
Placental pathologies and fetal outcome in pregnant women with COVID-19: A retrospective study
2022-06-11 08:33:58SoheilaSarmadiAraOmranipourElhamMirzaianRoghayyehAhangariZahraYazdiAzadehAsgarianMonirehMirzaie
Soheila Sarmadi, Ara Omranipour, Elham Mirzaian, Roghayyeh Ahangari, Zahra Yazdi, Azadeh Asgarian,Monireh Mirzaie✉
1Department of Pathology, Yas Hospital, Tehran University of Medical Sciences, Tehran, Iran
2Department of Obstetrics and Gynecology, School of Medicine, Shahid Beheshti Hospital, Qom University of Medical Sciences, Qom, Iran
3Department of Pathology, Shariati Hospital, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
4Department of Obstetrics and Gynecology, Clinical Research Development Unit, School of Medicine, Nekouei-Hedayati-Forghani Hospital, Qom University of Medical Sciences, Qom, Iran
5Department of Nursing, Clinical Research Development Unit, Nekouei-Hedayati-Forghani Hospital, Qom University of Medical Sciences, Qom, Iran
ABSTRACT
Objective: To describe histopathologic findings in the placentas in women with coronavirus disease 2019 (COVID-19) during pregnancy.
Methods: In a cross-sectional study, 38 pregnant women with COVID-19 and undergoing delivery between March 2020 and January 2022, were included. The patients had positive polymerase chain reaction (PCR) test for SARS-CoV-2 infection and the placentas after delivery were sent for histopathologic evaluation based on the Amsterdam Placental Workshop Group Consensus Statement and assessed by two pathologists.
Results: Our results showed that maternal vascular malperfusion was the most common and was present in 17 cases (44.7%).These features included accelerated villous maturation (36.8%)distal villous hypoplasia (5.3%), placental infarction (5.3%) and intervillous fibrin deposition (10.5%). Other pathologic findings included focal calcification (10.5%), intravillous congestion and hemorrhage (10.5%), sub-chorionic hemorrhage (5.3%), acute villitis, chronic histiocytic intervillositis and delayed villous maturation each in one case (2.6%). Twelve out of 38 cases showed no significant pathologic changes. Fetal outcomes included neonatal intensive care unit admission rate of 13.2%, dyspnea 31.6%,newborn’s anosmia 7.9%, intrauterine fetal demise 2.6%, asphyxia 2.6% and neonate COVID infection 5.3%.
Conclusions: Microvasculopathy, as a sign of maternal vascular malperfusion, is a common finding in placentas from SARS-CoV-2 positive pregnant women in the present study. Further studies with larger sample sizes and comparative studies between COVID-19 positive and negative, as well as information from patient follow-up are suggested.
KEYWORDS: Pregnant women; Placental; Pregnancy;Pathology; Mother; Maternal arteries sitefusion; COVID-19
Significance
Coronavirus infections during pregnancy were associated with severe maternal infection, and increased risk of maternal death in mothers as well as spontaneous abortion, fetal infection,fetal growth restriction, fetal loss, and congenital malformation in fetus and neonate. In the present study, maternal vascular malperfusion and accelerated villous maturation are the most common pathology findings in SARS-COV2 positive pregnant women. Microvasculopathy, as a sign of maternal vascular malperfusion, is a common finding in placentas of pregnant women with COVID-19.
1. Introduction
Coronavirus disease 2019 (COVID-19) is an acute respiratory disease caused by the virus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) belonging to the coronavirus family[1].Due to its rapid spread, it was soon declared a global pandemic by the World Health Organization in March 2020[2]. The impact of SARS-CoV-2 and the associated COVID-19 on pregnant women and infants is of particular interest to obstetricians, pediatricians,and patients[3]. The SARS-CoV-2 not only affects the respiratory system but also promotes histopathological changes and impacts on numerous non-respiratory organs, such as the heart, liver, kidney,brain, or male reproductive system[4,5].
The impact of SARS-CoV-2 infection on pregnancy outcome and its effects on the fetus and placenta is not well understood[6].Various viral infections in pregnancy may be associated with specific histopathological findings in the placenta. For example, cytomegalovirus infection in the mother manifests as lymphoplasmacytic villitis and enlargement of villi in the placenta[7].Little is currently known about the histopathological findings of placenta in SARS-CoV-2 infection and existing findings are nonspecific and variable[8].
The placenta is a highly specialized organ, which provides communication between the mother and fetus during pregnancy.It defends the balance between biochemical and immunological elements that are necessary for fetal development, and it is also a regulator for the protection of the fetus from various infections[7,9].A variety of viral infections in pregnancy are associated with specific placental findings, including lymphoplasmacytic villitis with associated enlargement of villi and intervillous hemosiderin deposition in the setting of maternal cytomegalovirus infection[8]as well as rare reports of intervillositis in the setting of Zika virus[10,11] and Dengue virus[12] among others. Several case series demonstrated that SARS infection during pregnancy was associated with severe maternal infection, increased risk of maternal death, and spontaneous abortion[13-16]. Additionally, some data available have also revealed fetal infection, fetal growth restriction, fetal loss, and congenital malformation that indicated the effects of the virus on the placenta[9].
In some studies, no significant changes have been reported; in some there is evidence of maternal and fetal vascular malperfusion,or both, and inflammatory lesions have been reported[10].Histopathologic examination of placental tissue can contribute significant information regarding the health of both mother and fetus[8]. In this study, we assessed the histopathological characteristics of placental specimens from thirty-eight pregnant women with COVID-19.
2. Materials and methods
2.1. Study setting and patients
This cross-sectional study was conducted in 38 pregnant women with COVID-19 referred to Forqani Hospital for delivery from March 2020 to January 2022. All patients had undergone polymerase chain reaction (PCR) tests for SARS-CoV-2 which were positive. All the patients were informed about the study purpose and signed the written informed consent form to participate in the study.
2.2. Maternal pathology and fetal outcome examinations
Clinical and demographic information of patients was extracted from medical documents and pathological and fetal outcome examinations were conducted.
2.2.1. Pathologic examination
After delivery, the placentas of all studied patients were sent to pathologic laboratory. To reduce infectivity, fixation of samples was done in 10% buffered formalin for 48 h[3]. After macroscopic examination, routine representative sections were submitted for histopathologic evaluation based on the Amsterdam Placental Workshop Group Consensus Statement (APWGCS)[2]. Pathologic findings based on the current APWGCS were evaluated by two pathologists.
2.2.2. Fetal outcome examination
For fetal outcome examinations, sections from membranes and umbilical cord including three full-thickness sections of the placental disc, one adjacent to the insertion site of umbilical cord and two sections from central portion of the placenta were prepared.All slides were stained by hematoxylin and eosin. Moreover,the newborn weight, Apgar at first and fifth minutes, newborn presentation, dyspnea, newborn’s anosmia, newborn gender,neonatal intensive care unit (NICU) admission, intrauterine fetal demise, asphyxia, and COVID infection were checked and assessed.
2.3. Statistical analysis
After data collection from the medical records and pathology library, the information entered to SPSS version 20 (SPSS Inc.,Chicago, IL, USA). Data were analyzed by descriptive statistics.Frequency and percent were used to describe the qualitative variables. Mean±standard deviation (mean±SD) and median(interquartile range) were used to describe the quantitate variables.Charts and graphs were depicted by Excel 2016.
2.4. Ethics statement
This study was approved by the Ethical Committee of Qom University of Medical Sciences, with study protocol IR.MUQ.REC.1398.154 cod at 2020.03.10 and IR.MUQ.REC.1399.007 cod at 2020.03.17.
3. Results
3.1. Demographic and hemodynamic data of mothers
The mean age of mothers was (30.1±6.5) years and varied from 17 to 41 years old. The gestational age was (35.7±3.2) weeks and ranged from 27 to 41 weeks. The mean of respiratory rate (breathes per minute), pulse rate (beats per minute), and SpO2was 23.4±5.0,103.1±23.6 and (94.5±5.0)%, respectively (Table 1). The nationality of 33 (86.8%) patients was Iranian and based on our results, 13(34.2%) of patients had a background disease and the prevalence of gestational diabetes mellitus, premature rupture of membrane and preeclampsia as pregnancy complications was 13.2%, 10.5% and 10.5%, respectively. The most common history of hypothyroidism in pregnant women was reported. The mother death happened in one mother (2.6%).
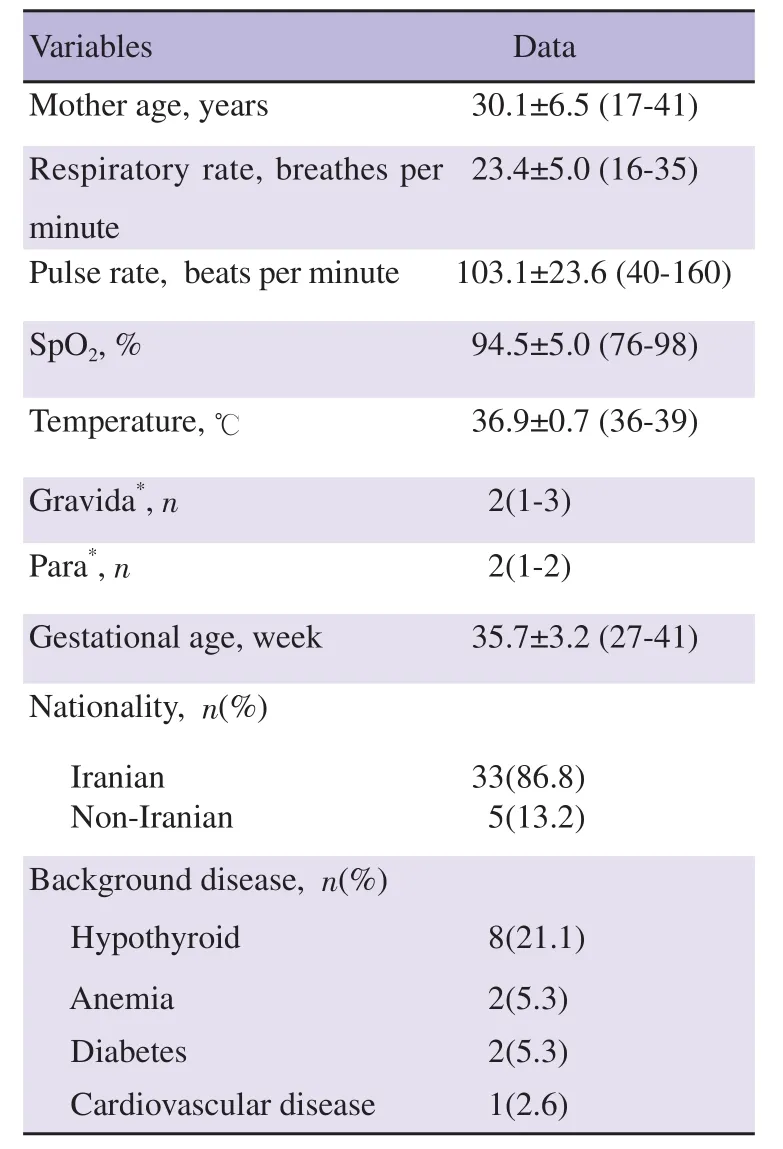
Table 1. Demographic and baseline characteristics of pregnant women with COVID-19.
3.2. Laboratory data of mothers
The laboratory results of pregnant women with COVID-19 are presented in Table 2 and showed that the mean of white blood cells and erythrocyte sedimentation rate was (10.68±4.19) ×103/μL and(68.80±25.34) mm/h, respectively.
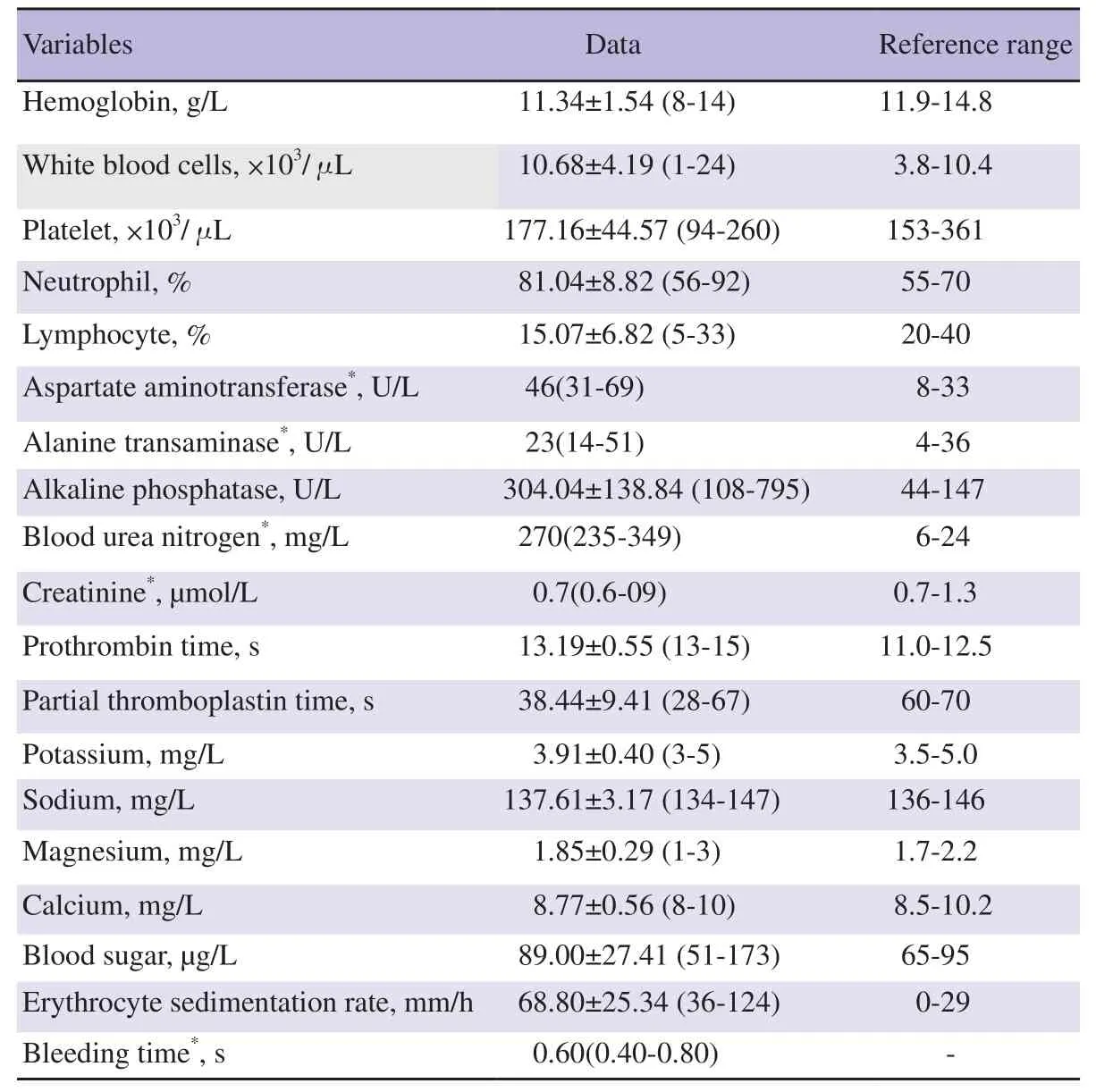
Table 2. Laboratory results of pregnant women with COVID-19.
3.3. Newborn data
From Table 3, the newborn weight, and newborn Apgar at 1 min was (2 900.7±579.9) g, and 8.9±0.3, respectively. Thirty-six cases(94.74%) had single baby and NICU admission occurred in 5 (13.2%)of newborns. The incidence of intrauterine fetal demise, asphyxia,COVID-19 infection in newborns was 1 (2.6%), 1 (2.6%) and 2(5.3%), respectively.
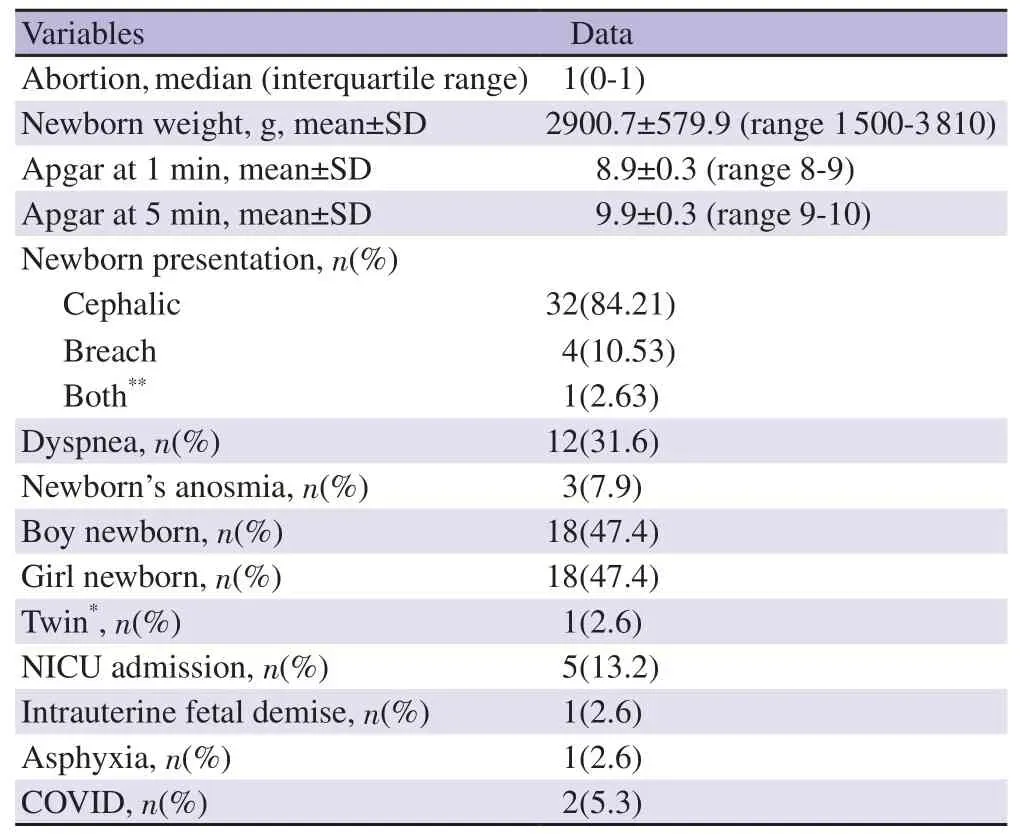
Table 3. Fetal clinical outcomes and complications from mothers with COVID-19 infection.
3.4. Clinical and pathological data
Our results showed that the most common symptoms in pregnant women with COVID-19 were cough in 19 cases (50.0%), fever 11 cases (28.9%), vomiting 6 cases (15.8%), myalgia 6 cases (15.8%)and weakness in 5 cases (13.2%), respectively (Supplementary Figure 1).
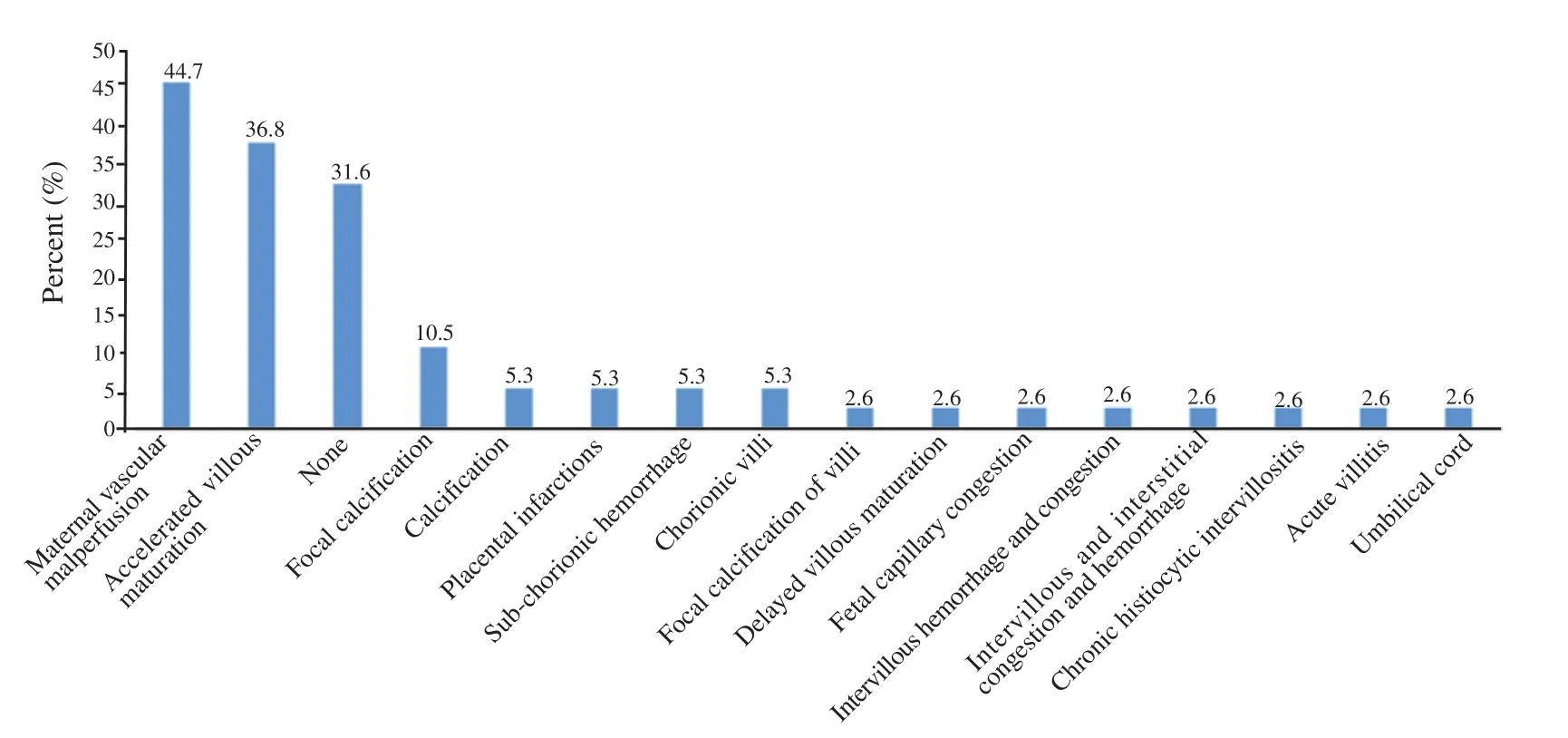
Figure 1. Pathologic findings of placenta in mothers with COVID-19 infection.
The pathologic findings showed no significant pathologic changes were observed in 12 patients (31.6%). Features of maternal vascular malperfusion were the most common pathology finding and were present in 17 cases (44.7%). These features included accelerated villous maturation in 14 cases (36.8%), distal villous hypoplasia in 2 cases (5.3%), placental infarction in 2 cases (5.3%) and intervillous fibrin deposition in 4 cases (10.5%). Other pathologic findings such as focal calcification (4/38), intravillous congestion and hemorrhage(4/38), sub-chorionic hemorrhage (2/38), acute villitis (1/38), chronic histiocytic intervillositis (1/38) and delayed villous maturation (1/38)were observed (Figure 1 and Supplementary Table 1).
4. Discussion
Coronavirus is a family of viruses known to cause a wide range of respiratory symptoms[17]. Nevertheless, there is sparse data available regarding coronavirus's effect on the placenta, maternal, and fetal outcomes[18]. Moreover, some studies have suggested that SARS infection was associated with increased micro-calcifications in viral positive mothers' placentas[19,20] and some reported histopathological findings compatible with edema and fibrin thrombi in the pulmonary vasculature[18,21].
In the current study, data of confirmed COVID-19 pregnant mothers including placental pathology and fetal outcomes were extracted after pathological and fetal examination. This study did not show significant pathologic changes observed in 31.6% (12/38) of patients,but revealed that maternal arteries sitefusion and accelerated villous maturation are the most common pathology findings of placenta in women with COVID-19. Focal calcification was diagnosed in 10.5% of cases, while calcification, placental infarctions, sub-chorionic hemorrhage and chorionic villi were observed in 5.3% of cases. A systematic review by Sharps et al examined the histopathological findings of placentas in mother with SARS-CoV-2 infection at third trimester. They found evidence of maternal vascular malperfusion in 46.0% of mothers and fetal vascular malperfusion in 35.3% of cases. In addition, evidence of inflammation including villitis 8.7%,intervillositis 5.3%, chorioamnionitis 6.0% in the placentas was observed[22]. Another study with very small sample by Menter et al including five placentas of confirmed SARS-CoV-2 women with term deliveries showed that maternal and fetal malperfusion were detected in 100% and 40% of patients, respectively. One placenta from symptomatic SARS-CoV-2-positive patient showed prominent lymphohistiocytic villitis and intervillositis[23]. Gao et al showed that the features of maternal vascular malperfusion observed in all eight studied placentas and focal increase of perivillous fibrin deposition were detected in seven cases[24].
Based on our results, all of the mothers recovered well and were discharged home asymptomatic, except one death and two newborns affected to COVID-19 after delivery that might be as a vertical transmission of SARS-CoV-2, but no clinical or serological evidence pointed to it. The study of Baergen et al showed that fetal vascular malperfusion or fetal vascular thrombosis was the most common lesion in 20 studied placentas. Meconium macrophages,maternal vascular malperfusion, acute chorioamnionitis, funisitis and chronic villitis were other miscellaneous findings. Therefore,COVID-19 might be associated to the tendency for thrombosis in the fetal circulation[25]. Moreover, a comparative study of Shanes et al in COVID-19 patients and control samples showed an increased prevalence of decidual arteriopathy and maternal vascular malperfusion due to abnormal or injured maternal vessels and intervillous thrombi through the placentas[18].
In a comparative study by Singh et al[26], placental pathology results showed that histologic features of malperfusion including micro-calcification, fibrin thrombi, syncytial knotting and villous agglutination were significantly higher in SARS-CoV-2 positive groups than negative ones[26]. This is maybe due to increased coagulation induced by SARS-CoV-2 or due to extreme syncytiotrophoblast injury. Nevertheless, Zhang et al’s study on 74 placentas that tested placental tissues for SARS-CoV-2 viral particles using in situ hybridization technique did not report any histopathological changes among placentas. But, viral particles within the syncytiotrophoblasts, atrophic endometrial glandular epithelium,and subchronic plate were showed. Therefore, they concluded no relationship between the maternal COVID-19 status and placental pathology[27]. The functional units of the placenta are chorionic villi and include syncytiotrophoblasts, cytotrophoblasts and extravillous trophoblasts between chorionic villi. Syncytiotrophoblasts locate in the external layer within the chorionic villi. In maternal infections,the syncytiotrophoblasts provide as a barrier against invasion.Extravillous trophoblasts locate in the base of the stem villi and unlike the syncytiotrophoblasts, they cause vertical transmission because extravillous trophoblasts define a direction through which pathogens can break the placental barrier. Additionally,cytotrophoblasts locate in the inside of the syncytiotrophoblasts and act as stem cells[28,29].
COVID-19 is known to interact with endothelial cells and cause a hypercoagulative state, which can lead to the formation of microthrombi[30]. These outcomes occur by effects on maternal perfusion of the placenta and can manifest as accelerated villous maturation, infarction, intervillous thrombi, extravillous trophoblastic lesions, and subchorionic laminar necrosis in the membranes. In addition, when fetal circulation is affected, thrombosis of larger vessels, fibrous obliteration of vessels in the villi and breakdown of the endothelial cells within the villous stroma might appear.Comparison of placental histopathological examination of COVID-19-positive mothers can provide significant information about the effect of coronavirus on maternal and fetal outcomes. China researchers showed placental histopathological findings in COVID-19 positive patients that included increased perivillous fibrin deposition, villous infarcts, and chorioangioma[31].
Our results showed that two newborns were infected to SARSCoV-2 based on PCR after delivery. In a retrospective cohort study by Patberg et al that evaluated placental pathology in term confirmed pregnant women with SARS-CoV-2 showed that fetal vascular malperfusion and villitis of unknown etiology were the most common placental histopathologic findings, respectively[32].In a study of Baergen et al, 20 placentas from COVID-19 positive mothers were assessed and showed the fetal vascular malperfusion incidence in 40% and maternal vascular malperfusion in 15%[25].Based on the recent studies[33,34], pregnant women with COVID-19 have a higher risk of severe disease than no pregnant women, as their odds for intensive care unit (ICU) admission is five times and for receiving mechanical ventilation is four times higher than nonpregnant women. Based on our results, mothers’ ICU admission was 26.32% due to COVID-19 infection. In addition, Vivanti et al study showed trans-placental transmission of SARS-CoV-2 from a pregnant woman with COVID-19 during late pregnancy[6].
This study was the first histopathologic assessment of placenta in COVID-19 positive patients and gave us important information about the effect of SARS-CoV-2 infection on pregnancy outcomes and probability of trans-placental transmission of COVID-19 from a pregnant woman during late pregnancy in Iran. No control group in our study was one of limitation. Nevertheless, the authors suggested future studies by larger sample size and comparative studies with control subjects.
In conclusion, our results show that microvasculopathy, which is a sign of maternal vascular malperfusion, is a common finding in placentas from SARS-CoV-2 positive pregnant women. However,this study gives us important information that the effect of SARSCoV-2 infection on pregnancy outcomes during late pregnancy is probable. The authors suggested further studies with larger sample sizes and comparative studies between COVID-19 positive and negative, as well as information from patient follow-up to investigate the relationship between placental histopathological findings and pregnancy and maternal and fetal outcomes.
Conflict of interest statement
The authors declare to have no competing interests.
Funding
This study was funded by Qom University of Medical Sciences (No.1399-007).
Acknowledgments
The authors are very thankful for all personnel in Forqani Hospital and all mothers and their families that were corporate in this study.We are also grateful for Ethical Committee of Qom University of Medical Sciences that approved the study protocol with IR.MUQ.REC.1399.007 cod at 2020.03.17.
Authors’ contributions
Soheila Sarmadi and Monireh Mirzaie developed the main idea of the study and devised the study question and collected data.Elham Mirzaian, Roghayyeh Ahangari and Zahra Yazdi wrote the methodology section and documented the manuscript and collected data. Ara Omranipour and Azadeh Asgarian assisted in analyzing the data, interpreting the results, and formatting the document. All authors read and approved the final manuscript.
 Asian Pacific Journal of Reproduction2022年3期
Asian Pacific Journal of Reproduction2022年3期
- Asian Pacific Journal of Reproduction的其它文章
- Sjögren’s syndrome and reproductive outcomes
- Effect of cholesterol-loaded cyclodextrin enriched extenders on the quality of prefrozen and frozen buffalo semen
- Antioxidant potential of pentoxifylline on spermatozoa of small ruminants
- Sperm DNA fragmentation does not affect the clinical outcomes in the cumulative transfers of an ICSI cycle along with blastocyst transfers in couples with normozoospermic male patients
- Investigation of FOXP3 (rs3761548) polymorphism with the risk of preeclampsia and recurrent spontaneous abortion: A systemic review and meta-analysis
- Oxidative stress and female reproductive disorder: A review