
Long-term outcome of pathologic myopic foveoschisis treated with posterior scleral reinforcement followed by vitrectomy
2022-06-22 03:12:34YaoHuangYueQiWenBinWeiAnLiDuan
INTRODUCTION
In our previous study, we found that FD had a significant impact on postoperative visual prognosis
. Therefore, we divided the patients into FD and non-FD groups. There were24 eyes without FD and 20 eyes with FD according to the preoperative OCT images. The preoperative BCVA of non-FD eyes were 0.96±0.50 logMAR, and were 1.34±0.73 logMAR in FD eyes (
=0.048). The postoperative BCVA in the non-FD group was 0.17±0.15, which was better than the BCVA in the FD group (0.45±0.42 logMAR;
=0.011). The preoperative CFT was 492.54±81.90 μm in the non-FD group and 751.95±240.08 μm in the FD group; the difference between these 2 groups was statistically significant (
<0.001). At the last visit, there was no significant difference in CFT between the FS and FD groups (190.71±55.26 and 161.95±52.67 μm,
=0.086). There was no significant difference between these two groups in age, sex, preoperative/postoperativine axial length, or preoperative refractive error (Table 3).
SUBJECTS AND METHODS
Baseline Characteristics Forty-four eyes of 27 patients were included in this study. The demographics and clinical data of the patients are presented in Table 1. The mean age was 53.3±12.6y (range 35-78y). The mean preoperative BCVA,refractive error, axial length and foveal thickness are shown in Table 1. The mean preoperative foveal thickness was 610.45±217.11 μm. The mean preoperative axial length was 29.60±1.71 mm and the mean preoperative refractive error in phakic eyes was -16.26±4.71 D. The follow-up period was 47.98±18.23mo (range 24-83mo).
All patients underwent a routine ophthalmologic examination preoperatively and at every follow-up visit postoperatively. The following data were collected: age,sex, optical coherence tomography (OCT) findings, BCVA(Snellen chart), refractive error, axial length, postoperative complications and follow-up time. BCVA was measured using a Snellen chart. Refractive error was measured with streak retinoscopy (Heine Optotechnik GmbH & Co. KG, Herrsching,Germany). Axial length was measured with IOL Master (Carl Zeiss Meditec). If cataract was obvious, axial length was measured with A-scan and color doppler flow imaging (Esaote mylab twice, Italy). Spectral-domain OCT (Cirrus high-defifinition OCT; Carl Zeiss Meditec, or Heidelberg Engineering, or Optovue) centred through the fovea was performed before and after surgery to observe the macular microstructures and measure the central foveal thickness. A cross-scan for Stratus OCT and a 5-line raster scan for Cirrus OCT were performed.The Snellen BCVA was converted into the logarithm of the minimal angle of resolution (logMAR) for statistical analysis.
The mean postoperative refractive error at the last visit(-4.70±5.34 D) was obviously lower than the preoperative value (-16.26±4.17 D;
<0.001). Such a significant difference is mainly because most patients underwent cataract surgeries combined with IOL implantation. Except for those who underwent cataract surgeries, the mean postoperative refractive error of the remaining patients was -14.53±3.13, which was not significantly different from the preoperative refractive error(
=0.356; Table 2).
The inclusion criteria were axial length no less than 26.0 mm; refractive error of the phakic eye ≤-6 D; with foveoschisis; completed more than two years of follow-up. The exclusion criteria were foveoschisis with MH (lamellar or fullthickness); and history of vitrectomy or PSR.
金际珍拿出儿子小时候戴的帽子和小围嘴,上面绣了花、草还有小精灵的图案,看起来相当精美,帽子上的布有几块已经脱线了,绣的图案却依然很牢固。
无论采用哪种轴系对中方法,都必须达到质量要求。在系泊试验和航行试验时,通过测量和分析轴系运转时的热态参数来评估轴系校中质量。测量记录见表3和表4。
The OCT images were analysed and measured in a masked fashion by two separate authors(Huang Y and Qi Y). Any discrepancies were resolved from detailed discussion with the principal investigator (Duan AL). Central foveal thickness was defined as the vertical distance from the inner surface of the sensory retina to the retinal pigment epithelium (RPE) at the highest foveal point of MF. After determining the internal and external points, the thickness was manually measured on the horizontal OCT scan using the OCT software.
All patients got PSR firstly. The surgical procedure of PSR was as described in our previous study
.A scleral buckle of donor sclera with a width of 6 to 10 mm was placed to the scleral surface of the macula. The superior end of the sclera buckle was sutured to the sclera surface to the nasal side of sclera surface near the insertion of superior rectus muscle, and the inferior end of the scleral buckle was sutured to the nasal side of sclera surface near the insertion of inferior rectus muscle. The location and scleral indentation were checked after placing the scleral buckle. It is necessary to make sure that the buckle did not compress the optic nerve.
治疗前,两组的APTT、PT、TT等指标不存在统计学差异性(P>0.05)。经过治疗,两组的三项指标均有所增加,观察组和之前以及治疗后的对照组相比不存在统计学差异性(P>0.05)。患者的BNP、CK-MB、LDH、ALT、AST、BUN、Cr指标均有所下降,和治疗前存在统计学差异性(P<0.05)。患者治疗前平均血细胞比容是(0.49±0.09),治疗后为(0.41±0.07),(P<0.05)。对照组的治疗显效率是20%,有效率是90%,观察组的显效率是65%,有效率100%,结果存在统计学差异性(P<0.05)。两组患者接受治疗的过程中没有发生并发症和不良反应。
One day and one week after operation, visual acuity, intraocular pressure (IOP) and ocular examination were recorded. Postoperative follow-up examinations, measurements of OCT, foveal thickness, BCVA, refractive error, and axial length were routinely performed. All patients completed more than 24 months’ follow-up. All Short-term and long-term postoperative complications were recorded.
Statistical analysis was performed using SPSS for Windows (version 19.0; IBM-SPSS, Chicago,IL, USA). The results are expressed as the means±standard deviation (SD). A paired
-test was used to compare the preoperative and postoperative BCVA, axial length, refractive error, and foveal thickness. The independent samples
-test was used to analyse the above parameters between patients with or without preoperative FD. The sex of patients with or without preoperative FD was analysed using the corrected Chi-square test. Differences were considered significant at
<0.05.
RESULTS
This study was approved by the Medical Ethics Committee of the Beijing Tongren Hospital. This study was a retrospective interventional case series. Patients with pathologic MF who underwent PSR followed by vitrectomy at Beijing Tongren Eye Center from 2012 to 2018 were included in this study. We obtained informed consents from all patients before surgery.
Anatomical Outcomes After PSR followed by vitrectomy,the postoperative foveal thickness was significantly reduced compared with the preoperative thickness (
<0.001,177.64±55.40 μm, 610.45±217.11 μm, respectively; Table 2).At the last follow-up visit, complete resolution of the MF was achieved in 42 eyes (95.45%). The remained two eyes (4.55%)got partial resolution. OCT imaging showed the macula had obvious foveoschisis and FD before surgery (Figure 1A). After surgery, the allogeneic scleral strip was just below the macular fovea area. The allogeneic scleral strip had a good reinforcing effect on the macular area (Figure 1B).
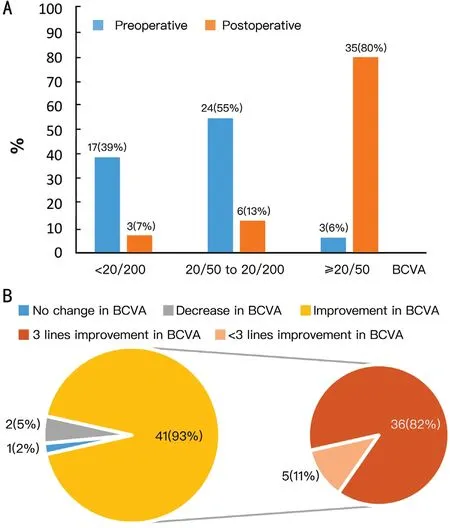
Best-Corrected Visual Acuity and Refractive Error The mean preoperative BCVA was 1.13±0.63 logMAR. The mean postoperative BCVA at the last visit was 0.30±0.33 logMAR,which was significantly improved compared with the preoperative BCVA (
<0.001; Table 2). Before surgery, the Snellen BCVA was <20/200 in 17 eyes (39%), 20/50 to 20/200 in 24 eyes (55%) and ≥20/50 in 3 eyes (6%). While the Snellen BCVA was <20/200 in 3 eyes (7%), 20/50 to 20/200 in 6 eyes (13%) and ≥20/50 in 35 eyes (80%; Figure 2A). At the last visit, the Snellen BCVA was improved in 41 eyes (93%),no change in 1 eye (2%), and decreased in 2 eyes (5%).Among the improved eyes, 36 eyes (82%) showed a 3-line improvement in BCVA (Figure 2B). Among the two decreased eyes, both had pathologic myopic choroidal neovascularization(CNV) that were treated with intravitreal ranibizumab and had scar formation.
以Zn2+螯合能力为考查指标,通过单因素试验,确定了碱性蛋白酶酶解玉米醇溶蛋白的最佳条件为反应体系pH值12,底物质量浓度10 mg/mL,酶添加量2×105U/mg,酶解时间180 min,酶解温度50℃,玉米醇溶蛋白与Zn2+螯合能力最佳,达到9.36 mg/g。在最适反应条件下酶解获得的玉米醇溶蛋白锌离子螯合肽,其DPPH自由基、羟自由基、ABTS+·的清除能力较未反应的玉米醇溶蛋白的有显著提高,表现出较好的抗氧化能力,为玉米醇溶蛋白的进一步加工提供参考。
Myopic foveoschisis (MF) can lead to significant decline in visual acuity in patients with pathologic myopia.The incidence of MF was about 9% to 34% in eyes with pathologic myopia
. MF is characterized by splitting of the layers of the neurosensory retina in macular region. Actually,MF is a slowly progressive condition. Most patients retain relatively good vision. However, a small number of cases(30%) will develop into more serious complications, such as foveal detachment (FD), vitreomacular traction (VMT),full-thickness macular hole (MH), and macular hole retinal detachment (MHRD). Once these above serious complications occur, visual acuity decreases significantly
. In these cases,surgical intervention is often necessary to prevent anatomical and functional deterioration. At present, the surgical strategies we adopt for MF are posterior scleral reinforcement (PSR)and vitrectomy
. PSR can reduce the foveal thickness and stabilize the axial length. However, PSR was not enough for MF accompanied by a premacular structure. In this condition,vitrectomy is a relatively more suitable surgical strategy,which can remove the posterior vitreous cortex and abnormal vitreomacular traction. On the other hand, for significant axial elongated eyes, especially combined with posterior scleral staphyloma, vitrectomy alone is not enough to for foveoschisis relief and macular reattachment
. In our previous study, we compared the surgical outcome of PSR followed by vitrectomy and vitrectomy alone on MF of extremely pathologic myopic eyes. The results showed that PSR followed by vitrectomy had a better best-corrected visual acuity (BCVA) improvement
.In our clinical experience, we usually use PSR followed by vitrectomy to treat MF, especially in markedly axially elongated eyes. To date, only one article has studied the oneyear follow-up results after PSR followed by vitrectomy for MF
, and there are no data on long-term follow-up after PSR combined with vitrectomy for MF. Moreover, their surgical technique of PSR is different from ours, and our surgical technique is relatively easier to master and implement
. We hope to explore whether PSR followed by vitrectomy can improve BCVA, relief foveoschisis, and stable axial length in the long-term. Therefore, in this study, we evaluated our longterm results of PSR followed by vitrectomy for MF, including functional and anatomic outcomes, to determine whether this surgical procedure can obtain a good prognosis in a long run.




The preoperative mean axial length was 29.60±1.71 mm. After PSR followed by vitrectomy, the postoperative mean axial length was 29.74±1.81 mm at the last visit. There was no significant difference between the preoperative and postoperative axial lengths (
=0.562; Table 2).Through PSR surgery, there was no significant increase in axial length within 47.98±18.23mo of follow-up.
The IOP of the two eyes (4.55%) after surgery were 25 mm Hg. One appeared at 1wk postoperatively, and the other appeared at the 1-year postoperatively. After treatment of cataprolol hydrochloride eye drops for 3-5d, both IOPs returned to normal (16-17 mm Hg). Myopic CNV developed at approximately 2y postoperatively in two eyes (4.55%)and was treated by intravitreal injection of ranibizumab.Two eyes (4.55%) developed cataracts approximately 1-2y postoperatively and underwent phacoemulsification and IOL implantation. No serious postoperative complications,including MH, peripheral retinal breaks, or retinal detachment,developed during the whole follow-up period.
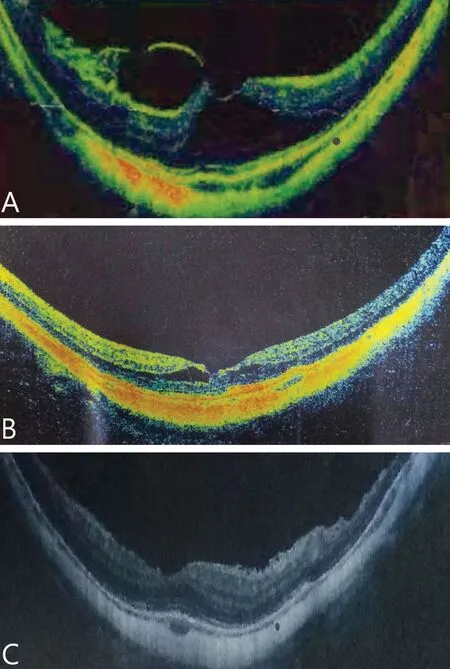
Case 1: A 47-year-old woman with MF in her left eye received PSR in December 2013. One week after PSR, this patients got vitrectomy with phacoemulsification and IOL implantation. During the surgery, we did not peel the ILM. Because there was VMT in the macular area without obvious epiretinal membrane, we only did complete PVD without ILM peeling and used C
F
as tamponade. Before surgery, the MF was obvious in her left eye (Figure 3A). The preoperative BCVA was 20/50 and the refractive error was-22.0 D. The preoperative central foveal thickness was 550 μm.The preoperative axial length was 31.5 mm. One month after surgery, the BCVA improved to 20/30 and the refractive error was -3.75 D. The MF got partial resolution (Figure 3B). The MF got complete resolution 3mo postoperatively and the central foveal thickness decreased to 264 μm (Figure 3C). The BCVA was improved to 20/25 and the refractive error was -2.0 D one year after surgery and continued to 5y postoperatively. The preoperative axial length at the last visit was 31.5 mm.
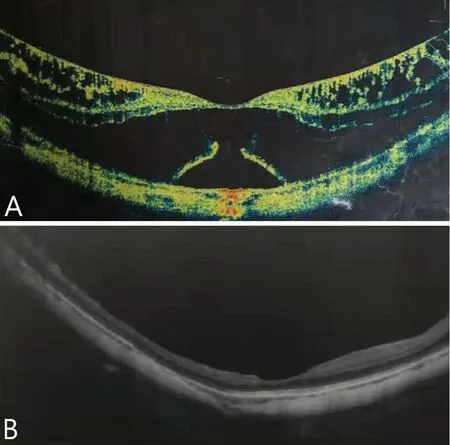
Case 2: A 38-year old man with MF and FD in his left eye(Figure 4A). PSR with vitrectomy was performed on his left eye on September 2014. The preoperative BCVA was 20/200 and the refractive error was -15.0 D. The preoperative central foveal thickness was 675 μm. The preoperative axial length was 28.72 mm. One month after surgery, the BCVA improved to 20/30 and the MF got complete resolution and maintained until the last visit more than 5y postoperatively (Figure 4B).The refractive error was -15.5 D, the central foveal thickness was 140 μm and the axial length was 29.34 mm at the last visit.
DISCUSSION
In our current study, we performed PSR followed by vitrectomy to treat patients with MF, who were followed for a long term. The follow-up period was 47.98±18.23mo (range 24-83mo). Our long-term outcomes showed that PSR followed by vitrectomy can effectively restore the anatomical structure of macula and improve the BCVA of MF patients. It was reported that vitrectomy alone could improve BCVA in 80%-84% of MF eyes
, and PSR alone could improve BCVA in 66%-75%of MF eyes at the end of follow-up
. While in our current study, up to 41 eyes (93%) achieved significant improvement in BCVA at the last follow-up visit. In our study, after PSR followed by vitrectomy, OCT showed that 95.45% of MF eyes achieved complete resolution of the MF, and the remaining 4.55% of MF eyes achieved partial resolution. While only 61.0%-80.0% of eyes achieved total resolution of foveoschisis after PPV alone
, and only 83.33% of eyes achieved complete resolution of foveoschisis after PSR alone
. Our current study showed that PSR followed by vitrectomy got better BCVA improvement and MF resolution than that of PSR or vitrectomy alone. PSR followed by vitrectomy can achieve the goal of internal and external combination. PSR can relieve posterior scleral staphyloma from the outside and stabilize the axial length. Vitrectomy can release the vitreoretinal traction from the inside, and the surface tension of gas tamponade can produce an additional pressure on foveoschisis, so as to further promote the resolution of foveoschisis and improve the BCVA. In our previous study, we also found that PSR followed by vitrectomy in extreme cases (axial length ≥30 mm)of MF had a greater improvement in BCVA than those treated with vitrectomy alone
. In our study, no full-thickness MH or recurrence of foveoschisis occurred during the follow-up period,while these two postoperative complications were reported as previously reported
. That’s why we chosen the surgical scheme of PSR followed by vitrectomy. This surgical scheme can not only remove the internal vitreo-retinal traction due to vitreofoveal adhesions but also release the antero-posterior stretching effect due to posterior staphyloma. Why didn’t we choose to do PSR and vitreomy simultaneously? At first, we did PSR and vitrectomy at the same time, but the postoperative reaction was relatively heavy. Therefore, we improved to do PSR first and vitrectomy later.
As for whether ILM should be removed during vitrectomy,it is still controversial. During vitrectomy, we only removed the posterior hyaloid membrane completely without peeling ILM. No full-thickness MH or MHRD occurred in our study.As previously reported
, the prevalence ranged from 7.5%to 21.4% in ILM peeling cases. Therefore, for pure MF eyes without obvious epimacular membrane, we do not think it is necessary to peel the ILM during vitrectomy. Without peeling ILM may reduce the risk of intraoperative and postoperative complications and shortening operation time.
One week after PSR, a conventional 23-gauge or 25-gauge 3-port vitrectomy was performed by a single experienced surgeon (Duan AL). Phacoemulsification with posterior chamber intraocular lens (IOL) implantation was performed simultaneously on eyes with cataracts. After vitrectomizing the core vitreous, triamcinolone acetonide (0.1-0.2 mL in a concentration of 40 mg/mL) was injected into the vitreous cavity to visualize the vitreous. The posterior hyaloid membrane was completely removed from the macular surface to get complete posterior vitreous detachment (PVD). The inner limiting membrane (ILM) was not peeled. Fluid-gas exchange was performed with tamponade of 16% perfluoroethane (C
F
), 12%perfluoroethane (C
F
), or air according to surgeon’s decision.After surgery, the patients were asked to stay in a facedown position for at least 1wk depending the type of tamponade.
During the natural course of extensive high myopia, the axial length elongated 2.05±0.91 mm, and the refractive error increased 3.02±1.57 D after 4-5y of follow-up
. Previous studies confirmed that PSR had a positive effect on visual acuity, refractive error, macular appearance, and axial length in pathologic myopic eyes
. In MF eyes, vitrectomy alone can only remove the internal vitreoretinal traction, while it cannot control the elongation of the axial length. Therefore,it may not be sufficient to improve the fovea anatomical situation, especially in markedly axially elongated eyes with posterior scleral staphyloma. In Zhang
’s study
.through vitrectomy alone, 40% of eyes had persistent residual foveoschisis after long-term follow-up. In our current study,we performed PSR associated with vitrectomy. A total of 95.45% of eyes achieved complete resolution of MF, and no full-thickness MH or recurrence of foveoschisis occurred during the whole follow-up period. The preoperative axial length was 29.60±1.71 mm, while the postoperative axial length was 29.74±1.81 mm after the long-term follow-up period (47.98±18.23mo). Axial length remained stable for a long time after PSR association with vitrectomy in our study. When patients with obvious preoperative cataract,A-ultrasound was used to measure the axial length. At this time, if the patient had FD, the measured value of axial length would be shorter than the actual one. In our study, there were 20 eyes (45.45%) with FD. Therefore, the preoperative actual axial length should be longer than 29.60±1.71 mm. It showed that our surgical scheme can shorten the axial length to a certain extent. This may explain why in our study, PSR with vitrectomy had a better outcome than vitrectomy alone
. Li
have reported the outcome of PSR with vitrectomy on MF patients. However, the operation procedure of Li
’s
PSR is different from ours. Our operation method is much simpler, lower risk of optic nerve injury and relatively much safer. Meanwhile, they had only one-year follow-up data and had no long-term follow-up results.
稻瘟病又称稻热病。是危害水稻最严重的病害之一,是一种真菌病害,属世界性水稻病害,在70多个国家发生此病。我国凡有水稻栽培的地区均有不同程度的发生,减产幅度一般为10%-15%,发病严重地块甚至颗粒不收。因此,稻瘟病已成为水稻高产、稳产的一大障碍。现将防治要点介绍如下。
根据得到的机构设计方案,结合实际使用需求对液压助力马桶装置进行实体设计以及三维图与装配图的绘制,如图7所示.
In our study, the postoperative complications included 2 cases of mildly elevated intraocular pressure, 2 cases of cataracts and 2 cases of myopic CNV. No serious complications occurred in our study. The cataracts were surgically managed with phacoemulsification and IOL implantation and got satisfactory results. Two eye (4.55%) developed CNV during the follow up period. In the natural course of pathological myopia, CNV will occur in about 10% of patients
, which is higher than the incidence of CNV in our study. Therefore, we believe that the occurrence of CNV is not related to surgery, but related to pathological myopia itself. A total of 4.55% of eyes developed mild glaucoma postoperatively. In a previous study,the rate of secondary glaucoma was 15% after PPV with silicone oil tamponade
. Our rate was much lower than that previously reported, and it was satisfactorily controlled by one antiglaucoma medication. In the current study, we only used air or gas as tamponade while not silicone oil, which led to a lower incidence of secondary glaucoma.
Vitrectomy with gas tamponade for MF has been performed with variable high success rates (75%-100%). Gas tamponade exhibited good outcomes on BCVA improvement or anatomical resolution
, possibly by inducing retinal repositioning by pushing back the retina. Gas has a larger surface tension and fewer complications than silicone oil; thus, we preferred gas or air for MF, which achieved good surgical results in this study:95.45% of MF eyes achieved complete resolution of MF. Air or gas is an ideal tamponade for vitrectomy in patients with MF.
In our current study, FD was associated with poor preoperative(
=0.048) and postoperative (
=0.011) BCVA. However, the postoperative BCVA significantly improved regardless of the presence of FD (
<0.001). Therefore, it seems that vitrectomy can improve visual acuity in eyes with or without FD, and the final BCVA was significantly correlated with the preoperative BCVA in both types of patients.
The main limitation of this study is that it is a retrospective study and without a control group. Further prospective studies are needed to study the long term effects of the surgical methods for MF patients in the future.In conclusion, for pathologic MF, PSR followed by vitrectomy is an effective procedure to improve the visual acuity and the anatomical structure of macula. It can also stabilize the axial ength for a long time.
稀疏解混方法假设高光谱图像中所有的端元已包含在端元光谱库中,作为一种半监督形式的混合像元分解方法[8],目的在于从这个已知的端元光谱库中寻找高光谱遥感图像像元最稀疏的线性端元光谱组合,即在端元光谱库中寻找最优的端元子集来表示每个混合像元。对应于传统的线性解混模型,稀疏解混的基本模型表示所示:
含电子器件的电路板越来越多地应用在信息化的国防设备中,在国防应用中电路板往往需承受更极端的工作条件,如精确制导炮弹中的电路板在发射过程中承受巨大冲击载荷,这些工况对电路板系统的结构可靠性提出了更高要求。此外,由于国防装备可能会经历长达20年的储存期,如何抵御环境中的潮湿和化学腐蚀也是结构设计中需考虑的问题。
: Supported by Central Health Bureau Project(No.2020YB49).
None;
None;
None;
None.
1 Duan TQ, Tan W, Yang J, Li FL, Xiong SQ, Wang XG, Xu HZ.Morphological characteristics predict postoperative outcomes after vitrectomy in myopic traction maculopathy patients.
2020;51(10):574-582.
2 Meng B, Zhao L, Yin Y, Li HY, Wang XL, Yang XF, You R, Wang JL, Zhang YJ, Wang H, Du R, Wang NL, Zhan SY, Wang YL.Internal limiting membrane peeling and gas tamponade for myopic foveoschisis: a systematic review and meta-analysis.
2017;17(1):166.
3 Wang LF, Wang YH, Li YL, Yan ZY, Li YH, Lu L, Lu TX, Wang X,Zhang SJ, Shang YX. Comparison of effectiveness between complete internal limiting membrane peeling and internal limiting membrane peeling with preservation of the central fovea in combination with 25G vitrectomy for the treatment of high myopic foveoschisis.
2019;98(9):e14710.
4 Iwasaki M, Miyamoto H, Okushiba U, Imaizumi H. Fovea-sparing internal limiting membrane peeling versus complete internal limiting membrane peeling for myopic traction maculopathy.
2020;64(1):13-21.
5 Lee DH, Moon I, Kang HG, Choi EY, Kim SS, Byeon SH, Koh HJ, Lee SC, Kim M. Surgical outcome and prognostic factors influencing visual acuity in myopic foveoschisis patients.
(
) 2019;33(10):1642-1648.
6 Liu BQ, Chen SD, Li YH, Lian P, Zhao XJ, Yu XL, Li T, Jin CJ, Liang XL, Huang SS, Lu L. Comparison of macular buckling and vitrectomy for the treatment of macular schisis and associated macular detachment in high myopia: a randomized clinical trial.
2020;98(3):e266-e272.
7 Dolar-Szczasny J, Święch-Zubilewicz A, Mackiewicz J. A review of current myopic foveoschisis management strategies.
2019;34(3):146-156.
8 Uchida A, Shinoda H, Koto T, Mochimaru H, Nagai N, Tsubota K,Ozawa Y. Vitrectomy for myopic foveoschisis with internal limiting membrane peeling and no gas tamponade.
2014;34(3):455-460.
9 Frisina R, Gius I, Palmieri M, Finzi A, Tozzi L, Parolini B. Myopic traction maculopathy: diagnostic and management strategies.
2020;14:3699-3708.
10 Lee CL, Wu WC, Chen KJ, Chiu LY, Wu KY, Chang YC. Modified internal limiting membrane peeling technique (maculorrhexis) for myopic foveoschisis surgery.
2017;95(2):e128-e131.
11 Azuma K, Hirasawa K, Araki F, Shiraya T, Yashiro S, Kato S,Nagahara M, Ueta T. Fovea-sparing as opposed to total peeling of internal limiting membrane for myopic foveoschisis: a systematic review and meta-analysis.
2021;5(7):670-679.
12 Lin JP, Yang CM. Combined fovea-sparing internal limiting membrane peeling with internal limiting membrane flap technique for progressive myopic traction maculopathy.
2022;260(2):489-496.
13 Germano RAS, Zacharias LC, Takahashi WY. Recurrent myopic foveoschisis: resolution after internal limiting membrane removal.
2015;78(1):44-46.
14 Qi Y, Duan AL, You QS, Jonas JB, Wang NL. Posterior scleral reinforcement and vitrectomy for myopic foveoschisis in extreme myopia.
2015;35(2):351-357.
15 Li XJ, Yang XP, Li QM, Wang YY, Wang J, Lyu XB, Jia H. Posterior scleral reinforcement combined with vitrectomy for myopic foveoschisis.
2016;9(2):258-261.
16 Huang Y, Huang WL, Ng DSC, Duan AL. Risk factors for development of macular hole retinal detachment after pars plana vitrectomy for pathologic myopic foveoschisis.
2017;37(6):1049-1054.
17 Zhang T, Zhu Y, Jiang CH, Xu GZ. Long-term follow-up of vitrectomy in patients with pathologic myopic foveoschisis.
2017;10(2):277-284.
18 Zhu ZC, Ji XY, Zhang JS, Ke GJ. Posterior scleral reinforcement in the treatment of macular retinoschisis in highly myopic patients.
2009;37(7):660-663.
19 Chen CH, Lin PY, Wu PC. Treatment effect of posterior scleral reinforcement on controlling myopia progression: a systematic review and meta-analysis.
2020;15(5):e0233564.
20 Gui JM, Ai L, Huang T. Vitrectomy with or without internal limiting membrane peeling for myopic foveoschisis.
2020;20(1):83.
21 Qi Y, Yan PY, Fan WY, Wang NL, Duan AL. Comparison of foveasparing and non-internal limiting membrane peeling for retinoschisis with foveal detachment in highly myopic eyes.
(
)2021;35(5):1467-1472.
22 Tian T, Jin H, Zhang Q, Zhang X, Zhang H, Zhao P. Long-term surgical outcomes of multiple parfoveolar curvilinear internal limiting membrane peeling for myopic foveoschisis.
2018;32(11):1783-1789.
23 Chen MJ, Dai JH, Chu RY, Qian YF. The efficacy and safety of modified Snyder-Thompson posterior scleral reinforcement in extensive high myopia of Chinese children.
2013;251(11):2633-2638.
24 Kato Y, Inoue M, Hirakata A. Effect of foveal vitreous cortex removal to prevent epiretinal membrane after vitrectomy for rhegmatogenous retinal detachment.
2021;5(5):420-428.
25 Dong XR, Liu J, Bu J. The efficacy of modified posterior scleral reinforcement with round scleral patches in Chinese children with high myopia.
2020;258(7):1543-1547.
26 Huang WL, Duan AL, Qi Y. Posterior scleral reinforcement to prevent progression of high myopia.
(
)2019;8(5):366-370.
27 Peng C, Xu J, Ding XY, Lu YY, Zhang J, Wang F, Yu JM, Wang HN,Zhang JS. Effects of posterior scleral reinforcement in pathological myopia: a 3-year follow-up study.
2019;257(3):607-617.
28 Ruiz-Medrano J, Montero JA, Flores-Moreno I, Arias L, García-Layana A, Ruiz-Moreno JM. Myopic maculopathy: current status and proposal for a new classification and grading system (ATN).
2019;69:80-115.
29 Bhatia D, Mehta A, DaCosta J, Crothers O, Talks JS. Real-world anti-vascular endothelial growth factor therapy outcomes in myopic choroidal neovascularization.
2021;15: 2753-2758.
30 Ghoraba HH, Leila M, Shebl M, Abdelhafez MA, Abdelfattah HM.Long-term outcome after silicone oil removal in eyes with myopic retinal detachment associated with macular hole.
2021;15:1003-1011.
31 Yun LN, Xing YQ. Long-term outcome of highly myopic foveoschisis treated by vitrectomy with or without gas tamponade.
2017;10(9):1392-1395.
32 Kim KS, Lee SB, Lee WK. Vitrectomy and internal limiting membrane peeling with and without gas tamponade for myopic foveoschisis.
2012;153(2):320-326.e1.
猜你喜欢
食品工业科技(2023年4期)2023-02-14 10:12:58
自然资源遥感(2022年3期)2022-09-20 08:04:22
科普童话·学霸日记(2022年1期)2022-05-30 10:48:04
科普童话·学霸日记(2022年1期)2022-05-30 10:48:04
中国食品学报(2019年10期)2019-11-12 11:31:36
安徽农业科学(2019年14期)2019-08-27 04:31:47
物流技术与应用(2017年3期)2017-05-17 05:29:04
西华师范大学学报(自然科学版)(2016年4期)2017-01-09 08:16:57
无线电工程(2016年11期)2016-02-07 02:25:06
中国洗涤用品工业(2015年2期)2015-02-28 19:02:00
 International Journal of Ophthalmology2022年6期
International Journal of Ophthalmology2022年6期
- International Journal of Ophthalmology的其它文章
- Intraocular lens removal or not during vitrectomy for acute infectious endophthalmitis after cataract surgery
- Vitreous function and intervention of it with vitrectomy and other modalities
- Short-term outcomes of mitomycin C-augmented excisional bleb revision with capsulectomy for failed Ahmed glaucoma valve
- Evaluation of nintedanib as a new postoperative antiscarring agent in experimental extraocular muscle surgery
- Multimodal imaging of experimental choroidal neovascularization
- A novel Nance-Horan syndrome mutation identified by next-generation sequencing in a Chinese family