armonk,NY,USA).
3.RESULTS
3.1.Demographic characteristics
The mean age of the 494 participants was 40.69 years(SD=8.75),and more than half were men (57.09%).The participants were largely from urban areas (n=466,94.33%),married (n=450,91.09%),and educated at tertiary or above (n=472,95.55%).Most participants had an annual family income between 50 000 and 200 000 RMB (n=348,70.45%) (Table 1).
3.2.Reliability and validity tests
Cronbach's α and confirmatory factor analysis (CFA)were used to evaluate the reliability and validity of the measurement model.Table 2 shows the values of Cronbach’s α,Bartlett’s test of sphericity,factor loadings,Kaiser-Meyer-Olkin (KMO) test,composite reliability(CR),and average variance extracted (AVE).Theoretically,the value of Cronbach's α ranges from 0 to 1,which effectively reflects the reliability of the questionnaire.26When the Cronbach’s α was higher than 0.7,the measurement model had sufficient consistency and reliability.27In our study,the Cronbach's α for each construct was greater than 0.900 (0.859-0.960).Regarding the KMO test,except for behavioral intention(0.500),the other values of all constructs were higher than 0.700 (0.767-0.906) and Bartlett’s test of sphericity was statistically significant (P<0.001).Moreover,all standardized factor loads were higher than the minimum standard value of 0.622 (0.622-0.965),indicating that each item had a significant correlation with its corresponding construct.28In terms of confirmatory factor analysis,the results showed that the CR and AVE values of each construct were higher than 0.7 and 0.5,respectively (0.906-0.964,0.583-0.872),suggesting that the measurement model had good composite reliability and convergent validity.29For the square root of AVE(reported in bold on the diagonal of the correlation matrix in Table 3),which is used to measure the discriminative validity of each construct,its value was higher than thecorrelation coefficients with other constructs,demonstrating that the measurement model has desirable discriminative validity.30
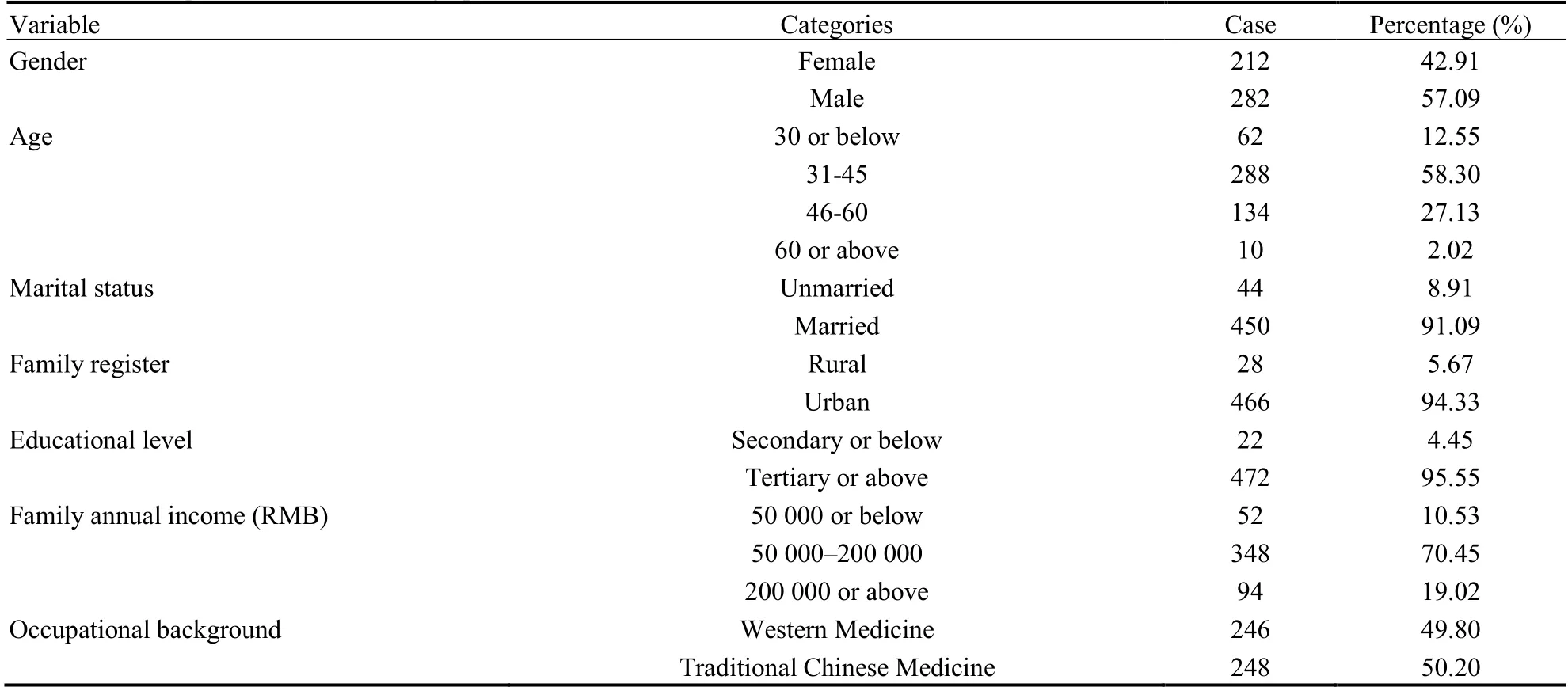
Table 1 Descriptive statistics of demographic characteristics
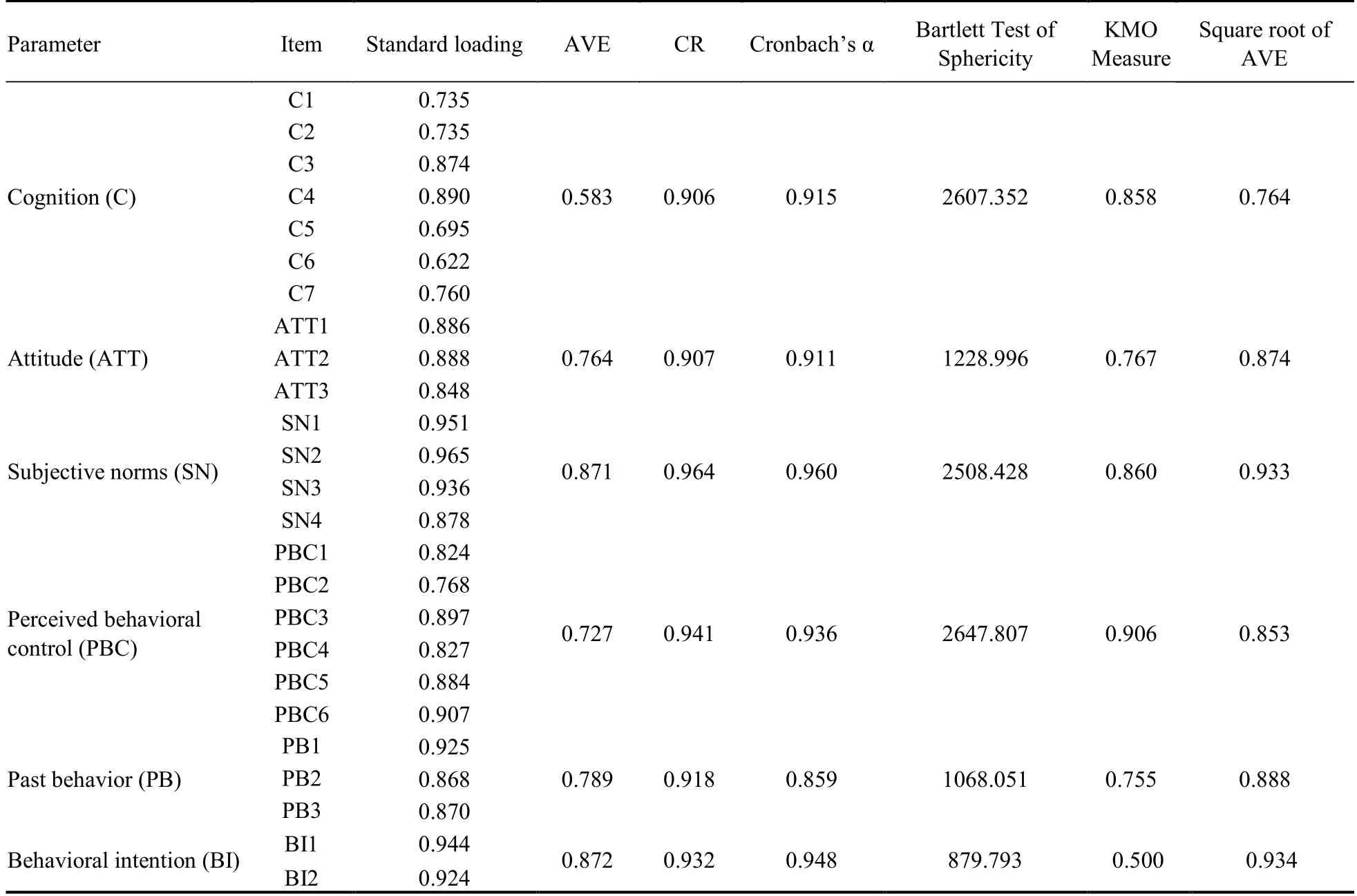
Table 2 Reliability and validity analysis results of the measurement model
3.3.Descriptive Statistics and Correlations
The mean value ranks (from low to high) of the six dimensions in the conceptual model were cognition(mean=3.816,SD=0.676),past behavior (mean=3.887,SD=1.086),subjective norms (mean=3.985,SD=0.892),perceived behavioral control (mean=4.147,SD=0.822),behavioral intention (mean=4.178,SD=0.863),and attitude (mean=4.296,SD=0.759).In addition,the results of the correlation analysis showed a statistically significant correlation between each dimension (P<0.01),and the correlation coefficients ranged from 0.567 to 0.824 (Table 3).Notably,as shown in Table 4,in each dimension,the mean score of Western medicine physicians was lower than that of TCM physicians,and the difference was statistically significant.
3.4.Goodness-of-fit statistics
SEM was used to test the measurement model.Prior to testing the proposed hypothesis,three types of indicators,namely the absolute fitness index (χ2/df,RMSEA,GFI,and AGFI),incremental fitness index (NFI,IFI,CFI),and parsimony fitness index (PNFI,PGFI,PCFI) were calculated to evaluate the overall fit of the model.The results showed that all indicators exceeded the recommended level,31-35indicating that the overall fit of the measurement model was acceptable:χ2/df=4.820 (<5.00),RMSEA=0.088 (<0.10),GFI=0.844 (>0.80),AGFI=0.808 (>0.80),NFI=0.910 (>0.90),IFI=0.927 (>0.90),CFI=0.927 (>0.90),PNFI=0.804 (>0.50),PGFI=0.688 (>0.50),and PCFI=0.819 (>0.50)(Table 5).
3.5.Testing hypotheses
The hypothesis testing results of the SEM analysis are presented in Table 6 and Figure 2.Overall,the model explained 75.5% and 75.4% of the total variance in intention and attitude,respectively.Specifically,C (β=0.606,P<0.001) was the most important factor affecting attitude,followed by PBC (β=0.569,P<0.001).SN (β=0.064,P=0.263) had no effect on attitude.In addition,attitude (β=0.467,P<0.001) was the most important factor affecting behavioral intention,followed by PB (β=0.384,P<0.001),SN (β=0.177,P<0.001),and PBC(β=0.133,P<0.05).As shown in Table 7,among the seven demographic factors,except occupational background,the other six factors had no significant influence on behavioral intention toward TCM.

Table 7 Regression analysis of demographics on TCM behavior intention and its components
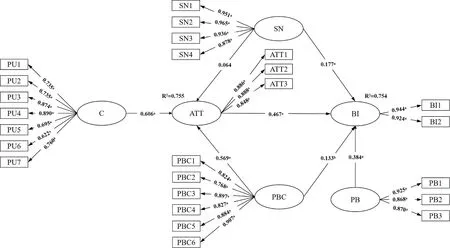
Figure 2 Structural equation model on intention of TCM utilization based on TPB

Table 3 Descriptive statistics,correlation and discriminative validity analysis results
Table 4 Differences in each variable between TCM and Western physicians ()

Table 4 Differences in each variable between TCM and Western physicians ()
Notes:C:cognition;ATT:attitude;SN:Subjective norms;PBC:perceived behavioral control;BI:behavior intention;PB:Past behavior.

Table 5 Structural equation model fitting index analysis results

Table 6 Results of structural equation modeling analysis
4.DISCUSSION
To investigate the factors influencing TCM utilization by Chinese physicians during the COVID-19 pandemic,the framework of the TPB was used in this study.In addition,SEM was performed to test the proposed hypotheses and analyze the interrelationships among the influencingfactors.The results suggest that physicians’ intention to use TCM was most affected by attitudes toward TCM,followed by PB,SN,and PBC.In addition,C and PBC were significant predictors of physicians’ attitudes toward TCM.However,SN had no effect on the attitudes.All hypotheses,except H5,were successfully confirmed in our proposed structural model,suggesting that the TPB is an acceptable theoretical basis for this study.
The present study is an empirical investigation of physicians’ intentions to use TCM during the COVID-19 pandemic.Our results showed that attitude,PBC,and SN were positively associated with physicians’ intentions to use TCM for the treatment of COVID-19.This was in line with the findings of previous research in the field of other health technology adoption.36,37Additionally,the four factors in the SEM model accounted for 75.4% of the variance in physicians’ intention to use TCM,indicating that the proposed constructs were the main reasons for physicians' intention to use TCM.Among the demographic factors,only professional background was significantly related to intention.In most cases,doctors with occupational backgrounds in TCM use TCM first or tend to use TCM.Syndrome differentiation and treatment are the core of TCM diagnosis and require a certain professional background.This may be the main reason why physicians with a professional background in Western medicine do not know how to use TCM or are reluctant to use it.Furthermore,the nature of the hospital for which a doctor works and the prescribing rights of physicians with different professional backgrounds are also critical to the use of TCM.
It is worth noting that C was the strongest predictor of attitude towards TCM,with PBC also predicting attitude,but SN was not a predictor.In other words,it seems that the positive attitude toward TCM often appears in physicians who have a positive perception of TCM,perceive the facilitating conditions and reputation rewards of using TCM,or perceive the expectations of their friends and co-workers.38,39In addition,we found that the mean C was the lowest among all variables,indicating that more attention should be paid to promoting physicians’ positive awareness of TCM.Compared with TCM physicians,Western physicians must focus more on TCM.
PBC reflected the degree of physicians’ perception of the ease or difficulty of performing TCM and whether they could implement this behavior.In this study,four observed variables were used to measure physicians’PBC:professional human resource reserve,availability of hospital facilities,convenient access to information,and sense of self-efficacy.The results of our study showed that both the convenience of information acquisition and the professional human resources reserve were the two strongest factors affecting physicians’ PBC,which indicated the importance of the timeliness of epidemic treatment and professionalism of TCM.Therefore,enhancing physicians’ PBC from these perspectives will help promote the formation of TCM intentions.
The SN can be divided into injunctive and descriptive norms.Injunctive norms refer to important social referents,including friends,relatives,and colleagues,supporting or opposing a certain behavior,whereas descriptive norms refer to implementing or prohibiting this behavior.In our study,both injunctive norms and descriptive social norms were proven to be direct antecedents of SN,which is in line with previous findings.40,41Additionally,our findings showed that SN was positively related to physicians’ intention to use TCM,which is consistent with our previous study.42However,the path coefficient of SN in the TCM attitude prediction was not statistically significant.In our opinion,these results could be due to the professionalism of physicians. For example,a high degree of professionalism makes them less affected by important social referents.Nevertheless,this does not mean that the SN is not important in determining TCM intentions.Thus,further research should focus on the important role of SN in predicting intention,although the path coefficients are weak.
This study has several limitations.First,the crosssectional design of this study did not reveal a causal relationship between research variables.This was an anonymous questionnaire;therefore,it was not possible to track these participants and repeat the questionnaire to confirm the hypothesis.Future longitudinal and prospective studies may help to solve this problem.Second,our study used a self-reported questionnaire to measure related variables,which may have led to overestimation of the results.In addition,data were collected shortly after the COVID-19 outbreak in China.During this period,no particularly effective treatment was found worldwide,and the Chinese government has strongly encouraged the use of TCM.These factors may have also affected the results.Finally,because an online questionnaire was used to conduct this study,physicians who did not have Internet access were not included in the study,which limited the generalizability of the findings.
5.ACKNOWLEDGEMENTS
The authors would like to thank the participants for their involvement in this study.
6.REFERENCES
1.Aleem A,Akbar Samad AB,Slenker AK.Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus(COVID-19) .StatPearls Publishing,Treasure Island (FL) online,2022-05-12,cited 2022-06-10. Available from URL:https://www.ncbi.nlm.nih.gov/books/NBK570580/.
2.Awadasseid A,Wu Y,Tanaka Y,Zhang W.Current advances in the development of SARS-CoV-2 vaccines.Int J Biol Sci 2021;17:8-19.
3.Tsai SC,Lu CC,Bau DT,et al.Approaches towards fighting the COVID-19 pandemic (Review).Int J Mol Med 2021;47:3-22.
4.Shi YH,Huang YF,Wang WY,Yang L,Zhou H,Sang Z.Analysis on the current quality standards of Chinese materia medica used in COVID-19 prevention and treatment.Pharmacol Res 2020;160:105074.
5.Zhou LP,Wang J,Xie RH,et al.The effects of Traditional Chinese Medicine as an auxiliary treatment for COVID-19:a systematic review and Meta-analysis.J Altern Complement Med 2021;27:225-37.
6.Ren W,Liang P,Ma Y,et al.Research progress of Traditional Chinese Medicine against COVID-19.Biomed Pharmacother 2021;137:111310.
7.Ho LTF,Chan KKH,Chung VCH,Leung TH.Highlights of Traditional Chinese Medicine frontline expert advice in the China national guideline for COVID-19.Eur J Integr Med 2020;36:101116.
8.Chen KJ,Lu AP.Situation of integrative medicine in China:results from a national survey in 2004.Chin J Integr Med 2006;12:161-5.
9.Yu HY,Wang XQ,Zhang Y,Liu J,Lin HS.Application status of Chinese medicine on cancer rehabilitation:a preliminary questionnaire survey.Chin J Integr Med 2020;26:890-6.
10.Mcquade JL,Meng ZQ,Chen Z,et al.Utilization of and attitudes towards Traditional Chinese Medicine therapies in a Chinese cancer hospital:a survey of patients and physicians.Evid Based Complement Alternat Med 2012;2012:504507.
11.Huber BM,Schoen-Angerer TV,Hasselmann O,Wildhaber J,Wolf U.Swiss paediatrician survey on complementary medicine.Swiss Med Wkly 2019;149:w20091.
12.Ajzen I.The theory of planned behavior.Organizational behavior and human decision processes 1991;50:179-211.
13.Lim HR,An S.Intention to purchase wellbeing food among Korean consumers:An application of the theory of planned behavior.Food Qual Prefer 2021;88:104101.
14.Soorani F,Ahmadvand M.Determinants of consumers’ food management behavior:applying and extending the theory of planned behavior.Waste Management 2019;98:151-9.
15.Davis KC,Jacques-Tiura AJ,Stappenbeck CA,et al.Men’s condom use resistance:Alcohol effects on theory of planned behavior constructs.Health Psychol 2016;35:178-86.
16.Boissin C,Al Maniri AA,Al-Azri AS,Hasselberg M,Laflamme L.Determinants of speeding among new generations of car drivers from the Arabian Peninsula.An investigation based among Omani drivers using the theory of planned behaviour.PLoS One 2019,14:e0226441.
17.Cheah I,Sadat Shimul A,Liang J,Phau I.Drivers and barriers toward reducing meat consumption.Appetite 2020;149:104636.
18.Bogers RP,Brug J,Assema PV,et al.Explaining fruit and vegetable consumption:The theory of planned behaviour and misconception of personal intake levels.Appetite 2004;42:157-66.
19.He Y,Yang F,Mu D,Xing Y,Li X.Examination of psychosocial predictors of Chinese hospital pharmacists’ intention to provide clinical pharmacy services using the theory of planned behaviour:a cross-sectional questionnaire study.BMJ Open 2016;6:e012775.
20.Muhammed A,Khuan L,Shariff-Ghazali S,Said SM,Hassan M.Predictors of midwives’ intention to provide planned home birth services to low-risk women:a theory of planned behaviour approach.Midwifery 2019;73:62-8.
21.Deng Q,Lu J,Zeng Z,Zheng Y,Liu W.Dynamics of Health Technology Diffusion in the Integrated Care System (DHTDICS):A development and validation study in China.Risk Manag Healthc Policy 2021;14:331-44.
22.Espada JP,Morales A,A Guillénriquelme,et al.Predicting condom use in adolescents:a test of three socio-cognitive models using a structural equation modeling approach.BMC Public Health 2016;16:35.
23.Shmueli L.Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model.BMC Public Health 2021;21:84.
24.Hair JF,Babin BJ,Black WC,Anderson RE,Tatham RL.Multivariate data analysis.,6th ed.Upper Saddle River.New Jersey:Pearson Prentice Hall,2006:460-1.
25.Ouellette JA,Wood W.Habit and intention in everyday life:the multiple prodcess by which past behavior predicts future behavior.Psychol Bull 1998;124:54-7.
26.Wu Z,Jiang M,Li H,Luo X,Li X.Investigating the critical factors of professionals’ BIM sdoption behavior based on the theory of planned behavior.Int J Environ Res Public Health 2021;18:3022.
27.Sun Y,Qin B,Hu Z,et al.Predicting mask-wearing behavior intention among international students during COVID-19 based on the theory of planned behavior.Ann Palliat Med 2021;10:3633647.
28.Chin WW,Gopal A,Salisbury WD.Advancing the theory of adaptive structuration:The development of a scale to measure faithfulness of appropriation.Inf Syst Res 1997;8:342-67.
29.Bagozzi RP,Yi Y.On the evaluation of structural equation models.JAMS 1988;16:74-94.
30.Fornell C,Larcker DF.Structural equation models with unobservable variables and measurement error:algebra and statistics.J Mark Res 1981;18:382-8.
31.Doll WJ,Xia W,Torkzadeh G.A confirmatory factor analysis of the end-user computing satisfaction instrument.MIS Quarterly 1994;18:453-61.
32.Arpaci I,Baloğlu M.The impact of cultural collectivism on knowledge sharing among information technology majoring undergraduates.Comput Human Behav 2016;56:65-71.
33.Bagheri Hosseinabadi M,Etemadinezhad S,Khanjani N,et al. Evaluating the relationship between job stress and job satisfaction among female hospital nurses in Babol:An application of structural equation modeling.Health Promot Perspect 2018;8:102-8.
34.Dominguez LC,Silkens M,Sanabria A.The dutch residency educational climate test:construct and concurrent validation in Spanish language.Int J Med Educ 2019;10:138-48.
35.Steiger JH.Structural model evaluation and modification:an interval estimation approach.Multivariate Behavioral Research 1990;25:173-80.
36.Deng Q,Zheng Y,Lu J,Zeng Z,Liu W.What factors predict physicians’ utilization behavior of contrast-enhanced ultrasound?Evidence from the integration of the theory of planned behavior and technology acceptance model using a structural equation modeling approach.BMC Med Inform Decis Mak 2021;21:173.
37.Archambault P,Turcotte S,Smith PY,et al.Intention to use Wikibased knowledge tools:survey of quebec emergency health professionals.JMIR Med Inform 2021;9:e24649.
38.Guo S,Guo X,Zhang X,Vogel D.Doctor–patient relationship strength’s impact in an online healthcare community.Inform Technol Dev 2018;24:279-300.
39.Guo S,Guo X,Fang Y,Vogel D.How doctors gain social and economic returns in online health-care communities:a professional capital perspective.J Manag Inform Sys 2017;34:487-519.
40.Bamberg S,Möser G.Twenty years after Hines,Hungerford,and Tomera:a new Meta-analysis of psycho-social determinants of pro-environmental behaviour.J Environ Psychol 2007;27:14-25.
41.Fornara F,Pattitoni P,Mura M,Strazzera E.Predicting intention to improve household energy efficiency:the role of value-beliefnorm theory,normative and informational influence,and specific attitude.J Environ Psychol 2016;45:1-10.
42.Xia Y,Shi LS,Chang JH,Miao HZ,Wang D.Impact of the COVID-19 pandemic on intention to use Traditional Chinese Medicine:a cross-sectional study based on the theory of planned behavior.J Integr Med 2021;19:219-25.
 Journal of Traditional Chinese Medicine2022年4期
Journal of Traditional Chinese Medicine2022年4期
- Journal of Traditional Chinese Medicine的其它文章
- Editorial Board Listing
- Mixed methods research in complementary and alternative medicine:a scoping review
- Herbal anthelmintic agents:a narrative review
- Identification of novel biomarkers and therapeutic target candidates for stasis-heat symptom pattern of acute intracerebral hemorrhage by quantitative plasma proteomics
- Effect of three tongue needles acupoints Lianquan (CV23) and Hegu(LI4) combined with swallowing training on the quality of life of laryngeal cancer patients with dysphagia after surgery
- Effectiveness of auricular point acupressure with magnetic plate for pain management in acute postpartum cesarean section patients in Thammasat University Hospital:a randomized clinical controlled trial