
Isolated pancreatic metastasis from a malignant pleural mesothelioma diagnosed using endoscopic ultrasonography-guided fine needle aspiration biopsy
2022-04-29 06:30:42YukiIshikawaKakiyaHirotsuguMaruyamaKojiroTanoueShuseiFukunagaYasuakiNagamiYasuhiroFujiwara
Yuki Ishikawa-Kakiya, Hirotsugu Maruyama , Kojiro Tanoue, Shusei Fukunaga, Yasuaki Nagami, Yasuhiro Fujiwara
Department of Gastroenterology, Osaka City University Graduate School of Medicine, 1-4-3, Asahimachi, Abeno-ku, Osaka 545-8585, Japan
TotheEditor:
Malignant pleural mesothelioma is a rare and aggressive form of cancer with a poor prognosis [1] . Its progression is mainly a direct invasion from the primary lesion, and metastasis to distant regions rarely occurs. It was found that metastasis of malignant pleural mesothelioma may occur in the liver, adrenal glands, and kidneys in autopsy cases [2] . However, isolated pan- creatic metastasis is extremely rare, even in advanced malignant pleural mesothelioma; there are few cases diagnosed by surgery or autopsy. Herein, we report the first case in which endoscopic ultrasonography (EUS) and EUS-guided fine needle aspiration biopsy (EUS-FNAB) were useful in a case of isolated pancreatic metastasis caused by malignant pleural mesothelioma.
A 66-year-old man who had worked in a shipyard where he had been exposed to asbestos for 10 years, had a smoking history of 20 cigarettes per day for 5 years. He was previously diagnosed with epithelioid malignant pleural mesothelioma, and neoadju- vant chemotherapy was performed using cisplatin with peme- trexed. After chemotherapy, a pleurectomy/decortication was per- formed (4 years prior to this study). When right pleural recur- rence and lymph node metastasis were later discovered (3 years prior to this study), chemotherapy was initiated. Carboplatin with pemetrexed, gemcitabine, and nivolumab were administered; how- ever, contrast-enhanced computed tomography (CT) showed an en- hanced tumor in the right pleura ( Fig. 1 A). In addition, it revealed a 5 mm low-density area in the pancreatic body 9 months af- ter treatment, which increased to 12 mm in 3 months ( Fig. 1 B). Magnetic resonance imaging showed slight hyperintensity of the pancreatic body mass via T2-weighted imaging, while diffusion- weighted imaging of the mass showed hyperintensity with a clear boundary ( Fig. 1 C). An18F-fluorodeoxyglucose positron emission tomography scan showed weak uptake in the same region with a standardized uptake value of 3.19 ( Fig. 1 D). The pancreatic lesion was detected by EUS as a low-echoic lesion with a clear and regu- lar border ( Fig. 1 E). The main pancreatic duct was not affected, as it passed around the pancreatic lesion; this was not enhanced by contrast-enhanced ultrasonography. We suspected that the pancre- atic metastasis was a result of malignant pleural mesothelioma, as these were not images typical of invasive pancreatic ductal carci- noma; EUS-FNAB was therefore performed.
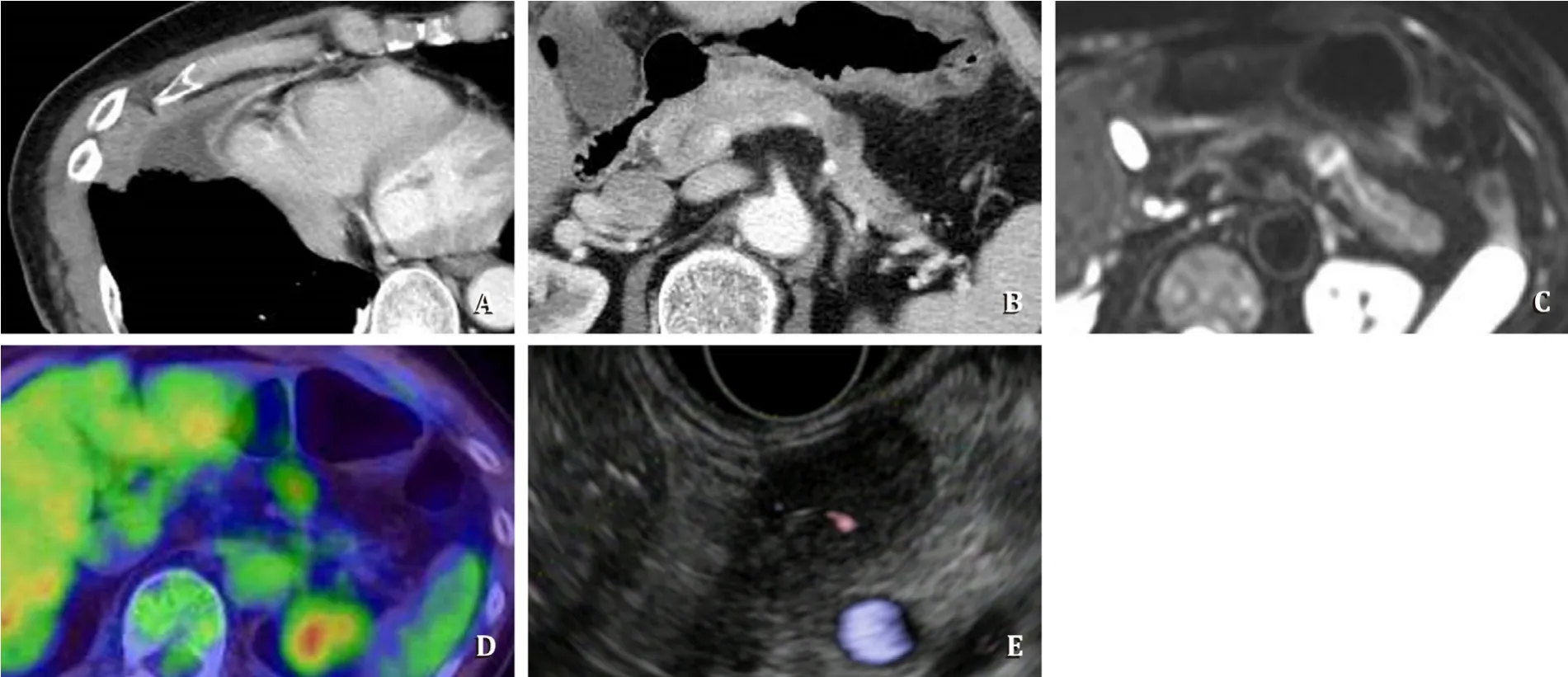
Fig. 1. A: Contrast-enhanced CT showing an enhanced lesion in the right pleura; B: contrast-enhanced CT showing a hypovascular lesion in the pancreatic body with- out dilatation of the tail side pancreatic duct; C: diffusion weighted imaging sequence of the mass, showing hyperintensity; D: 18 F-fluorodeoxyglucose positron emission tomography scan shows weak uptake in the pancreatic body; E: endoscopic ultrasonography showing a low-echoic lesion in the body of the pancreas.
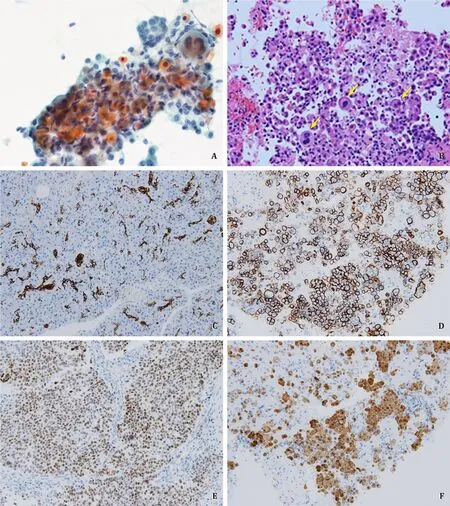
Fig. 2. A: Aspiration cytology showing orange-colored cytoplasm cells (Papanicolaou stain, original magnification × 40); B: yellow arrows indicate clumping cell (hematoxylin-eosin stain, original magnification × 20); C-E: immunohistochemical analysis revealed CK7 ( C ) , D2-40 ( D ), WT-1 ( E ), and calretinin ( F ) positivity (original magnification × 20).
A Papanicolaou stain showed a cluster of atypical cells with anisokaryosis and orange-colored cytoplasm ( Fig. 2 A), and some cell clusters were found using hematoxylin-eosin staining ( Fig. 2 B). Immunohistochemical analysis revealed CA19-9 and CD20 negativ- ity, as well as CK7, D2-40, WT-1, and calretinin positivity ( Fig. 2 C- F); thus, we diagnosed this lesion as pancreatic metastasis from malignant pleural mesothelioma in stage IV. Chemotherapy was subsequently performed, and the patient was administered vinorel- bine; he remains in good form 5 years after the initial diagnosis.
This is the first report regarding the use of EUS-FNAB to diagnose isolated pancreatic metastasis from malignant pleural mesothelioma. Pancreatic metastasis itself is extremely rare [2-4] , and isolated metastasis has only been reported in one case [5] . The images of pancreatic metastasis from malignant pleural mesothe- lioma are insufficient in the literature; in addition, EUS findings regarding pancreatic metastasis from malignant pleural mesothe- lioma have never been reported.
Generally, malignant mesothelioma is characterized as an en- hanced tumor. Metastasized lesions show various findings by contrast-enhanced CT [6] . In the present case, the isolated pan- creatic lesion was hypovascular. Pancreatic metastasis from malig- nant mesothelioma and invasive pancreatic carcinoma may be re- ported with a differential diagnosis; therefore, we performed EUS and EUS-FNAB. The pancreatic lesion was clear, and the edges were sharp based on EUS findings — characteristics not seen in inva- sive pancreatic ductal carcinoma. In addition, immunohistochemi- cal analysis was possible using EUS-FNAB.
Pancreatic metastasis from malignant pleural mesothelioma is rare. However, it is important to consider the possibility of metas- tasis. EUS and EUS-FNAB are useful for the diagnosis of pancreatic metastasis from malignant pleural mesothelioma.
Acknowledgments
None.
CRediTauthorshipcontributionstatement
YukiIshikawa-Kakiya:Conceptualization, Visualization, Writ- ing - original draft.HirotsuguMaruyama:Conceptualization, Su- pervision, Writing - original draft, Writing - review & editing.KojiroTanoue:Visualization, Writing - review & editing.Shu-seiFukunaga:Supervision, Writing - review & editing.YasuakiNagami:Supervision, Writing - review & editing.YasuhiroFuji-wara:Supervision, Writing - review & editing.
Funding
None.
Ethicalapproval
Written informed consent was obtained from the patient.
Competinginterest
No benefits in any form have been received or will be received from any commercial party related directly or indirectly to the sub- ject of this article.
 Hepatobiliary & Pancreatic Diseases International2022年2期
Hepatobiliary & Pancreatic Diseases International2022年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Meetings and Courses
- Information for Readers
- NAFLD or MAFLD: That is the conundrum
- Relevant Content
- Neutrophil-to-lymphocyte ratio or platelet-to-lymphocyte ratio is a predictive factor of pancreatic cancer patients with type 2 diabetes
- Nanosecond pulsed electric field interrupts the glycogen metabolism in hepatocellular carcinoma by modifying the osteopontin pathway