
Adaptive Wall-Based Attachment Ventilation: A Comparative Study on Its Effectiveness in Airborne Infection Isolation Rooms with Negative Pressure
2022-04-24 03:23YingZhngOuHnAnguiLiLiHouThomsOlofssonLinhuZhngWenjunLei
Engineering 2022年1期
Ying Zhng, Ou Hn, Angui Li,,*, Li’n Hou,*, Thoms Olofsson, Linhu Zhng, Wenjun Lei
a School of Building Services Science and Engineering, Xi’an University of Architecture and Technology, Xi’an 710055, China
b Department of Applied Physics and Electronics, Umeå University, Umeå SE 90187, Sweden
c School of Thermal Engineering, Shandong Jianzhu University, Jinan 250101, China
Keywords:Ventilation efficiency Air change rate COVID-19 Attachment ventilation Air distribution Isolation ward
ABSTRACT The transmission of coronavirus disease 2019(COVID-19)has presented challenges for the control of the indoor environment of isolation wards. Scientific air distribution design and operation management are crucial to ensure the environmental safety of medical staff. This paper proposes the application of adaptive wall-based attachment ventilation and evaluates this air supply mode based on contaminants dispersion,removal efficiency,thermal comfort,and operating expense.Adaptive wall-based attachment ventilation provides a direct supply of fresh air to the occupied zone. In comparison with a ceiling air supply or upper sidewall air supply, adaptive wall-based attachment ventilation results in a 15%–47%lower average concentration of contaminants, for a continual release of contaminants at the same air changes per hour (ACH; 10 h-1). The contaminant removal efficiency of complete mixing ventilation cannot exceed 1. For adaptive wall-based attachment ventilation, the contaminant removal efficiency is an exponential function of the ACH. Compared with the ceiling air supply mode or upper sidewall air supply mode, adaptive wall-based attachment ventilation achieves a similar thermal comfort level(predicted mean vote (PMV) of -0.1–0.4; draught rate of 2.5%–6.7%) and a similar performance in removing contaminants, but has a lower ACH and uses less energy.
1. Introduction
During an infectious disease pandemic,such as coronavirus disease 2019 (COVID-19), Middle-East respiratory syndrome (MERS),or severe acute respiratory syndrome (SARS), the risk of transmission between patients and healthcare workers (HCWs) greatly increases. It has been reported that the diffusion of droplets from the respiratory tract and intimate contacts are the main transmission routes of COVID-19 [1]. Moreover, aerosol transmission has been suggested to be an additional—yet important—pathway on the basis of clinical observations in confined spaces [2,3]. A retrospective cohort study suggested that airborne spread may have had an important role in the transmission of SARS [4,5]. Many other viruses, such as rhinovirus, influenza, and adenovirus, are spread by the airborne route [6,7]. In addition to taking personal protection (i.e., protective clothing, medical masks, goggles, etc.)and decontamination(i.e.,handwashing,surface cleaning,and disinfection) measures, the airflow distribution of the airborne infection isolation room (AIIR) should be addressed [4,8,9].
The purpose of the AIIR should be to minimize the threat of exposure to the medical staff within the isolation room and to others outside of the room to the airborne infectious media. Air changes per hour (ACH) and air distribution are important factors in reducing contaminant concentration in hospital buildings[10,11]. The ACH is commonly used as a measure of how quickly the supply air spread throughout the entire volume of air in the room [12]. Many studies have observed that a lower ACH can increase the risk of airborne cross-infection [13,14]. In research studies,ACHs of 3.0–29.9 h-1have been adopted[15–17].In different national regulations and the World Health Organization(WHO)recommendations, ACHs range from 6 to 15 h-1[12,18–23]. Field test studies have also shown that new isolation rooms do not always comply with an ACH of 12 h-1, and as many as 21%(3/14) of tested isolation rooms violated the lowest requirement of 6 h-1for existing buildings [24]. Lower ACHs are used in order to conserve energy[25,26].However,the ACH describes the ventilation in a room as a whole,and assumes a complete mixing of the supply air throughout the entire volume. The degree of mixing of ventilation air depends on the air distribution.
There are many different air distribution modes for built environments [27]. The general principles for AIIRs are to achieve and maintain a directional air distribution from a clean area to a less clean area [28,29] and to position exhaust vents as close to contaminant sources as possible [12]. The air distribution in a built environment is mainly determined by the positions of the supply and exhaust vents; the Reynolds number (Re), as it is generally known that the supply air Re relates to the ACH; the Archimedes number (Ar) of the supply air [26]; and other potential confounders. Ceiling and sidewall air supply modes are usually used,based on mixing ventilation under the assumption that the air in the room is completely mixed[15,17]. The concept of mixing ventilation was originally developed from the perspective of thermal comfort considerations [26], so it does not promote better inhaled air quality [30,31], especially when there is a point source of air pollutants, as in the case of airborne infectious disease spread[32].Displacement ventilation is created using the buoyancy forces from heat sources in the room[33].The contamination distribution in a displacement-ventilated room depends on the position of the contamination sources and their association with the heat sources[27].Since air is supplied directly to the occupied zone,the ACH is limited in order to avoid undesirable thermal sensation. Wallbased attached ventilation is therefore proposed, based on a combination of mixing ventilation, displacement ventilation, and impinging jet flow. An air jet with high momentum can be maintained by the air jet attaching to the wall and reaching the occupied zone with acceptable air velocity via imping. The background mechanism of this concept is the extended Coanda effect (Coanda–Li effect) [27,34], firstly proposed by Li, which is the tendency of a fluid jet to continually attach to a complex of convex and concave surfaces after impinging [35].
In this paper, the concept of wall-based attachment ventilation is extended to an adaptable form according to the requirement of the AIIR. In adaptive wall-based attachment ventilation, the jet impinging zone is elevated to the zone occupied by the HCWs. In the discussion below, the performance of adaptive wall-based attachment ventilation is evaluated and compared with those of two traditional air supply modes (ceiling air supply and upper sidewall air supply). Both constant and transient air contaminant sources are taken into account.Removal efficiency and availability of air supply are calculated for different air distribution modes.
2. Theoretical model of adaptive wall-based attachment ventilation
Adaptive wall-based attachment ventilation is based on vertical attachment ventilation. The airflow structure is shown in Fig. 1.When an isothermal airflow near to a vertical solid surface is a jet, the jet is deflected and attaches to the surface due to the Coanda effect, as shown in Region I. Based on the inertia momentum, the jet moves in the original direction, reaches a separation point (Separation point I), and causes a stagnation phenomenon after collision. The pressure of the stagnation zone, which is the area between the separation point and the reattachment point, is close to the ambient pressure. In the region downstream of the stagnation point, the static pressure increases and reaches a maximum value. With the recovered static pressure, the jet fluid overcomes the wall resistance and moves horizontally, as shown in Region II.In vertical attachment ventilation,the airflow attaches to the floor in Region II. The key to the jet movements shown in Regions I and II is the virtual origin inlet[36],which is determined by the extended Coanda effect zone of the real jet inlet that determines the horizontal jet range shand the axis velocity attenuation vmax/v0of the air supply (v0is the supply air velocity of the slot inlet). The final result of the axis velocity attenuation is the designed air velocity in the occupied zone.Theoretical and experimental studies on the virtual origin inlet and the extended Coanda effect with planar surfaces can be found in Ref. [37].
Although the air supply jet plays a leading role in the ventilation of a room,there are many potential confounders,such as contaminant sources, thermal buoyancy, obstacles in the flow path,and so forth. Therefore, computational fluid dynamics (CFD) validated by experimental results was adopted to study the application of adaptive wall-based attachment ventilation in AIIRs.
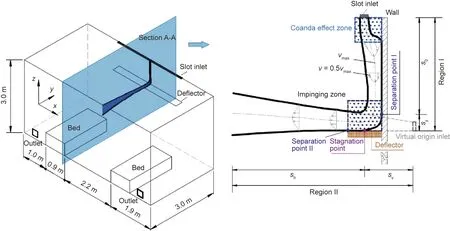
Fig. 1. Adaptive wall-based attachment ventilation used in AIIR and its airflow structure. Region I: vertical attachment region; Region II: horizontal jet region; s0: vertical attachment length;sy:distance between Separation point I and the stagnation point;sv:distance between the virtual origin inlet and the stagnation point;sh:horizontal jet range;v: the jet axis velocity;v: velocity at different locations.
3. Materials and methods
Researchers in the field of indoor environment studies have adopted CFD as a useful tool for predicting air movement in ventilated spaces. This method has been used as a research tool for many years [38,39]. In hospitals such as the Huoshenshan and Leishenshan Hospitals (the two hospitals built in Wuhan, China),which needed to be rapidly built over a short time period, it is often difficult to solve design problems using field experimental methods. In this case, CFD can produce scientific numerical calculations on air distribution and effective control methods for contaminated air in isolation wards by means of validated numerical models.
3.1. Physical model and ventilation configurations
A normal two-bed AIIR was adopted for the current study; it includes a ventilation system, contaminant sources,and beds.The dimension of the ward is 6 m×3 m×3 m(length×width × height). The exhaust vent is close to the floor [23], while the air supply vent is in the ceiling or upper sidewalls, with the aim of forming a clean directional airflow path. We highlight the air supply modes,as the sink flow at the exhaust vents has a much smaller effect on the flow field. For ceiling air supply and upper sidewall air supply, there are three inlets with a size of 0.32 m ×0.12 m each. For adaptive wall-based attachment ventilation, the inlet is a slot with a size of 3 m× 0.05 m.For each mode,the outlets are on the lower part of the wall,near the contaminant sources(i.e., the patients), and have a size of 0.25 m × 0.25 m each.Detailed layouts of the air vents are shown in Fig.S1 in Appendix A.
3.2. Governing equations and turbulent model
The airflow of the ward is described with basic equations of mass, momentum, energy, and species transportation, which can be found in Ref. [40].
One of the keys to successful CFD application in an indoor environment is the turbulence model.Based on the preliminary results[41], the turbulent model shear stress transport (SST) k–ω (k:specific turbulent kinetic energy (m2·s-2); ω: specific turbulent dissipation rate(s-1))was adopted.The quasi-steady and unsteady conditions were both included.As the air velocity in an indoor built environment is relatively slow, the air is assumed to be incompressible[42].The Boussinesq approximation was adopted to solve the equations with density [43].
3.3. Boundary conditions and grids
In the simulation,the walls,floors,and ceilings are non-slip surfaces.A pressure outlet at-10 Pa is used for the outlets.The tracer gas(i.e.,contaminants)is assumed to be released from the heads of the patients in the ward[24,44]. Based on the literature,given the most unfavorable conditions for the environment of medical staff in an isolation ward,the rate of contaminants generated is 0.7 L·s-1under steady conditions [45,46] and 10 L·s-1for 2 s with a frequency of 40 counts per hour under unsteady conditions [47–49].As mentioned in Section 1,the air change rates of AIIRs ranging from 6 to 15 h-1are adopted. Due to the buoyancy of warm air,winter is the most unfavorable working condition for ventilation.Therefore, this paper focuses mainly on winter conditions. A total of 21 typical cases under different boundary conditions are studied and compared, as shown in Appendix A Table S1.
The geometry of the calculation domain is regular. Three kinds of unstructured grids with total numbers of 0.100 million, 0.195 million, and 0.392 million are used, respectively. The dimensionless air velocity, temperature, and concentration of the occupied zone at the height of 2 m vary with the dimensionless horizontal distance from the inlet,as shown in Appendix A Fig.S2.The dimensionless parameters are defined in Appendix A Table S2 for analysis. The results show that 0.195 million grids can ensure calculation accuracy under these conditions with fewer computing resources.
3.4. Experimental validation
As axis velocity attenuation is the key to the whole flow field.This work collects the experimental data from the research team’s previous wall-based attachment ventilation studies [35,37,41,50]and semi-empirical formulas from the American Society of Heating, Refrigerating and Air-Conditioning Engineers (ASHRAE) [26],Topp et al. [51], Yu et al. [52], and Rajaratnam [53] to validate the numerical model, as shown in Fig. 2. These formulas correspond to a variety of empirical coefficient K, which is related to inlet type, for describing the axis velocity of a wall-based attachment air supply. The dimensionless results of CFD are compared with these data. The range of errors is 4.0%–9.3% (cf. Ref. [51])when the temperature difference between the supply air and the wall is 5 °C (warm air). For cool air, the temperature difference between the supply air and the wall is-4 °C,and the errors range from 0.2%to 7.4%(cf.Ref.[52]).Here,Refs.[51,52]were chosen for comparison because they use the same inlet type. There is good agreement between the CFD results and the experimental results,so the numerical model can be used to carry out further analysis.The flow pattern and the jet axis velocity and temperature distribution are shown in Appendix A Figs. S3 and S4.
4. Results and discussion
4.1. Contaminant concentration dispersion
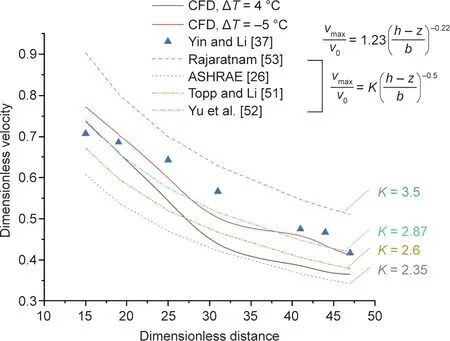
Fig. 2. Experimental validation of the axis velocity attenuation of adaptive wallbased attachment ventilation.K:the empirical coefficient related to inlet type;ΔT:the temperature difference between the supply air and the wall; h: the distance between the slot inlet and the floor;z:different height from the floor;b:the width of the slot inlet.
According to the modified Wells–Riley equation [54], airborne contamination should be kept low in order to reduce the risk of infection. Given the most unfavorable working conditions, the patients continually release contaminants into the environment.At the same ACH, the average contaminant concentration of the occupied zone is the lowest (0.45%) for adaptive wall-based attachment ventilation, followed by that for the ceiling air supply mode(0.95%),shown in Fig.3.The cause can be analyzed according to the velocity of the cross-section. Zhao et al. [55] simulated air movement and aerosol particle concentration and deposition using a discrete trajectory model in mixing (upper sidewall air supply)and displacement ventilation rooms.It was found that mixing ventilation has a lower indoor particle concentration, but the deposition rate is larger. Zhao et al. [55] pointed out that this finding did not necessarily mean that mixing ventilation will lead to better indoor air quality,because the deposited particles may re-suspend.
For ceiling air supply,there is a downdraft under each inlet,and the updraft is along the sidewalls.The contaminated air is induced by the momentum of the supply airflow along the wall and ceilings after the release, and turns downward. The contaminants are diluted and diffused throughout the entire ward before finally being exhausted through the outlets. This mode can cause contaminants to circulate repeatedly in the ward, increasing the risk of infection of the medical staff.Qian et al.[17]showed a flow visualization of cool air with a high supply velocity from the diffuser right above the head. Their results also showed strong entraining of the surrounding contaminated air from exhalation in spite of the high supply air velocity. In the present research,the average contaminant concentration of the upper sidewall air supply mode is 1.4% (noting that 0.45% for adaptive wall-based attachment ventilation). The airflow moves along the ceiling after coming out of the inlets on the upper sidewall, and turns downward when reaching the opposite wall. Airflow cannot be efficiently supplied to the occupied zone due to buoyancy between the supply air and indoor air in winter. Ceiling air supply and the upper sidewall air supply are the most popular modes in public buildings. However, the requirements of isolation wards are stricter than those of other public places, including common hospitals.Adaptive wall-based attachment ventilation is an improvement of the traditional ventilation mode that combines the advantages of mixing ventilation and displacement ventilation.In addition,adaptive wall-based attachment ventilation focuses on providing a direct supply of fresh air to the occupied zone. It is found that the airflow first attaches to the vertical wall near the inlet;it then reaches the deflector (2 m above the floor), and turns toward the occupied zone. To supply warm air in winter, the upward deflection of the airflow can be changed by adjusting the angle of the deflector, so that fresh air can be directly supplied to the zone occupied by medical staff and patients.
Respiratory diseases often cause repeated coughing or sneezing.As a result,intermittent release of a large amount of contaminants can occur. In order to simplify the condition of intermittent exhaled contaminants, tracers are regularly released, shown as the right y-axis in Fig. 4(a). The transient source causing the concentration distributions varies with time. To evaluate the performance of the air distribution, the concentration of the outlets over time was integrated, as shown in Fig. 4. Adaptive wallbased attachment ventilation achieves the highest concentration of outlets and the greatest concentration integration over time,followed by those of an upper sidewall air supply. This is because adaptive wall-based ventilation supplies air to the occupied zone directly, which pushes out more contaminants. The outlets’ accumulated concentration of mixing ventilation depends on the dilution time. When the release frequency is higher than the dilution time, contaminants accumulate continuously. The dilution time in minutes that is required for certain airborne contaminant removal efficiencies, as mentioned in Refs. [12,20,22], can be traced to a manual on industrial ventilation published by the American Conference of Governmental Industrial Hygienists(ACGIH)[56].This dilution time is used to calculate the duration of dilution after contaminant sources are interrupted. However, the time should be evaluated with an effective ACH while considering K,which is a factor reflecting the degree of incomplete mixing.The K value is selected based on the locations of inlets and outlets,the working process, the typical locations of staff relative to the sources of contamination,and so forth.However,complete mixing usually does not occur,and the mixing factor K can be as high as 10[29,56].
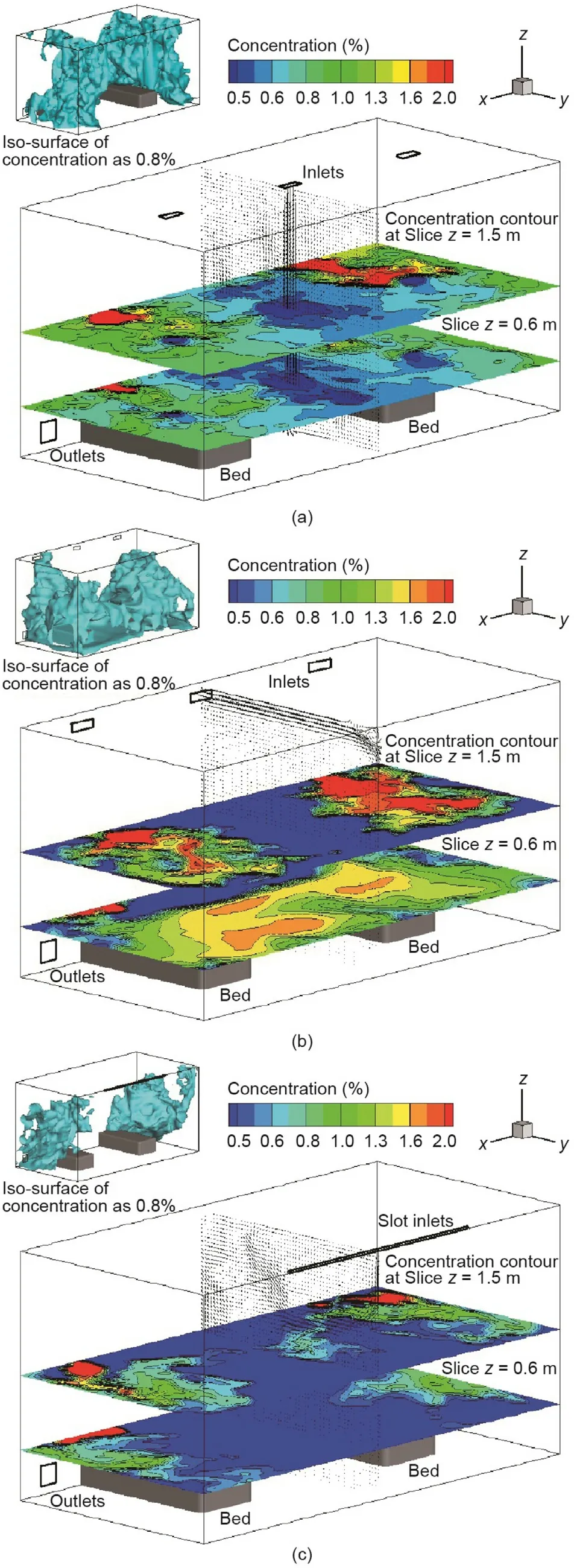
Fig. 3. Contaminant concentration distribution in an isolation ward with the same ACH under different air supply modes:(a)ceiling air supply;(b)upper sidewall air supply; and (c) adaptive wall-based attachment ventilation.
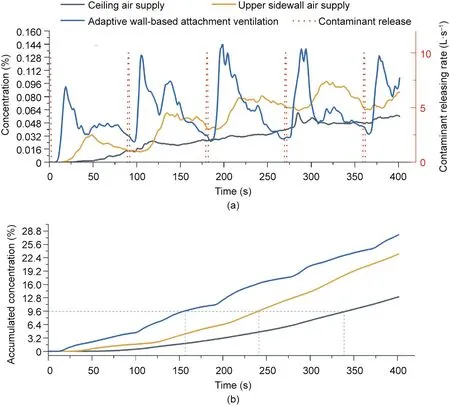
Fig.4. Mean concentration of outlets under the condition of intermittent exhaled contaminants.(a)Concentration versus time;(b)accumulated concentration versus time.
4.2. Ventilation performance
Contaminant removal efficiency (also called removal effectiveness or ventilation efficiency) is recommended as the index to evaluate ventilation performance [57,58]. For the same ACH, the removal efficiency of adaptive wall-based attachment ventilation is the highest of the three air supply modes in both winter and summer. In winter, the removal efficiency is 1.33, which is followed by that of ceiling air supply,at 1.04.In summer,the removal efficiency of adaptive wall-based attachment ventilation is 1.93,which is followed by that of upper sidewall air supply, at 0.92, as shown in Appendix A Fig. S5. The removal efficiency of adaptive wall-based attachment ventilation is 1.3–2.5 times greater than that of ceiling air supply. This is because the airflow of adaptive wall-based attachment ventilation turns toward the target zone by impinging the deflector. Fresh air is thus supplied to the HCWs and patients.However,for complete mixing ventilation,the maximum removal efficiency is 1.0 [59]. This means that the contaminants are mixed throughout the air of the entire room, and the occupied zone is contaminated as much as the exhaust vent.In this case, the fresh air supplied is not fully utilized. The results of Cheong and Phua [15] showed that the local removal efficiency at the HCWs’positions ranges from 0.91 to 1.12 in AIIRs with ceiling air supply and lower exhausts in the sidewall.The removal efficiency exceeds 1.0 when the sampling points are right under the air supply vents at 1.4 m height. In practice, an air supply that directly vents toward the occupants is unacceptable due to undesirable draughts.
By increasing the ACH, the removal efficiency of adaptive wallbased attachment ventilation increases significantly,while those of ceiling air supply and upper sidewall air supply remain around 1.0,as shown in Fig. 5 [23,60]. In an experiment, Berlanga et al. [61]carried out four kinds of mixing ventilation configurations.For very similar air distribution modes with ceiling air supply and low sidewall exhaust,the removal efficiency ranged from 0.97 to 0.99 when the ACHs varied from 6 to 12 h-1.According to the theory of complete mixing ventilation,the removal efficiency cannot exceed 1.0,despite a continuous increase in ACH. For adaptive wall-based attachment ventilation, the relation between ACH and removal efficiency (E) can be obtained by exponential function fitting, as in Eq. (1):

where E0, A, and R0are coefficients of the fitting formula;E0= –0.96 ± 1.71, A = 0.51 ± 0.65, and R0= 0.16 ± 0.06, with R2=0.98.It has also been reported that variation occurs in removal efficiencies according to the ACHs of other air distribution modes,such as displacement ventilation and stratum ventilation. Tian et al.[62]found that the removal efficiencies were 1.10–1.49 when the ACHs were 2.2–4.7 h-1. Mateus and Carrilho da Graça [63]tested the removal efficiencies of displacement ventilation and found that the average value was 1.7 when the ACH was 4.4 h-1.Although these two studies were not aimed at AIIRs,their core idea for airflow distribution is to move clean air into the occupied zone. Adaptive wall-based ventilation has a similar principle. By supplying fresh air to the occupied zone directly, these studies achieved higher removal efficiencies. However, these studies used limited ACHs because the air supply vents of displacement ventilation and stratum ventilation are usually directly aimed toward the occupants.Thus,increasing the ACH may lead to a high air velocity, with a greater risk of a draught at floor level [64]. For adaptive wall-based ventilation, the air velocity decays by impinging the deflector before entering the occupied zone.Thus,air can be supplied with an ACH as large as the rate required for mixing ventilation, but with greater removal efficiency.
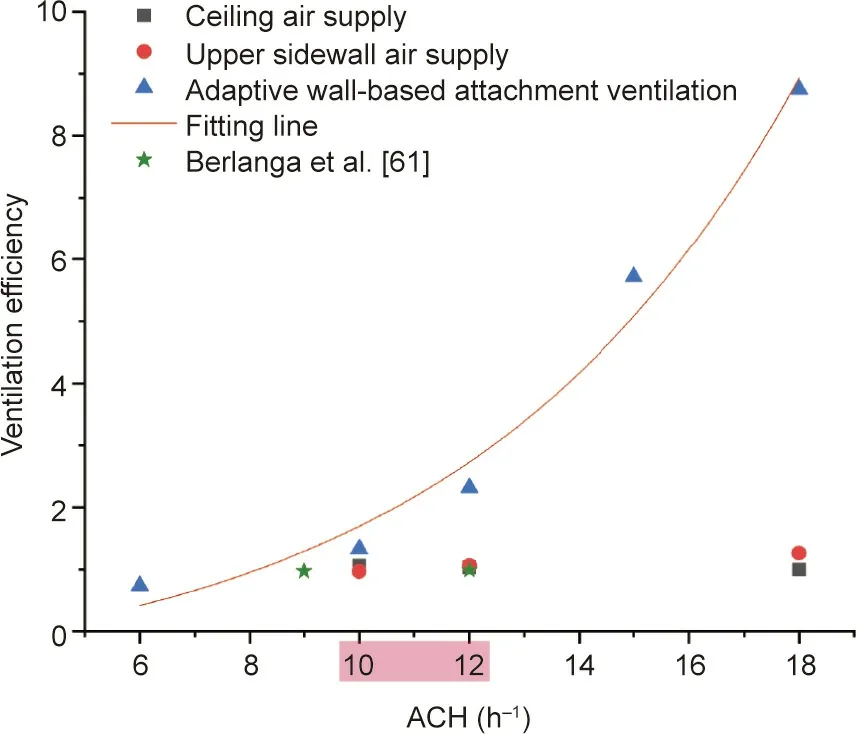
Fig. 5. Removal efficiency of the air distribution mode for varying ACHs. The ACHs in the red box is the recommended range [23,60].
4.3. Effect of negative pressure
To prevent contaminants from leaking out from the isolation ward, a negative pressure should be maintained. In the present research, a range from 0 to -30 Pa was used to determine how the negative pressure affects the flow fields and ventilation in the isolation wards. The removal efficiency ranged from 1.31 to 1.48 when the negative pressure of the outlets was changed. The result can be fitted linearly with a slope of 0 and the residual sum of squares 0.02, as shown in Appendix A Fig. S6. This finding illustrates that, in practice, the negative pressure of the outlets has barely any influence on air distribution.There are vertical pressure gradients in the studied isolation ward due to the air stack effect.The largest negative pressure appears near the outlets,while the smallest pressure is near the inlet due to the boundary conditions at the inlets and outlets.
There is insufficient scientific evidence regarding the pressure difference limit values that are required to prevent the escape of infectious air from an AIIR [65]. As Xu and Zhou [66] pointed out,a negative pressure within the AIIR can only prevent the leakage of contaminants and has nothing to do with protecting the medical staff. In different countries and districts, the commonly required value of negative pressure is different. According to US guidelines[12], the pressure difference between the AIIR and the corridor should be at least 2.5 Pa. In the United Kingdom, this value is 5 Pa [18]. Nordic countries require the pressure difference to be 15 Pa [20,22], while an even higher pressure difference of 30 Pa is recommended in Australia[29].In practice,a small pressure difference is not enough to hold against variable weather conditions,especially when the airtightness of an AIIR is insufficient [65]. Li et al. [67] found that the pressure difference criteria of -2.5 Pa was met in 97% of the 38 rooms tested (mean -7.7 Pa for all the rooms tested) in SARS isolation wards in Hong Kong, China.Alevantis et al.[68]suggested that the negative pressure in an AIIR should be at least-7 Pa to prevent the leakage from exceeding 1%.Due to both the effect on removal efficiency and the pressure distribution, a large negative pressure for the outlets is unnecessary.
4.4. Thermal comfort and economic analysis
To assess the thermal conditions in the room, environmental parameters and different local discomfort indices were obtained,as presented in Appendix A Table S3. To maintain a comfortable indoor thermal environment, assuming that the heating load is 40 W·m-2in winter and the cooling load is 60 W·m-2in summer,the indoor air temperature is required to be 20–22°C in winter and 26–27 °C in summer [23]. According to the balance of heat and mass, the supply air temperature is 24 °C in winter and 21 °C in summer for the ceiling air supply mode using an ACH of 10 h-1,while the temperature is 24.6 °C in winter and 20 °C in summer for adaptive wall-based ventilation with an ACH of 8.5 h-1.
Adaptive wall-based attachment ventilation can meet all the requirements [23,69] for air temperature and air velocity as well as the ceiling air supply mode. The thermal comfort indices, predicted mean vote (PMV), and draught rate (DR) were adopted to evaluate the thermal environment [70]. An HCW is considered to be a standing person performing a light activity (1.4 met), while the patients are considered to be quietly sitting (1 met) [60]. As the HCWs and patients have different metabolic rates, their thermal comfort levels are different. When using adaptive wall-based attachment ventilation, the HCWs’ and patients’ thermal comfort levels in both winter and summer are within the thermal comfort interval (-1, 1). The HCWs feel slightly warm in both winter and summer due to their light activity, while the patients’ thermal comfort levels are lightly cool in winter and lightly warm in summer. In winter, with the same ACH, the PMV results for adaptive wall-based attachment ventilation comply with regulation EN-16798 from Energy performance of buildings—ventilation for buildings—Part 1 in European Union(EU)countries[71].This is because the extended Coanda effect in adaptive wall-based attachment ventilation helps to maintain a downward momentum against buoyancy, enabling air to be effectively supplied to the occupied zone. For the same reason, the DRs of adaptive wall-based attachment ventilation (6.7%) are a bit higher than those of mixing ventilation in summer,although they still meet the requirement of EN-16798 [71]. Berlanga et al. [61] found that HCWs (with a PMV of 0.39–0.72) felt warmer than patients (with a PMV of -0.32 to-0.07) under different mixing ventilation modes. In their study,when the ACH increased, the PMV for the ceiling air supply mode did not change.Aganovic et al.[72]proposed a protected occupied zone ventilation by using an air curtain between HCWs and patients.At a short distance from the air supply,the DRs of different body parts were evaluated,and were found to range from 0.9%to 31.0% [72].
It is noted that adaptive wall-based attachment ventilation achieves a slightly better thermal environment with the same removal efficiency and a lower ACH when compared with the ceiling air supply mode.From the perspective of system configuration,adaptive wall-based ventilation uses slots instead of grills or diffusers. A specialized hospital for the airborne infection isolation of diseases was taken as an example for economic analysis. The hospital has ten sections for patients with confirmed cases, and each section has 20 AIIRs. The air in each section is controlled by an air handling unit and a set of air transmission systems. As the heating and cooling load are respectively the same for both air distribution modes, the main operating energy costs come from the fans of the air transmission systems. For adaptive wall-based ventilation with an ACH of 8.5 h-1,the fan capacity is 85%of that of the ceiling air supply mode with an ACH of 10 h-1.An economic analysis comparison of one section is shown in Appendix A Table S4.Although the proposed system increases the initial material costs and the labor costs of the deflector,it saves air duct material costs due to the reduction of the total air volume, and saves operating costs due to less ACH. Therefore, adaptive wall-based attachment ventilation is economically feasible and more energy efficient than other options.
5. Conclusions
Studies have shown that better ventilation can greatly reduce the suspension time of respiratory droplets in the air. In order to establish suitable ventilation strategies for isolation wards, the application of adaptive wall-based attachment ventilation was studied and compared with the ceiling air supply and upper sidewall air supply modes. Contaminant source emission characteristics, negative pressure, and outdoor climate were taken into account. Three aspects of different air distribution modes, including contaminants dispersion, removal efficiency, and indoor thermal comfort, were evaluated by indexes. It can be concluded that adaptive wall-based attachment ventilation can create a clean and comfortable occupied zone for medical staff and patients with less energy use than other air transmission systems.
(1) Adaptive wall-based attachment ventilation can supply fresh air to the zone occupied by medical staff and patients.Under the constant release of contaminants, with the same air change rate (10 h-1), adaptive wall-based attachment ventilation has the lowest average contaminant concentration in the occupied zone(winter 0.45%,summer 0.29%),followed by ceiling air supply(winter 0.95%, summer 1.91%) and upper sidewall air supply (winter 1.4%, summer 1.19%). Adaptive wall-based attachment ventilation provides greater access to fresh air supply than the other two modes. When intermittent releases of a large number of contaminants occur, the concentration of contaminants varies with time.Within the same duration, adaptive wall-based attachment ventilation exhausts the greatest quantity of contaminants.
(2) A formula associating air change rate with removal efficiency for adaptive wall-based attachment ventilation can be obtained based on an exponential function.When air change rates increase,the removal efficiency of adaptive wall-based attachment ventilation increases significantly,while those of ceiling air supply and upper sidewall air supply remain at around 1.0.For an ACH of 10 h-1, the removal efficiency of adaptive wall-based attachment ventilation is 1.3–2.5 times greater than that of ceiling air supply.
(3) The effect of negative pressure only appears locally around the exhaust vent.It barely has any influence on the air distribution of adaptive wall-based attachment ventilation. Thus, with this mode, there is no need for a large negative pressure in isolation wards.
(4) Under the same heating and cooling load, adaptive wallbased attachment ventilation can achieve the same removal efficiency and a similar thermal comfort level as ceiling air supply,but with a 15% lower ACH. A lower ACH also means that less duct area is required in terms of material investment. The duct area saved when using this mode is 12.6 times greater than the increased area of the deflector that is required for this mode.Thus,adaptive wall-based attachment ventilation is both economically feasible and more energy efficient than other options.
Acknowledgments
The study was supported by the Ministry of Science and Technology of China, the Chinese Academy of Engineering, a project on the risk prevention and control of the relationship between the spread of COVID-19 and the environment (2020YFC0842500 and 2020-ZD-15),and the National Key Research and Development(R&D) Program of China (2017YFC0702800).
Compliance with ethics guidelines
Ying Zhang, Ou Han, Angui Li, Li’an Hou, Thomas Olofsson, Linhua Zhang, and Wenjun Lei declare that they have no confict of interest or financial conflicts to disclose.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.eng.2020.10.020.

- Engineering的其它文章
- Editorial for the Special Issue on 6G Requirements, Vision, and Enabling Technologies
- The Drive for Electric Motor Innovation
- Direct Air Carbon Capture Takes Baby Steps—Giant Strides Are Needed
- Start-Ups Seek to Accelerate Path to Nuclear Fusion
- 6G:Ubiquitously Extending to the Vast Underwater World of the Oceans
- Industrial Wireless Control Networks: From WIA to the Future