Effect of auricular plaster for primary hypertension in older people:A meta-analysis
2022-07-04 00:27:04YongQinYuLouXiaoYanShenYunGai
World Journal of Meta-Analysis 2022年2期
Yong Qin, Yu Lou, Xiao-Yan Shen, Yun Gai
Yong Qin, Yu Lou, Xiao-Yan Shen, Yun Gai, Department of Cardiology, The Seventh People's Hospital of Shanghai University of TCM, Shanghai 200137, China
Yun Gai, Department of General Medicine, The Seventh People's Hospital of Shanghai University of TCM, Shanghai 200137, China
Abstract BACKGROUND Hypertension is a critical public health problem globally. Antihypertensive drugs can create an extra burden on hypertension patients' self-regulation leading to an imbalance of blood supply and demand. This study aimed to evaluate the effect of auricular plaster therapy combined with western medicine to treat primary hypertension in older people.AIM To carry out a systematic review and meta-analysis for the effect of auricular plaster in elderly hypertension patients.METHODS Multiple databases like PubMed, EMBASE, Cochrane Library, Chinese Biomedical Literature on Disc, China National Knowledge Infrastructure, Wan Fang and Chinese Science and Technology Periodical Database were used to search for the relevant studies and full-text articles involved in the evaluation of auricular plaster combined with western medicine and western medicine alone for primary hypertension in older people. All included articles were quality assessed and the data analysis was conducted with the Review Manager (5.4). Forest plots, sensitivity analysis and funnel plots were also performed on the included articles.RESULTS In this analysis, fourteen (14) relevant studies were included. The Meta-analysis showed a significant difference in the effective ratio (OR = 3.62; 95%CI, 2.46 to 5.33; P < 0.00001), diastolic blood pressure change (5.68 mmHg; 95%CI, 3.49 to 7.87; P < 0.00001), systolic blood pressure change (MD = 8.78 mmHg; 95%CI, 5.04 to 12.53; P < 0.00001) and symptom score (MD = 3.20; 95%CI, 1.23 to 5.18; P = 0.001) between auricular plaster combined with western medicine group and western medicine alone group. One bias was detected as selection bias and another two in reporting bias. Sensitivity analysis fulfilled the stability of the results.CONCLUSION Our study suggested that auricular plaster combined with western medicine improved primary hypertension better than western medicine alone. Limited by the quality of included studies, further studies should be performed to confirm our findings.
Key Words: Primary hypertension; Older people; Auricular plaster; Meta-analysis
lNTRODUCTlON
Primary hypertension, referred to as hypertension, is a syndrome with elevated blood pressure as the main clinical manifestation[1,2]. It is an important cause and risk factor for a variety of cardiovascular and cerebrovascular diseases. It affects the structure and function of essential organs such as the heart, brain and kidney and eventually leads to the failure of these organs. It is still one of the leading causes of death in patients with cardiovascular diseases[3,4]. At present, the number of people with hypertension in the world has exceeded 1 billion and 90%-95% of these are diagnosed with primary hypertension[5,6]. Hypertension has become a significant public health problem endangering human health.
Long-term high blood pressure (BP) will cause compression on the systemic blood vessels, leading to vascular blockage or rupture, stroke, heart failure, aortic dissection and other complications[7-9]. Therefore, reasonable control of blood pressure is the key to treat hypertension and reduce its complications. Patients with hypertension must take prescription medicine for life. Applying antihypertensive drugs will increase the burden of patients' self-regulation leading to the imbalance of blood supply and demand and has certain limitations[10,11]. It is of great clinical significance to explore the non-drug therapy available for hypertension[12].
In recent years, a non-drug therapy called auricular plaster has been reported to treat essential hypertension in China and the number of reports is increasing[13-15]. Auricular plaster is a common diagnosis and treatment technology of traditional Chinese medicine, also known as auricular point pressing beans or auricular point pressing seeds, which refers to sticking hard and smooth drug seeds or pills, magnetic beads and other things on the surface of the auricular points and fixing them with adhesive tape[16-18]. The human body has six meridians distributed in and around the ear and the ear is connected with organs through meridians. The auricle is the only body surface area with vagus nerve distribution. Auricular plaster can activate the vagus nerve and regulate the autonomic nervous system by stimulating auricular points with cowherb seeds to reduce blood pressure ( BP)[19,20].
There are many clinical studies on auricular plaster therapy for elderly patients with primary hypertension, but the intervention methods and intervention time were quite different. Our study conducted a systematic review and meta-analysis of related randomized controlled trials (RCT) to evaluate the clinical efficacy of auricular plaster therapy combined with western medicine to treat primary hypertension in older people to provide a reference for clinical decision-making.
MATERlALS AND METHODS
Literature search strategy
We used comprehensive databases (PubMed, EMBASE, Cochrane Library, Chinese Biomedical Literature on Disc, China National Knowledge Infrastructure, Wan Fang and Chinese Science and Technology Periodical Database) to search for previous studies investigating the effects of auricular plaster therapy for primary hypertension in the elderly. The literature search was performed from inception up to July 2021 using the following keywords: (1) Auricular plaster; (2) Primary hypertension; and (3) Western medicine. Terms were searched as text words and these three themes were combined using the Boolean operator 'or' to complete our search strategy. Our literature search was comprehensive with neither language restrictions nor publication status limitations. Two of us identified and reviewed full-text articles deemed relevant by screening the list of titles and abstracts. Disagreements were resolved through consensus between the two reviewers.
Study selection
After the primary selection, the text of the potentially relevant studies was reviewed. The studies included must meet the following inclusion criteria: (1) Comparing research patients who receive combination therapy of auricular plaster and western medicine (test group) and standard western medicine alone (control group); (2) Patients with primary hypertension [systolic BP (SBP) ≥ 140 mmHg or diastolic BP (DBP) ≥ 90 mmHg]; (3) Containing indicators evaluating effectiveness between test group and control group; and (4) Available in full text.
Studies were excluded based on the following pre-determined exclusion criteria: (1) Not randomized controlled trials (RCT); (2) Reviews, letters, or protocols; (3) Duplicate articles; and (4) lack of related outcomes.
Data extraction and quality assessment
Two independent reviewers performed the study selection, data extraction and quality assessment. Prespecified data elements were extracted from each trial using a structured data abstraction form, including baseline characteristics, sample size and interventions used. The risk of bias of included RCTs was assessed using a modified version of the Cochrane Collaboration’s Risk-of-Bias Tool. Two coauthors independently performed the risk-of-bias assessment on all included RCTs. When in a disagreement, the rechecking of the original article was followed by discussion and was used to reach a consensus.
Statistical analysis
Meta-analysis was performed in Review Manager (RevMan) software (version 5.4; Cochrane Collaboration) using the inverse variance method. We assumed that the studies' variability beyond subjectlevel sampling error was random, and consequently, we adopted a random-effect model. The Mantel-Haenszel odds ratio (OR) model was used to summarize classification data, summary estimates and a 95%CI was reported for continuous variables as the mean difference (MD). Quantifying the inconsistency and heterogeneity across studies was assessed using Cochran Q andI2statistics. When the heterogeneity was present, the random-effects model was used to calculate the pooled OR or MD, whereas the fixed effects model was used in its absence. We also performed a sensitivity analysis with each endpoint to determine if there was any difference between groups. Publication bias was graphically analyzed with funnel plots. We also applied Egger and Begg’s statistical test. APvalue of < 0.05 was considered statistically significant.
RESULTS
Results of the literature search process
An electronic search was performed to identify all potential articles published in the English language by July 2021, and initially, 932 articles were selected. After a careful review of the titles and abstracts, 126 studies were included due to immediate satisfaction with the purpose of the present meta-analysis. Further, 112 articles were excluded due to not fulfilling the inclusion criteria. The remaining 14 studies were assessed and reviewed to satisfy the inclusion criteria and were considered in our meta-analysis[21-34]. Figure 1 represents an outline of the studies' identification, inclusion and exclusion criteria, thereby summarizing the search process and the reasons for exclusion.

Figure 1 Flow chart of literature search and study selection for systematic review and meta-analysis.
Study characteristics
A total of 1088 patients with primary hypertension were included in this meta-analysis study and all these studies were published from 2012 to 2021. The primary outcome contained effective ratio, DBP change, SBP change and symptom score.
The antihypertensive effect was determined according to the relevant standards in the guiding principles for clinical research of new drugs in traditional Chinese medicine[35]. (1) Strongly effective (meets one of the following conditions): Diastolic blood pressure (DBP) decreased by 10 mmHg or more, and within the normal range; DBP did not fall to the normal range but decreased by 20 mmHg or more; (2) Moderate effective (meet one of the following conditions): DBP decreased less than 10 mmHg, within the normal range; DBP decreased to 10-19 mmHg, but still higher than the normal range; Systolic blood pressure (SBP) decreased to 30 mmHg; and (3) Ineffective: Did not meet any of the above criteria. The effective ratio in our outcome variable was the sum of strongly effective and moderate effective ratios.
Symptom score referred to the curative effect standard in the guiding principles for clinical research of new Chinese medicine in 2002[36]. Headache, vertigo and insomnia were selected to observe the symptoms and the symptoms were scored according to the degree of symptoms from mild to severe. The primary study chosen characteristics are summarized in Table 1.
Results of the quality assessment
According to the Cochrane risk of the bias assessment tool, to assess the bias risk (including selection, performance, detection, attrition and reporting bias among the included randomized trials) (Figures 2 and 3), the methodological quality of included studies was evaluated for the bias risk. There was a high risk of selection bias in one study and reporting bias in two other studies. In the summary risk of bias assessment of the 14 included studies, there is a limited selection bias, performance bias and detection bias. In general, there are only two trials with bias risk and the other six tests have no risk.
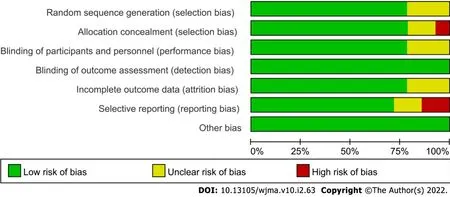
Figure 2 Proportion of studies with low (green), high (red), or unclear (yellow) risk of bias.

Figure 3 Graph of the risk of bias summary.
Results of heterogeneity test
The effect of auricular plaster on effective ratio was reported in 12 studies. A significant improvement in the effective ratio was identified compared with the control group (OR = 3.62; 95%CI, 2.46 to 5.33;P< 0.00001). There was no significant heterogeneity for effective ratio assessment (P= 0.74,I² = 0%) (Figure 4).

Figure 5 Meta-analysis on the effect of auricular plaster therapy on DBP change.
Thirteen trials reported information about DBP change. A random-effect model was used to evaluate the heterogeneity of DBP change due to the significant heterogeneity (P< 0.0001,I² = 89%). The pooled analysis showed that the test group had a better reduction of DBP than the control group (MD = 5.68 mmHg; 95%CI, 3.49 to 7.87;P< 0.00001) (Figure 5).
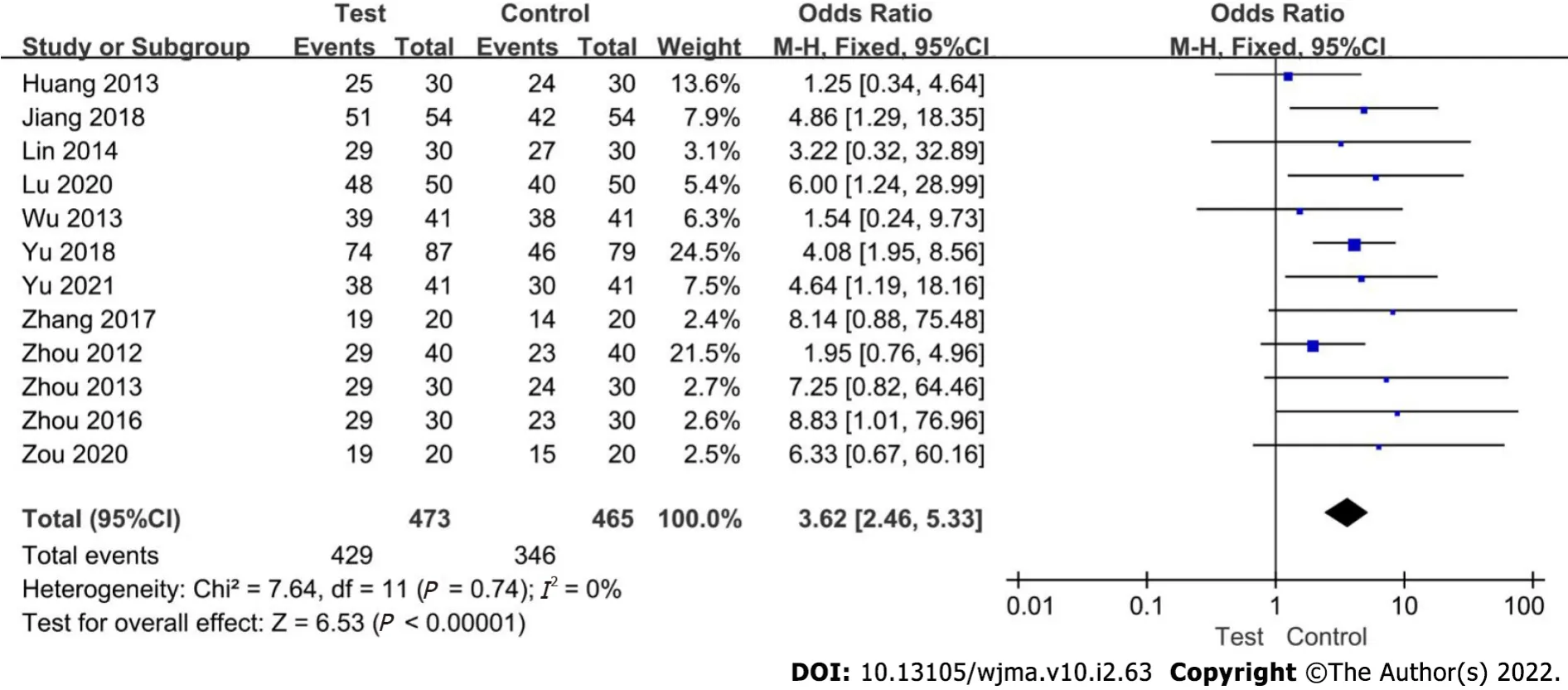
Figure 4 Meta-analysis on the effect of auricular plaster therapy on effective ratio.
In evaluating the difference of SBP change between the test group and control group, 13 articles involved 1028 patients. Meta-analysis showed that compared to the control group, the test group had a higher reduction of SBP (MD = 8.78 mmHg; 95%CI, 5.04 to 12.53;P< 0.00001), with significant heterogeneity (I² = 94%,P< 0.00001) (Figure 6).

Figure 6 Meta-analysis on the effect of auricular plaster therapy on SBP change.
Four studies reported symptom scores. A random-effect model was used to evaluate the heterogeneity among the significant heterogeneity included studies (P< 0.00001,I² = 89%). The results showed that the test group improved symptom scores better than the control group (MD = 3.20; 95%CI, 1.23 to 5.18;P= 0.001) (Figure 7).

Figure 7 Meta-analysis on the effect of auricular plaster therapy on symptom score.
Results of sensitivity analysis and publication bias
The included studies will be excluded one by one for sensitivity analysis. The heterogeneity of DBP change was decreased from 89% to 87% when Wu 2013 was excluded suggesting that the meta-analysis results were robust.
A funnel plot was performed to evaluate the publication bias for effective ratio qualitatively. The shape of the funnel plot showed some evidence of symmetry (Figure 8) and the Egger test was not significant (P= 0.77), which indicated no significant publication bias existed in this meta-analysis.

Figure 8 Funnel plot for potential publication bias.
DlSCUSSlON
Hypertension is one of the most common cardiovascular diseases. In recent years, with the change of modern living habits, the incidence rate of hypertension has been increasing year by year. Hypertension has presented a trend toward younger people. How to control BP safely and reliably has become a problem that medical workers must solve today[37]. How to effectively and stably control BP and avoid large fluctuations such as a sudden fast rise or lowering of blood pressure. Maintaining a steady BP reduces the damage caused by BP fluctuations, prevents the adverse effects caused by excessive BP, reduces the damage of essential organs and effectively controls the disability rate and mortality rate which is the key to the problem[1,38,39].
At present, western medicine is the primary treatment for hypertension and the first-line antihypertensive drugs include diuretics, β Receptor blockers, calcium antagonists, angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists[40,41]. The guidelines point out that diuretics can reduce blood volume and relax peripheral blood vessels; β Receptor blockers can reduce cardiac output; Calcium antagonists can inhibit calcium influx in vascular smooth muscle and reduce myocardial contractility; Angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists can block the renin-angiotensin system and dilate arterioles and venules. The mechanism of action of these drugs is to improve the circulatory system from different aspects to reduce BP[42,43].
In China, auricular plaster is a diagnosis and treatment technology developed based on auricular acupuncture therapy[44]. Cowherb Seeds are complicated and can activate blood circulation and regulate BP. Auricular plaster therapy can regulate BP to a certain extent, significantly improve patients' clinical symptoms with hypertension and improve patients' satisfaction with nursing work[45,46]. Some studies have shown that auricular plaster therapy can regulate the balance of viscera and meridians, promote the function of the cerebral cortex to return to normal quickly and comprehensively treat the uncoordinated nerve, body fluid and vascular function to achieve the effect of reducing BP[47,48].
Fourteen studies were included in this systematic review and meta-analysis. The meta-analysis results showed that the effective ratio of auricular plaster therapy in the treatment of hypertension based on conventional western medicine therapy was higher than that of western medicine alone therapy (OR = 3.62;P< 0.00001), suggesting that auricular plaster therapy had an excellent adjuvant effect on hypertension. The decrease of DBP (MD = 5.68 mmHg;P< 0.00001), SBP (MD = 8.78 mmHg;P< 0.00001) and symptom score (MD = 3.20;P= 0.001) were more evident than that of the control group, suggesting that the combination therapy of auricular plaster and western medicine was better than western medicine alone in improving clinical symptoms. It showed that auricular plaster therapy had significant health benefits in treating hypertension and was worthy of clinical promotion.
This study showed apparent heterogeneity in the assessment of the literature included in the improvement of SBP, DBP and symptom scores. Although sensitivity analysis showed that heterogeneity did not affect the final results, we still analyzed the source of heterogeneity. After further reading and analysis of the included studies, we found that the heterogeneity may be caused by different types of antihypertensive drugs, other antihypertensive mechanisms and different effects on SBP, DBP and clinical symptoms, which suggested that we need to conduct a subgroup analysis on different types of antihypertensive drugs.
There were some limitations in this meta-analysis. Firstly, auricular plaster therapy was a unique traditional medical method in China and the published reports were mainly in Chinese with the quality being relatively poor. Secondly, some of the included studies did not describe the implementation of random allocation and blind methods. In addition, the frequency of auricular plaster, the type and dose of western medicine was also different in the experiment which suggested that more detailed hierarchical or subgroup analysis can be done in the future.
CONCLUSlON
In conclusion, auricular plaster combined with western medicine can improve the antihypertensive effect of primary hypertension, reduce BP and improve clinical symptoms. In view of the quality of the included studies, the reliability of the conclusions was reduced. It is still necessary to carry out multicenter, large sample randomized controlled trials, paying attention to the implementation of the randomized method, allocation concealment method and blind method to obtain reliable research data so as to provide the evidence-based basis for clinical treatment of hypertension.
ARTlCLE HlGHLlGHTS
Research background
Hypertension is a very common health problem for older people. Recently, a non-drug therapy called auricular plaster has been used to treat hypertension in China and is considered traditional Chinese medicine. There were many clinical studies which reported on auricular plaster therapy for elderly patients with hypertension but the intervention methods and intervention times were quite different.
Research motivation
We speculate about gaining a detailed insight into the effect of auricular plaster therapy on elderly patients with primary hypertension.
Research objectives
This study aimed to evaluate the effect of auricular plaster therapy combined with western medicine to treat primary hypertension in older people.
Research methods
A literature search was carried out to identify reports published through July 1, 2021. The meta-analysis was carried out for the outcomes of the significant difference in the effective ratio, diastolic blood pressure (DBP) change, systolic blood pressure (SBP) change, and symptom score between auricular plaster combined with western medicine group and western medicine alone group. Publication bias was identified by the funnel plots test.
Research results
In this analysis, fourteen (14) relevant studies were included. The Meta-analysis showed a significant difference in the clinical effective ratio (OR = 3.62; 95%CI, 2.46 to 5.33; P < 0.00001), DBP change (5.68 mmHg; 95%CI, 3.49 to 7.87; P < 0.00001), SBP change (MD = 8.78 mmHg; 95%CI, 5.04 to 12.53; P < 0.00001) and symptom score (MD = 3.20; 95%CI, 1.23 to 5.18; P = 0.001) between auricular plaster combined with western medicine group and western medicine alone group.
Research conclusions
Auricular plaster could be a potential therapy to treat hypertension in elderly patients.
Research perspectives
More prospective sample studies are needed in the future to enhance the speculation of our conclusion.
FOOTNOTES
Author contributions:Qin Y, Lou Y, and Gai Y participated in the conception and design of the study, library searches and assembling relevant literature, critical review of the paper, supervising the writing of the paper and database management; Qin Y, Shen XY, and Gai Y participated in data collection, library searches assembling relevant literature, writing the paper and critical review.
Supported byLeading talent training of Pudong New Area Health Committee, No. PWR12020-02; Exploration on the discipline construction mode of treating and preventing diseases based on specific diseases, No. PWZY-2019-0402; Shanghai collaborative innovation center of traditional Chinese medicine health services.
Conflict-of-interest statement:All authors declare that they have no conflict of interest.
PRlSMA 2009 Checklist statement:This study was conducted as per PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Yong Qin 0000-0001-9972-281X; Yu Lou 0000-0002-1885-2397; Xiao-Yan Shen 0000-0002-0605-9922; Yun Gai 0000-0002-8718-2315.
S-Editor:Liu JH
L-Editor:Filipodia
P-Editor:Liu JH