
儿童难治性肺炎支原体肺炎炎症特征及糖皮质激素的治疗价值
2022-03-27 10:33:24周琴孔海波
中国现代医生 2022年5期
周琴 孔海波


[摘要] 目的 分析難治性肺炎支原体肺炎的炎症特征及Mp-DNA载量的表达,寻找早期识别的最佳指标;研究甲基泼尼龙治疗前后炎症指标及Mp-DNA的动态变化。方法 选取2018年9月至2020年8月间浙江省人民医院收治的152例肺炎支原体肺炎(MPP)患儿为研究对象,根据诊断标准将患儿分为普通MPP(GMPP组,n=80)和RMPP组(n=72)。对两组患儿在血清CRP、LDH,细胞因子(IL-1β、IL-6、IL-8、IL-17、IL-18),Mp-DNA的差异进行统计学分析,绘制ROC曲线分析各独立危险因素在RMPP中的预测价值。RMPP组进一步测定甲基泼尼龙治疗前后血清CRP、LDH、细胞因子及MP-DNA的变化。结果 ①RMPP组CRP、LDH、IL-1β、IL-6、IL-8、IL-18和Mp-DNA水平明显高于GMPP组,差异有统计学意义(P<0.001);而IL-17在两组间比较,差异无统计学意义(P>0.05)。②RMPP组激素治疗后,CRP、LDH、IL-1β、IL-6、IL-8及IL-18水平明显较激素治疗前下降,差异有统计学意义(P<0.001)。而IL-17和Mp-DNA在激素治疗前后,差异无统计学意义(P>0.05)。③ROC曲线分析显示,CRP、LDH、IL-1β、IL-6、IL-8及IL-18用于鉴别RMPP和GMPP患儿具有较好价值,其最佳阈值分别为12.75 mg/L、432.50 IU/L、13.42 pg/ml、13.28 pg/ml、5.55 pg/ml、227.50 pg/ml。结论 血清CRP、LDH、IL-1β、IL-6、IL-8、IL-18水平明显升高有助于早期识别RMPP,激素治疗可抑制机体的免疫炎症反应,从而缓解RMPP患儿的临床症状。
[关键词] 肺炎支原体肺炎;难治性;细胞因子;糖皮质激素
[中图分类号] R725.6 [文献标识码] B [文章编号] 1673-9701(2022)05-0069-04
[Abstract] Objective To explore the inflammatory characteristics and the expression of Mp-DNA load in patients with refractory mycoplasma pneumoniae pneumonia, and to find the best index for early identification. To study the dynamic changes of inflammatory indexes and Mp-DNA before and after methylprednisolone treatment. Methods Children with MPP hospitalized between September 2018 to August 2020 were selected as study subjects in Zhejiang Provincial People's Hospital. According to the diagnostic criteria, children were divided into GMPP group (n=80) and RMPP group (n=72). The differences in serum CRP, LDH, cytokines (IL-1β, IL-6, IL-8, IL-17, IL-18), and Mp-DNA between the two groups of children were statistically analyzed, and ROC curve analysis was drawn the predictive value of each independent risk factor in RMPP. Results (1)The levels of CRP, LDH, IL-1β, IL-6, IL-8, IL-18 and Mp-DNA in RMPP group were significantly higher than those in GMPP group, and the difference was statistically significant (P<0.05). However, there was no statistically significant difference in IL-17 between the two groups (P>0.05). (2)After hormone therapy in RMPP group, the levels of CRP, LDH, IL-1β, IL-6, IL-8 and IL-18 were significantly lower than before hormone therapy, the difference was statistically significant (P<0.05). However, there was no statistically significant difference between IL-17 and Mp-DNA before and after hormone treatment (P>0.05). (3)ROC curve analysis showed that CRP, LDH, IL-1β, IL-6, IL-8 and IL-18 had good value in distinguishing children with RMPP and GMPP. The optimal thresholds were 12.75 mg/L,432.5 IU/L,13.42 pg/ml,13.28 pg/ml,5.55 pg/ml,227.50 pg/ml. Conclusion Significant increase in serum CRP, LDH, IL-1β, IL-6, IL-8, and IL-18 levels is helpful for early recognition of RMPP. Hormone therapy mainly suppresses the body′s cellular immune response, reduces systemic inflammatory damage, and relieves clinical symptom.
[Key words] Mycoplasma pneumoniae pneumonia; Refractory; Cytokine; Glucocorticoids
肺炎支原体(mycoplasma pneumonia,MP)是儿童社区获得性肺炎(community acquired pnuemonia,CAP)的常见病原体之一,MP可占CAP病例的10%~30%[1]。近年来随着儿童肺炎支原体肺炎(mycoplasma pneumoniae pneumonia,MPP)发病率的上升,难治病例明显增多,患儿应用大环内酯类抗生素治疗后病情未见好转,并且可引起多器官、多系统的肺外并发症[2-4]。
目前,RMPP早期缺乏特异的诊断方法及生物标志物。近年来,有研究认为MP感染时过强的炎症反应可能是RMPP的重要原因[5]。而糖皮质激素是目前最有效的抗炎药物。本研究通过分析儿童RMPP的炎症特点及糖皮质激素治疗后炎症因子的变化,旨在为早期诊断及合理治疗提供理论依据,现报道如下。
1 对象与方法
1.1 研究对象
选取2018年9月至2020年8月在浙江省人民医院儿科病区确诊的152例MP感染CAP住院患儿,根据诊断标准分为普通MPP(common mycoplasma pneumonia,GMPP)组(n=80)和难治性肺炎支原体肺炎(refractory mycoplasma pneumoniae pneumonia,RMPP)组(n=72)。
本研究经浙江省人民医院医学伦理委员会批准(批件编号2018KY059)。患儿纳入标准:①研究时期本科室收治、明确为MPP的住院患儿。以第7版《诸福棠实用儿科学》的肺炎诊断标准为依据。MP感染的诊断依据符合儿童肺炎支原体肺炎专家共识(2015版),应用大环内酯类抗生素1周或以上,患儿仍表现发热,临床症状和影像学表现继续加重者定义为RMPP[6]。②知情同意书由患儿本人及其监护人签署。
1.2 方法
RMPP组在注射用阿奇霉素(商品名:希舒美,规格:0.5 g,国药准字J20140073)10 mg/(kg·d)qd 7 d后,给予注射用甲基泼尼龙琥珀酸钠(商品名:甲强龙,规格:40 mg,国药准字H20170197)1 mg/(kg·次) q12h 3 d,部分患儿激素治疗3 d后体温仍不稳定,可再用甲强龙1 mg/(kg·次) qd 2 d。
1.3 观察指标
患儿于入院的当天采静脉血检测血清CRP、LDH、MP-IgM及细胞因子等。用无菌拭子取咽后壁分泌物,置于EP管中,RT-PCR检测MP-DNA。RMPP组在激素疗程结束、体温正常48 h后复查炎症指标和Mp-DNA水平。采用速率散射比浊法检测CRP,LDH用全自动生化仪测定,细胞因子检测采用ELISA法,试剂盒由美国B&D公司提供。RT-PCR法检测Mp-DNA,试剂盒由达安基因股份有限公司供应。
1.4 统计学方法
采用SPSS 23.0统计学软件进行统计分析。符合正态分布的计量资料以(x±s)表示,采用独立样本t检验;非正态分布的计量资料以中位数[M(P25,P75)]表示,采用非参数秩和检验。P<0.05为差异有统计学意义。将两组间存在明显差异的指标作为独立相关危险因素,通过ROC曲线对指标进行分析。
2 结果
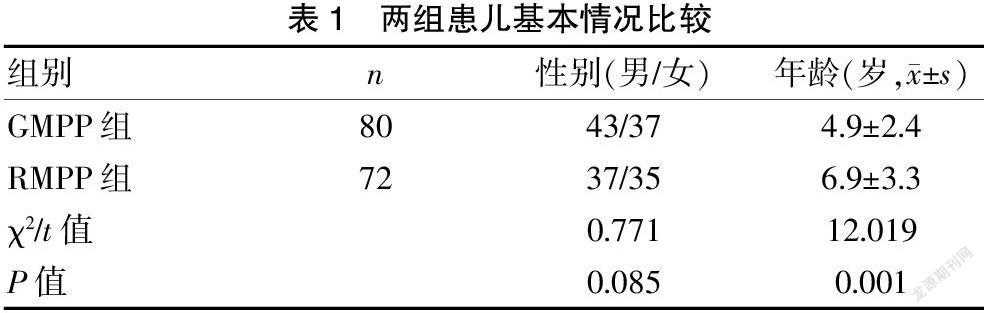
2.1 兩组患儿基本情况比较
两组的性别构成比比较,差异无统计学意义(P>0.05),但两组的年龄比较,RMPP组患儿年龄明显大于GMPP组患儿,差异有统计学意义(P<0.05)。见表1。
2.2 两组实验室指标比较
RMPP组CRP、LDH、IL-1β、IL-6、IL-8、IL-18和Mp-DNA水平明显高于GMPP组,差异有统计学意义(P<0.001);而IL-17在两组间比较,差异无统计学意义(P>0.05)。见表2。
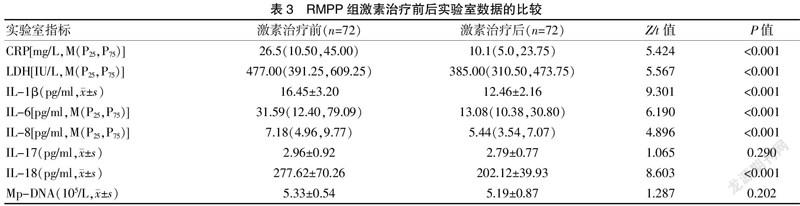
2.3 RMPP组激素治疗前后实验室指标比较
RMPP组激素治疗后,CRP、LDH、IL-1β、IL-6、IL-8及IL-18水平明显较激素治疗前下降,差异有统计学意义(P<0.001)。而IL-17和Mp-DNA在激素治疗前后比较,差异无统计学意义(P>0.05)。见表3。
2.4 各独立危险因素在RMPP患儿中的预测价值
ROC曲线分析显示,CRP、LDH、IL-1β、IL-6、IL-8及IL-18能较好地用于鉴别RMPP和GMPP患儿(P<0.05)。当CRP、LDH、IL-1β、IL-6、IL-8及IL-18的最佳阈值分别为12.75 mg/L、432.50 IU/L、13.42 pg/ml、13.28 pg/ml、5.55 pg/ml、227.50 pg/ml时,其预测RMPP发生的敏感度和特异度分别为73.6%和65.0%、63.9%和82.5%、83.3%和65.0%、73.6%和72.5%、72.2%和73.8%、79.2%和83.8%。见表4、封三图5。
3 讨论
近年来,随着儿童MPP发病率的上升,难治性病例明显增多[7]。目前尚不清楚RMPP的发病机制,但有学者认为,过强的炎症反应在RMPP的发生中起着重要的作用[8]。本研究结果显示,与GMPP组比较,RMPP组的年龄更大,可能与年长儿免疫系统相对成熟、免疫反应过强有关。
MPP时,免疫炎症反应对机体的损伤远大于MP引起的直接损伤。本研究结果显示,RMPP组患儿CRP水平明显高于GMPP组,提示RMPP可引起严重的免疫反应。同时,LDH水平在RMPP组也较GMPP组明显升高,原因可能为RMPP引起组织炎症损害,LDH从细胞内释放到血液中[9]。本研究结果还显示,RMPP组患儿的血清IL-1β、IL-6及IL-8水平明显高于GMPP组,与Miyashita等[10]的研究结果一致,即细胞因子水平越高,器官损伤和临床表现越严重。糖皮质激素可通过诱导促炎因子向抑炎因子转换,从而达到抑制炎症的作用[11]。本研究在全身使用甲基泼尼龙后,IL-1β、IL-6及IL-8水平均较治疗前明显下降,提示激素治疗可抑制机体的细胞免疫反应,减轻炎症损伤,从而缓解RMPP患儿的临床症状。
过度免疫炎症反应导致MPP病情加重,可能与NF-кB信号通路的激活有关,其中IL-17、IL-18作为上游调控因子,可以调控IL-6、IL-8,理论上可间接激活NF-кB信号通路[12-13],故推测可能与RMPP有关。但是,本研究结果显示,RMPP组与GMPP组外周血清中IL-17水平相比,无显著性差异,且激素治疗前后IL-17水平也无明显变化,提示IL-17与炎症反应严重程度无关,不宜作为预测RMPP的指标。其结果与Shao[14]的文献报道结果相同,但与Wang等[15]研究结果相悖。分析结论不一致的可能原因为IL-17是一种主要由单核细胞、CD4+记忆T细胞(Th17细胞)等分泌的促炎细胞因子,目前总共发现Th17细胞有6个家族成员,包括IL-17A~IL-17F。IL-17各个成员的角色不同,其各自功能也不相同。另外,IL-17家族属于调控因子,处于免疫机制上游,其影响因素更多[16]。所以,仅检测IL-17总体水平各研究结果差异较大,且不能真正反映RMPP的发病机制,需要进一步研究IL-17家族各个成员在RMPP中所起的作用。
IL-18是主要由單核-巨噬细胞分泌的一种前炎症细胞因子,属于IL-1家族。本研究结果显示,IL-18水平在RMPP组患儿血清中较GMPP组明显升高,提示IL-18是RMPP病情进展中一种重要的炎症细胞因子,可能作为预测RMPP的指标之一,这一结果与Miyashita等[17]研究一致。IL-18水平在RMPP患儿使用甲基泼尼龙后明显下降,提示静脉使用糖皮质激素可抑制IL-18在患儿体内的产生及释放,进一步降低组织中IL-18的浓度,证明糖皮质激素可通过抑制细胞因子从而起到治疗RMPP的作用,该结果也进一步证实IL-18参与了RMPP的发病机制。
Mp-DNA的水平反映了宿主免疫清除能力与MP感染之间的平衡[18]。本研究结果显示,RMPP患儿的Mp-DNA复制倍数显著高于GMPP患儿,这一结果与Liu等[19]研究一致,提示高水平的Mp-DNA可能是RMPP患儿过度免疫反应的诱发因素之一。但全身糖皮质激素治疗前后,Mp-DNA水平虽有所下降,但差异无统计学意义(P>0.05)。其机制可能与支原体耐药现象增加,通过P1蛋白粘附呼吸道黏膜上皮细胞的逃避机制,以及RMPP患儿存在不同程度的纤毛功能受损、清除病原菌的作用下降等有关[20]。
本研究结果显示,RMPP的独立危险因素包括CRP、LDH、IL-1β、IL-6、IL-8及IL-18,这些因子的分泌越多,免疫反应越强,患儿发生RMPP的风险就越高。分析ROC曲线发现,当血清CRP、LDH、IL-1β、IL-6、IL-8及IL-18的最佳阈值分别为12.75 mg/L、432.50 IU/L、13.42 pg/ml、13.28 pg/ml、5.55 pg/ml、227.50 pg/ml时,预测RMPP发生的敏感度和特异度分别为73.6%和65.0%、63.9%和82.5%、83.3%和65.0%、73.6%和72.5%、72.2%和73.8%、79.2%和83.8%。上述指标曲线下面积均大于0.7,对RMPP患儿的早期诊断具有重要价值。其中,IL-18的曲线下面积为0.845,显示出最佳的判别能力,今后可作为预测RMPP的指标之一。
综上所述,RMPP的发病可能有多种免疫机制共同参与,提高对RMPP的早期识别能力非常重要,对于持续发热伴CRP、LDH、IL-1β、IL-6、IL-8及IL-18水平明显升高,且伴有高水平Mp-DNA的患儿,当大环内酯类抗生素治疗效果不佳时,则应考虑RMPP的可能。及时使用全身糖皮质激素的治疗,可以抑制机体的细胞免疫反应,从而缓解RMPP患儿的临床症状,减少肺部并发症的发生。
[参考文献]
[1] Arnold FW,Summersgill JT,Ramirez JA. Role of atypical pathogens in the etiology of community-acquired pneu- monia[J].Semin Respir Crit Care Med,2016,37(6):819-828.
[2] Kapur N,Grimwood K,Masters IB,et al. Lower airway microbiology and cellularity in children with newly diagnosed non-CF bronchiectasis[J].Pediatr Pulmonol,2012,47(3):300-307.
[3] Wang Y,Xu D,Li S,et al. Mycoplasma pneumoniae-associated necrotizing pneumonitis in children[J].Pediatr Int,2012,54(2):293-297.
[4] Narita M. Classification of extrapulmonary manifestations due to Mycoplasma pneumoniae infection on the basis of possible pathogenesis[J]. Front Microbiol,2016,7:23.
[5] Zhang Y,Zhou Y,Li S,et al. The clinical characteristics and predictors of refractory Mycoplasma pneumoniae pneumonia in children[J]. PLoS One,2016,11(5):e0156 465.
[6] 陳志敏,尚云晓,赵顺英,等.儿童肺炎支原体肺炎诊治专家共识(2015年版)[J].中华实用儿科临床杂志,2015,30(17):1304-1308.
[7] Narita M. Classification of extrapulmonary manifestations due to Mycoplasma pneumoniae infection on the basis of possible pathogenesis[J]. Front Microbiol,2016,7:23.
[8] Waites KB,Xiao L,Liu Y,et al. Mycoplasma pneumoniae from the respiratory tract and beyond[J]. Clin Microbiol Rev,2017,30(3):747-809.
[9] Lu A,Wang C,Zhang X,et al. Lactate dehydrogenaseas a biomarker for prediction of refractory Mycoplasma pneumoniae pneumonia in children[J].Respir Care,2015, 60(10):1469-1475.
[10] Miyashita N,Narita M,Tanaka T,et al. Histological find- ings in severe Mycoplasma pneumoniae pneumonia[J].J Med Microbiol,2017,66(5):690-692.
[11] Strehl C,Buttgereit F. Optimized glucocorticoid therapy:Teaching old drugs new tricks[J].Mol Cell Endocrinol,2013,380(1-2):32-40.
[12] Fan H,Lu B,Yang D,et al. Distribution and expression of IL-17 and related cytokines in children with Mycop- lasma pneumoniae pneumonia[J].Jpn J Infect Dis,2019, 72(6):387-393.
[13] Narita M,Tanaka H. Late increase of interleukin-18 levels in blood during Mycoplasma pneumoniae pneum- onia[J].Cytokine,2012,59(1):18-19.
[14] Shao L,Cong Z,Li X,et al. Changes in levels of IL-9,IL-17,IFN-γ,dendritic cell numbers and TLR expres- sion in peripheral blood in asthmatic children with Mycop- lasma pneumoniae infection[J].Int J Clin Exp Pathol,2015,8(5):5263-5272.
[15] Wang Z,Sun J,Liu Y,et al. Impact of atopy on the severity and extrapulmonary manifestations of childhood Mycop- lasma pneumoniae pneumonia[J].J Clin Lab Anal,2019, 33(5):e22 887.
[16] McGeachy MJ,Cua DJ,Gaffen SL. The IL-17 family of cytokines in health and disease[J].Immunity,2019,50(4):892-906.
[17] Miyashita N,Kawai Y,Inamura N,et al. Setting a standard for the initiation of steroid therapy in refractory or severe Mycoplasma pneumoniae pneumonia in adolescents and adults[J].Infect Chemother,2015(21):153-160.
[18] Dumke R,Jacobs E. Evaluation of five real-time PCR assays for detection of Mycoplasma pneumoniae[J]. J Clin Microbiol,2014,52(11):4078-4081.
[19] Liu J,Zhao F,Lu J,et al. High Mycoplasma pneumoniae loads and persistent long-term Mycoplasma pneumoniae DNA in lower airway associated with severity of pediatric Mycoplasma pneumoniae pneumonia[J]. BMC Infect Dis,2019,19(1):1045.
[20] Spuesens EB,Meyer Sauteur PM,Vink C,et al. Myco- plasma pneumoniae infections-Does treatment help[J]. Journal of Infection,2014,69(Suppl 1):S42-S46.
(收稿日期:2021-03-22)
猜你喜欢
中老年保健(2021年5期)2021-08-24 07:06:38
中老年保健(2021年6期)2021-08-24 06:53:48
中老年保健(2021年11期)2021-08-22 03:14:10
中华养生保健(2020年3期)2020-11-16 00:53:14
中国实用医药(2016年28期)2016-12-07 07:22:22
中外医学研究(2016年28期)2016-11-28 07:11:06
今日健康(2016年12期)2016-11-17 12:05:02
中国实用医药(2016年24期)2016-10-17 04:39:28
中国实用医药(2016年13期)2016-07-05 04:14:34
饮食与健康·下旬刊(2016年7期)2016-05-10 12:45:11
