
Effectiveness of auricular point acupressure with magnetic plate for pain management in acute postpartum cesarean section patients in Thammasat University Hospital:a randomized clinical controlled trial
2022-07-20 08:19:30RakchanokTanitsookarnKomsunSuwannarurkParadiSangvatanakulSupapenLertvuttivivatJunyaPattaraarchachaiKornkarnBhamarapravatana
Rakchanok Tanitsookarn,Komsun Suwannarurk,Paradi Sangvatanakul,Supapen Lertvuttivivat,Junya Pattaraarchachai,Kornkarn Bhamarapravatana
Rakchanok Tanitsookarn,Komsun Suwannarurk,Supapen Lertvuttivivat,Department of obstetrics and gynecology,Faculty of medicine,Thammasat University,Pathum Thani 12120,Thailand
Paradi Sangvatanakul,Junya Pattaraarchachai,Chulabhorn International College of Medicine,Thammasat University,Pathum Thani 12120,Thailand
Kornkarn Bhamarapravatana,Department of preclinical science,Faculty of medicine,Thammasat University,Pathum Thani 12120,Thailand
Abstract OBJECTIVE:To compare the effectiveness of auricular acupressure with or without magnetic plates to routine post cesarean pain management.METHODS:This randomized controlled trial was conducted at Obstetrics and Gynecology Department,Thammasat University Hospital,between January and June 2020.All participants were term primigravida pregnant women who underwent cesarean delivery during the study period.Participants were divided into three groups,namely control,placebo and study groups.Study (magnetic application) and placebo (non-magnetic application) groups received magnetic and non-magnetic auricular patches at both pinnas,respectively.Randomized assignments for each group were computergenerated,printed and kept in opaque sealed envelopes.The points in this study were Shenmen (TF4),Erzhong(HX1) and Penqiang (TF5).Visual analog scale (VAS)was immediately recorded up to 72 h after the operation.RESULTS:A total of 195 cases were enrolled during the period of study.Each group had 65 participants.The mean participant’s age was 31 years old.Demographic and clinical characters among the three groups were comparable.Pain scores within 12 h postoperative period of all three groups were comparable.Between 36 and 72 h post-operation,study groups had significantly lower VAS than the control group.One-quarter of participants had comparable nausea and vomiting side effects.CONCLUSIONS:Auricular acupressure at Shenmen(TF4),Penqiang (TF5) and Erzhong (HX1) with magnetic plate attachment could significantly relieve post cesarean pain between 18 and 72 h.
Keywords:cesarean section;pain;acupressure;magnetic plate
1.INTRODUCTION
In recent years,cesarean delivery rate in Thailand has risen higher than that of Southeast Asia regional average and exceeded the recommended rate of the World Health Organization.1Postoperative cesarean pain within 24 h was the most problematic among parturients who underwent surgery. Multimodal anesthesia for postoperative pain control had been recommended by the Enhanced Recovery After Surgery Society (ERAS) in 2017.2Analgesic agents used for post caesarean operative pain control should be selected to vary in their pain reduction mechanisms to best support new mothers.Opioids (most commonly meperidine) were the most common class of analgesic agents used for pain control in post cesarean parturients.However,nausea and vomiting were common opioid side effects.3The aim of postoperative pain management is an effective anesthesia control with minimal side effects.
Post cesarean delivery mothers who had minimal pain could return to normal activities,i.e.,nursing their offspring,as soon as possible.Complementary and alternative therapy (CATs) was recommended by the World Health Organization for reduction of opioid doses in parturients.4
Acupuncture and acupressure are methods from Traditional Chinese Medicine (TCM) which has been investigated for the use in pain reduction.5According to TCM,postoperative pain is generated by surgical trauma.Over blood flow and stagnation between skin causes stagnation ofQi,blood stasis and impassable arteries.5
Gate control theory and its biochemical mechanism were possible explanations for its efficacy.Gate control theory states that impulses from acupressure points are transmitted to the brainviathe meridian line at four times transmission rate of pain stimuli.6Fast and continuous acupressure impulse the transmission to the brain could block the low transmission of pain stimuli,leading to pain receptor blockage.Neuro-hormonal transmitters(cortisol,endorphin and serotonin) were reported to be released from acupoint stimulation.6
Stimulation at a specific pinna’s area could induce somatic reflexology.The concept of imbalancedYin-Yang(Qi) energy was believed to be the causative stimulus of pain or diseases.7Auricular stimulation of specific areas by acupressure could release opioid peptides,i.e.,endorphin,enkephalin and other neurotransmitters.8
Shenmen (TF4) is recognized as a pain relieving acupoint.It regulates the excitation and inhibition process of cerebral cortex and subcortical autonomic nerve center.Anti-inflammatory,analgesia and calming nerve are consequent of Shenmen (TF4) stimulation.Erzhong (HX1) is a hemorrhagic control acupoint for labor induction and postpartum pain.Penqiang (TF5) is used for various gynecological and obstetric disease via meridian conduction.5Much recent literature reported the effectiveness of auricular acupressure in post cesarean pain reduction.Zhonget al9stated that auricular acupressure in conjunction with botanical plant seed or magnetic plate usage could reduce postoperative pain in surgical,abdominal and orthopedic surgery.Auricular acupressure had also been used to reduce postoperative cesarean delivery pain as reported by several studies.8,10-12
The aim of this investigation was to compare the effectiveness of auricular acupressure (with and without magnetic plates) to standard post cesarean pain management.
2.METHODS
2.1.Participants
This randomized controlled trial was conducted at the Obstetrics and Gynecology department of Thammasat University Hospital between January and June 2020.Ethical approval was obtained prior to the study by the Ethics Committee on Clinical Research of the Faculty of Medicine,Thammasat University (MTU-EC-OB-1-170/62).The Thai clinical trial registration number was TCTR 20191221004.
All participants were term primigravida pregnant women who underwent cesarean delivery during the study period.The age of participants ranged between 18 and 45 years old.Exclusion criteria included cases with multiple pregnancy,coagulation abnormality,bleeding disorders,intraoperative complication,postoperative complication,repeated exploratory laparotomy within 24 h postoperatively,chronic skin disease,lesions at pinna or nonconsent to study participation.Demographic data included age,gestational age,underlying diseases,body mass index,occupation and education level.
2.2.Study design,assessments and treatment
Enrollment was taken during the last trimester antenatal visit.Consent form was signed to allow the patient's participation in the event that the patient had to undergo cesarean delivery.Once the cesarean delivery option was recommended by the attending obstetrician,the allocation method was randomized for the patient by computer generated numbers printed and kept in an opaque sealed envelope.Participants were divided into three groups:control,placebo and study.All groups were counseled regarding the operation detail and postsurgery pain management according to Thammasat university hospital standard protocols.
The standard protocol of anesthesia used in the present study was a neuraxial regional block.Bupivacaine (11 mg)in hyperbaric solution with 0.2 mg of morphine was the standard anesthetic agent in the current study.General anesthesia with endotracheal intubation was performed as a secondary option per the anesthesiologist’s judgement.Standard postoperative care was applied to participants in all three groups.
Study (magnetic application) and placebo (non-magnetic application) groups received magnetic and non-magnetic auricular patches at both pinnas,respectively.The auricular patch used in this study was a 10 mm diameter adhesive tape.Two mm diameter acupressure magnetic auricular plate FENG FAN®(Hengshui Fengfan Medical Device Trading Co.,Ltd.,Hengshui,China) were attached to the adhesive side of the auricular patch.Each pinna had patches attached at three sites.Both study and placebo groups received auricular patches at all three sites,namely Shenmen (TF4),Erzhong (HX1) and Penqiang (TF5),on both pinnas.Patch attachment was performed by a certified Doctor of Traditional Chinese Medicine or an OB&GYN resident who performed the procedure under the former’s supervision.
The concept of auricular acupressure was demonstrated and counseled to both the study and placebo groups in the same manner.Auricular acupressure was manipulated at the same site on both ears using the index finger and the thumb.The frequency of acupressure was once every second.Each point received 30 acupressure(for 1 or 2 min).5The second and the last point of both ears were manipulated in the same manner.Each set of acupressure points were repeatedly messaged every five minutes. Additional auricular acupressure was performed as needed if patients felt that the pain had not been relieved.Auricular acupressure was started 2 h after surgery (T0) and maintained for three consecutive days.Assessment of postoperative pain was performed at T0(checked in time at the ward 2 h post-surgery),then at 12,24,36,48,60 and 72 h intervals thereafter.Visual analog scale (VAS) (0=no pain,10=worst possible pain) was used for pain evaluation in all subjects.Non-opioid intravenous analgesia as prescribed in cases reporting pain was equal to or greater than 6 before T24.
After T24,additional analgesia (ibuprofen and acetaminophen) were prescribed only by patient request.Side effects of opioid administration,i.e.,nausea,vomiting,dizziness,itching,urticarial rash,anaphylaxis symptom,respiratory distress and apnea,were also recorded.
2.3.Statistical analysis
Sample size was calculated by an experienced statistician using the G-power program version 3.1.7 (UCLA,LA,USA).Effect size was set at the level of 0.25.Alpha and beta errors were set at the level of 0.05.Total sample size that met statistical significance was 65 cases per arm(total sample size was 195 cases).
Data collections were randomized from in-patient charts,classified into different groups based on a randomized order,then chosen into the study based on the acceptance response.Patients were not privy to their group assignment.
The identified methods and controlled variables included the type of skin incision (low midline,Pfannenstiel) and the choice of anesthetic.The selected patients were 195 primigravida following cesarean delivery,defined and sorted into three groups (65 cases per group),namely the control (standard treatment protocol),placebo and study group.The control group received standard medical treatment following cesarean delivery which included oral 500 mg acetaminophen or 400 mg ibuprofen.The placebo group received standard medical treatment and non-medical auricular patches while the study group received standard medical treatment and auricular patches with magnets.The patches were placed at the same sites (Shenmen,Erzhong,Penqiang) with each patient receiving a total of six auricular ear patches (three patches per each earlobe).
Pain evaluation was recorded as pain score in VAS from T0,12,18,24,36,48,60,and 72 h following ward admission after cesarean operation and delivery.Patient’s pain was also evaluated based on the frequency and quantity of any additional pain medication requested.Other operative and medical side effects,namely nausea,vomiting,abdominal pain,and respiratory depression were also recorded.
The statistical package for the social science,version 17.0 for Windows (SPSS Inc.Released 2008.SPSS Statistics for Windows,Version 17.0.Chicago,IL,USA)was used for the statistical analysis.Demographic and clinical characteristics between each group were analyzedviamean and standard deviation analysis.Category data was analyzed using percentage,95%confidence interval (CI) and χ2whenever clinically applicable.The mean was estimated by a generalized linear model for repeat measure analysis of variance and visualized as a bar chart for pain score evaluation after surgery.ThePvalue of less than 0.05 was set as the statistical significance in this study.
3.RESULTS
A total of 195 cases were enrolled and divided into three equal groups (65 cases per group).The mean average age of all participants was 31 years old without statistically significant difference among control (non-auricular patch),placebo (non-magnetic auricular patch) and study groups (magnetic auricular patch).Percentages of participants less than 35 years old were 84.6,81.5 and 80.0 in control,placebo and study group,respectively without statistical significance.
All participants delivered healthy and appropriate weight offspring for their gestational ages.Half of the study participants had government or office jobs.Other demographic characteristics of all three groups are shown in Table 1.
Ninety-three percent of participants underwent cesarean delivery under neuraxial spinal anesthesia.All participants were nulliparous.Physicians’ choice of midline or low transverse skin incision was comparable between all three groups with no statistical significance.Length of surgical wound,time under surgery,estimated blood loss and length of hospital stay were all comparable as presented in Table 2.
Participants in control,placebo and study groups had comparable immediate postoperative pain at T0 and T12(Table 3).
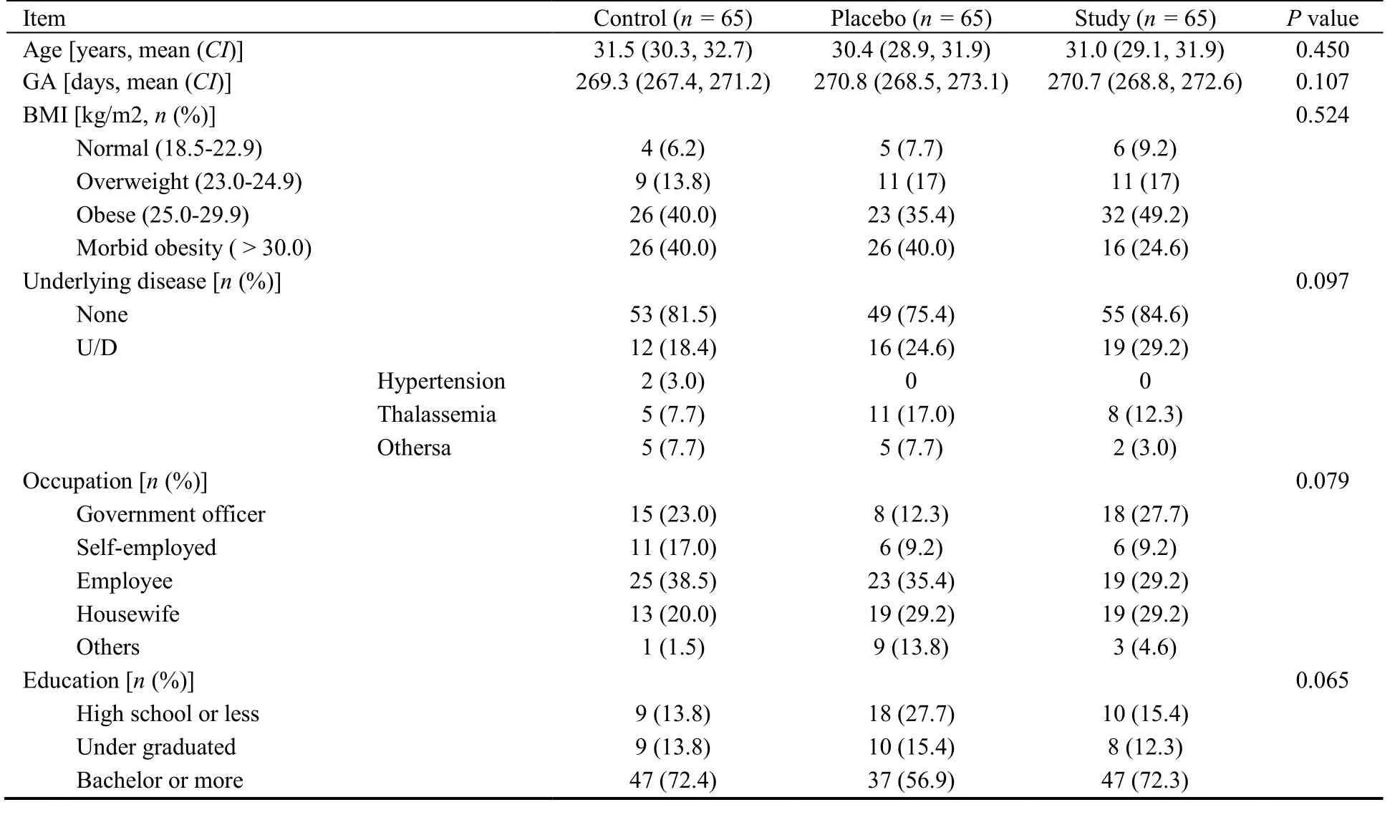
Table 1 Demographic character of participants
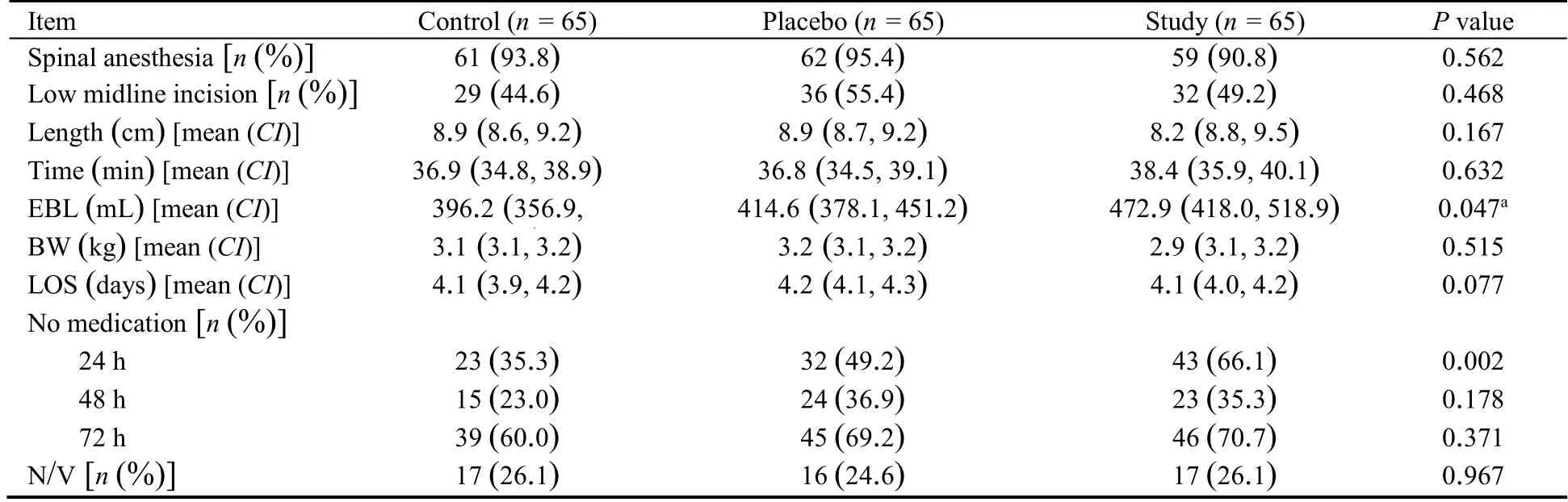
Table 2 Obstetrics history of participants
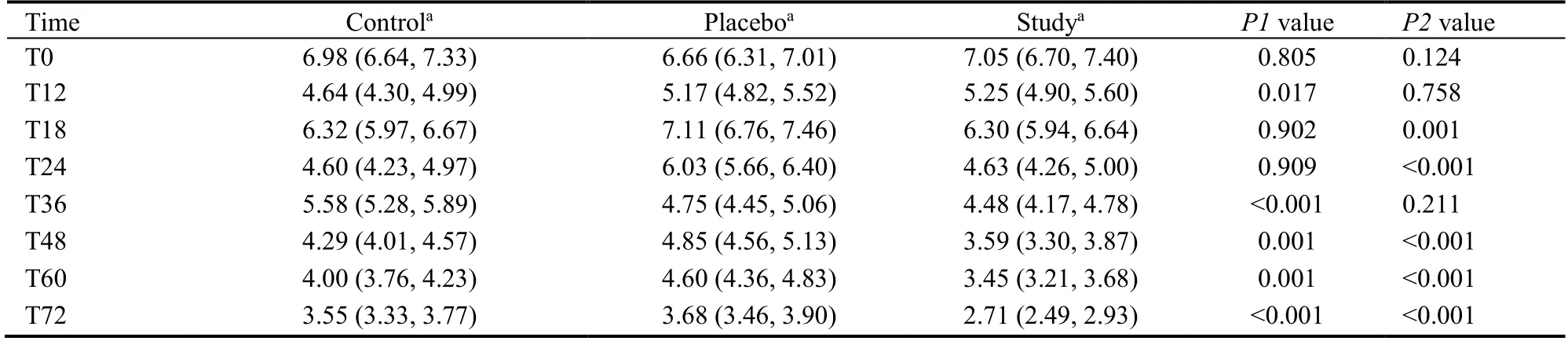
Table 3 Effect of pain score change by the mean scale of generalized linear model for repeat measure analysis of variance and visual expressed in table chart
VAS at T18 and T24 of control and study groups were statistically lower than that of the placebo group.Control and study groups had comparable postoperative pain levels during these periods (T18 and T24).At T36 placebo and study groups had significantly less postoperative pain than that the control group.T48 and T60 revealed VAS of the study group with significantly lower pain levels than the placebo and control groups.At T48 control and placebo groups had comparable VAS.At T72 showed both control and placebo groups with comparable pain scores,which were significantly higher than the study group.Nausea and vomiting among participants in control,placebo and study groups occurred at 26.1 (17/65),24.6 (16/65) and 26.1 (17/65)percent,respectively and without any statistical significance.There were no harmful or unwanted side effects from the use of magnetic plates or adhesive tape in the current study.
4.DISCUSSION
Nulliparous parturients were selected for this investigation,and they had no prior experience of delivery.This minimized any pain bias participants might bring to the investigation.The study of the use of needle acupuncture at arm,body and calf revealed effective pain relief in cesarean parturients.12-15Prolonged needle puncture at body site or extremities were invasive and caused maternal disturbance.16Noninvasive technique could possibly be an appropriate method for adjunctive pain relief in cesarean parturients.Since the pinna had no subcutaneous fat,neither percent fat deposit nor BMI should affect results from the auricular acupoint.17Each acupressure point in TCM had a different effect on the nervous system.18In the current study,pain from cesarean section was the patient’s main concern.Specific acupressure points for primary acupressure point and master acupressure point were carefully selected.Shenmen (TF4),Penqiang (TF5) and Erzhong (HX1)were chosen as acupressure points to investigate in this study.The VAS score results showed that magnetic
acupressure manipulation of these three points statistically lower perceived pain in the study group.This result supported the purported value of Chinese acupressure medicine.All three groups had comparable pain levels at 12 h of postoperative pain.This was explained by the remaining effect of neuraxial analgesia.19,20
At T18 and T24,study and control groups had equal pain levels.The placebo group had significantly higher pain levels than the study and control groups.Expectation of pain relief was found in placebo and study groups.Pain relief in the study group was significantly lower than in the placebo group.Cases in the placebo group believed in the efficacy of acupressure and may have benefited from a placebo effect.21The cases in the control group did not have any expectation of pain relief except pain relief from post operative treatment.Postoperative pain medication continued to have lingering effects into the first data collection periods.19At T18 and T24 auricular acupressure was shown to significantly relieve pain in the study group.Moreover patients at T18 and T24 in both placebo and study groups requested less pain medication while control group participants requested more analgesics as shown in Table 2.
T36 revealed comparable pain levels for both the placebo and study groups which were significantly lower than that of the control group.At T36,the effects of neuraxial anesthesia had completely subsided.19,20Placebo and study groups showed significantly more pain relief levels compared to the control group.Pain relief effects in the study group were comparable and increasingly greater than that reported in control and placebo groups at T48,T60 and T72,respectively.
In this investigation,massage at auricular point was shown to relieve minor and moderate postoperative pain.Auricular plate marked auricular acupoints and assisted participants in better ability to locate auricular acupoint Shenmen (TF4),Penqiang (TF5) and Erzhong (HX1) for self-massage compared to placebo group with the nonmagnetic plate.Auricular massage without a magnetic plate showed precise acupoint sites,allowing for somewhat effective pain relief.
The mechanism of pain relief effects from auricular acupressure remains unclear to western researchers.22The techniques of ancient Chinese medicine have been integrated into modern medicine.Acupoints in the Chinese language were classified in alphabetic order.Auriculotherapy in Chinese medicine had somewhat exaggerated effects on health according to western medical perception.However,three auricular acupoints selected by this investigation allowed postoperative cesarean surgical pain relief as expected from the TCM body of knowledge.The pain relief effect from auriculotherapy was explained by the stimulation of nerve fibers and the release of neurotransmitters.22Many western literatures reported pain relief effect by acupoint stimulation in minor and moderate pain,even though the exact mechanism of action was not fully understood.22Mafetoni’s and Nani’s studies demonstrated that body point acupressure could relieve postoperative cesarean pain.23,24Body acupuncture had also been reported to relieve post cesarean pain in two Chinese studies.12,13A combination of body and auricular acupuncture demonstrated efficacy of pain management in postoperative patients.14A similar study by Hesse and colleagues from Germany reported that the combination of body and auricular acupuncture decreased post cesarean pain.15Systematic reviews by Zhonget al9concluded that auricular acupressure with botanical plant seeds or magnetic pellets could significantly decrease hemorrhoid,abdominal,orthopedic and ENT pain up to 72 h after surgery.Acupoints in the present study were chosen with reference to Mafetoni’s study,which reported that auricular acupressure at the points of Shenmen,uterus,endocrine and neurasthenia area showed a significant effect on labor pain and labor duration.25Our results supported Mafetoni’s results in the obstetric field.The comparison of auricular treatment for pain was summarized in Table 3.
Strengths of this study:all participants were healthy pregnant women with high levels of education (bachelor or higher).Communication and detailed counseling were given to participants.Auricular acupressure did not interfere with early ambulation in post cesarean parturients.Auricular acupuncture was an invasive technique and prolonged application led to maternal disturbance in lactation and nursing.
Limitations of this study:cesarean delivery is one of the most potent pain responses in obstetric work.Auricular acupressure alone could not fully mitigate this potent pain.During the 24 h post-operative period,the remaining analgesic effects could interfere with the measurement of the effect of auricular acupressure pain.In conclusion,auricular acupressure at Shenmen (TF4),Penqiang (TF5) and Erzhong (HX1) is shown to relieve post cesarean pain after 24 h.After two and three days during post cesarean delivery,the addition of auriculotherapy was shown to contribute to additive pain relief.Magnetic plate attachment was shown to increase accuracy in auricular acupressure stimulation when compared with non-magnetic attachments.Auricular acupressure was convenient,low cost and non-invasive,and should be considered for post cesarean parturient in the future.
5.REFERENCES
1.Liabsuetrakul T,Sukmanee J,Thungthong J,Lumbiganon P.Trend of cesarean section rates and correlations with adverse maternal and neonatal outcomes:a secondary analysis of thai universal coverage scheme data.AJP Rep 2019;9:328-36.
2.Macones GA,Caughey AB,Wood SL,et al.Guidelines for postoperative care in cesarean delivery:Enhanced Recovery After Surgery (ERAS) Society recommendations (part 3).Am J Obstet Gynecol 2019;221:247.e1-9.
3.Landau R.Post-cesarean delivery pain.Management of the opioid-dependent patient before,during and after cesarean delivery.Int J Obstet Anesth 2019;39:105-16.
4.World Health Organization.Reproductive health and research.Care in normal birt:a practical guide.Report of a Technical Working Group.Geneva:WHO;1996;14.
5.Oleson T.Overview of auriculotherapy treatment procedures.In:Oleson T.Auriculotherapy Manual,4th ed.Los Angeles:Churchill Livingstone 2014;195-7,215-22.
6.Alimoradi Z,Kazemi F,Gorji M,Valiani M.Effects of ear and body acupressure on labor pain and duration of labor active phase:a randomized controlled trial.Complement Ther Med 2020;51:102413.
7.Makvandi S,Mirzaiinajmabadi K,Sadeghi R,Mahdavian M,Karimi L.Meta-analysis of the effect of acupressure on duration of labor and mode of delivery.Int J Gynaecol Obstet 2016;135:5-10.
8.Hou PW,Hsu HC,Lin YW,Tang NY,Cheng CY,Hsieh CL.The history,mechanism,and clinical application of auricular therapy in Traditional Chinese Medicine:Evid Based Complement Alternat Med 2015;205:495684.
9.Zhong Q,Wang D,Bai YM,Du SZ,Song YL,Zhu J.Effectiveness of auricular acupressure for acute postoperative pain after surgery:a systematic review and Meta-analysis.Chin J Integr Med 2019;3:225-32.
10.Yeh CH,Chiang YC,Hoffman SL,et al.Efficacy of auricular therapy for pain management:a systematic review and metaanalysis.Evid Based Complement Alternat Med 2014;934670.
11.You E,Kim D,Harris R,D'Alonzo K.Effects of auricular acupressure on pain management:a systematic review.Pain Manag Nurs 2019;1:17-24.
12.Yang GY,Chen QZ,Fu HY,Chen CH.Effect of auricular acupuncture on postpartum rehabilitation of primipara with cesarean.Zhong Guo Zhen Jiu 2019;39:717-20.
13.Wu HC,Liu YC,Ou KL,et al.Effects of acupuncture on postcesarean section pain.Chin Med J (Engl) 2009;122:1743-8.
14.Liu XL,Tan JY,Molassiotis A,Suen LK,Shi Y.Acupuncturepoint stimulation for postoperative pain control:a systematic review and Meta-analysis of randomized controlled trials.Evid Based Complement Alternat Med 2015;657809.
15.Hesse T,Henkel B,Zygmunt M,Mustea A,Usichenko TI.Acupuncture for pain control after Caesarean section:a prospective observational pilot study.Acupunct Med 2016;34:14-9.
16.Nielsen A,Gereau S,Tick H.Risks and safety of extended auricular therapy:a review of reviews and case reports of adverse events.Pain Med 2020;21:1276-93.
17.Langevin HM,Agache P.Subcutaneous tissue histophysiology.Agache’s Measuring the Skin 2017:661-8.
18.Oleson T.Auriculotherapy treatment protocols.In:Oleson T.Auriculotherapy Manual,4th ed.Los Angeles:Churchill Livingstone,2014:355-98.
19.Brull R,Macfarlane AJ,Chan VW.Spinal,epidural and caudal anesthesia.In:Gropper MA,editors.Miller's Anesthesia.9th ed.Philadelphia:Elsevier,2020:1425-7.
20.DeSousa KA,Chandran R.Intrathecal morphine for postoperative analgesia:current trends.World J Anesthesiol 2014;3:191-202.
21.Rankin L.Mind over medicine:scientific proof that you can heal yourself.California:Hay House,Inc.,2013:6-16.
22.Santoro A,Nori SL,Lorusso L,Secondulfo C,Monda M,Viggiano A.Auricular acupressure can modulate pain threshold.Evid Based Complement Alternat Med 2015;457390.
23.Mafetoni RR,Shimo AK.Effects of acupressure on progress of labor and cesarean section rate:randomized clinical trial.Rev Saude Publica 2015;49:9.
24.Nani D,Maryati S,Rahmaharyanti R.Effect of acupressure therapy point HT 6 and LI 4 on post cesarean sectio’s pain.Int J Res Med Sci 2015;3:119-22.
25.Mafetoni RR,Shimo A.Effects of auriculotherapy on labour pain:a randomized clinical trial.Rev Esc Enferm USP 2015;50: 726-7.
 Journal of Traditional Chinese Medicine2022年4期
Journal of Traditional Chinese Medicine2022年4期
- Journal of Traditional Chinese Medicine的其它文章
- Editorial Board Listing
- Mixed methods research in complementary and alternative medicine:a scoping review
- Herbal anthelmintic agents:a narrative review
- Factors influencing physician's behavioral intention to use Traditional Chinese Medicine to treat coronavirus disease 2019 based on the theory of planned behavior
- Identification of novel biomarkers and therapeutic target candidates for stasis-heat symptom pattern of acute intracerebral hemorrhage by quantitative plasma proteomics
- Effect of three tongue needles acupoints Lianquan (CV23) and Hegu(LI4) combined with swallowing training on the quality of life of laryngeal cancer patients with dysphagia after surgery