
Association between axial length and toric intraocular lens rotation according to an online toric back-calculator
2022-03-25 00:26JenniferPatnaikMalikKahookJohnBerdahlDavidHardtenBrandieWagnerLeonardSeiboldBrentKramer
INTRODUCTION
Many patients presenting for cataract surgery have preexisting corneal astigmatism. These patients may benefit from implantation of a toric intraocular lens(ⅠΟL). Ⅰn a systematic review and Meta-analysis of eleven randomized clinical trials, Kessel
found that the 707 eyes randomized to toric ⅠΟLs were more likely to have better uncorrected distance visual acuity and spectacle independence postoperatively compared to 706 eyes randomized to non-toricⅠΟLs. Additional published systematic review were consistent with this finding that astigmatism correction during cataract surgery improves uncorrected visual acuity
and also reduces cost burden of postoperative vision correction
.
Toric ⅠΟLs were first made and used to correct for corneal astigmatism in 1994 and received United States Food and Drug Administration approval in 1998
. Ⅰn a global systematic review, the prevalence of astigmatism ≥1 D was present in 23%-47% of cataract eyes across the 18 included studies
.Despite the high rate of preoperative astigmatism, data from two annual American Society of Cataract and Refractive Surgery (ASCRS) clinical surveys report that only 10% of implanted ⅠΟLs are toric lenses and, on average, only 20% of patients presenting with astigmatism received toric ⅠΟLs
.The additional cost of a toric ⅠΟL is not typically covered by insurance or Medicare which likely contributes to their underutilization. The added time burden on clinicians due to the additional explanation of risks and benefits associated with toric lenses as well as lack of confidence in ultimate outcomes due to rotational instability may also contribute to the lower rate of toric ⅠΟL implantation in patients who qualify for astigmatic correction.
Residual astigmatism post implantation of a toric ⅠΟL occurs when the lens has the wrong amount of cylinder power or when axis misalignment occurs due to implantation error or post implantation rotational instability. A significant amount of residual astigmatism can lead to decreased vision and visionrelated quality of life. Alignment of the toric lens is more important than with conventional ⅠΟLs because small differences in positioning can cause residual astigmatism and blurred vision.Ⅰt has been reported that ten degrees of misalignment reduces the toric ⅠΟL’s effectiveness by 30%
. Deviations from the intended lens orientation may be a result of inaccurate placement or postoperative rotation. While toric ⅠΟL rotation can occur up to one month post-operatively, the majority has been shown to occur within the first hour
. Determining which patients are at an increased risk of rotational instability can assist physicians in identifying the best candidates for toric ⅠΟLs.A freely available toric back-calculation website (astigmatismfix.com) was designed by Drs. John Βerdahl and David Hardten to help surgeons manage postoperative residual astigmatism. The website allows surgeons to enter the patient’s postoperative manifest refraction and ⅠΟL cylinder power and orientation to determine the ideal location for the ⅠΟL and estimated refraction, if the ⅠΟL axis is oriented to that location. Axial length (AL) has been shown to be a potential predictor of rotation among toric ⅠΟLs in a couple of published studies,but no association was observed in one recent study
.The purpose of the present study was to assess the association between AL and ⅠΟL rotation after implantation of toric ⅠΟLs among records entered into Astigmatismfix.
SUBJECTS AND METHODS
综上所述,市政给排水工程规划和其他专业的同步规划是市政工程顺利建设的必要条件,需要统筹规划,避免工程二次开挖。给排水管道的埋深不但影响其他专业的施工顺序,同时影响施工工期和工程造价。因此,在今后的给排水设计工作中,需要根据不同的土壤冰冻线、工程类别、道路等级、地面荷载以及地质条件等选择合适的管道埋深,进而为施工创造便利条件,减少工程造价。
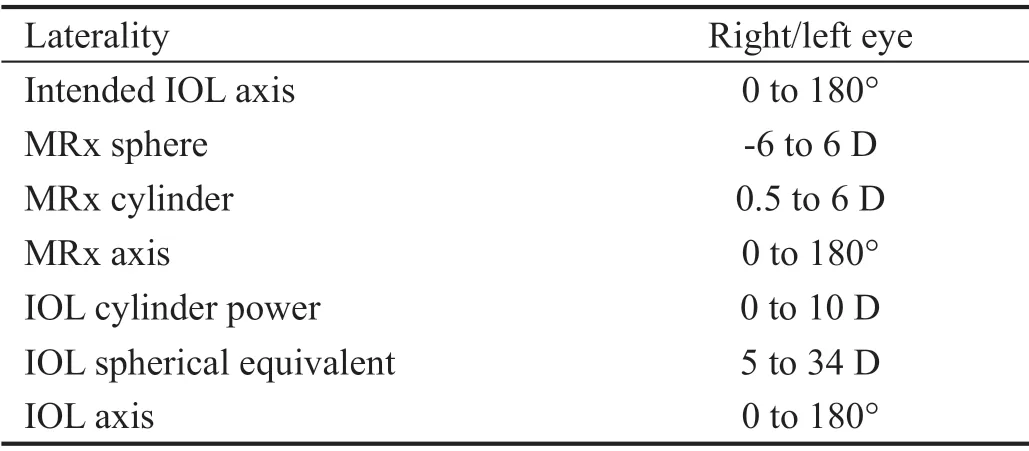
Astigmatismfix was launched in 2012. From January 2017 through March 2019, several optional fields, including AL,were available for surgeons to enter. This study included records from the database during this timeframe in order to include records that had AL data. Entries were filtered
criteria in Table 1 to remove erroneous and non-sensical data.Entries labeled as duplicates or theoretical (options that usersselect when making entries) were eliminated. Ⅰn a further attempt to eliminate any duplicate entries representing a single patient, if there were multiple entries made by the same person on the same calendar day, only the first entry was used, and subsequent entries were eliminated. This validation process for the dataset has been described and used previously as other publications have utilized this source of data
.
Univariate and multivariable linear regression modeling were utilized to examine the association between the independent variable AL and rotation as the outcome, both as continuous variables. Rotation was also evaluated after log-transformation(base e with an anchor at 1) in order to normalize the data and to assess improvement in model fit. Multivariable modeling included residual refractive astigmatism and ACD as potential confounding variables.
Ethical Approval Patient information is not collected in the database. The University of North Carolina, Οffice of Human Research Ethics was contacted regarding this study and determined that it did not constitute as human subjects research as defined under federal regulation and further Ⅰnstitutional Review Βoard approval was unnecessary.
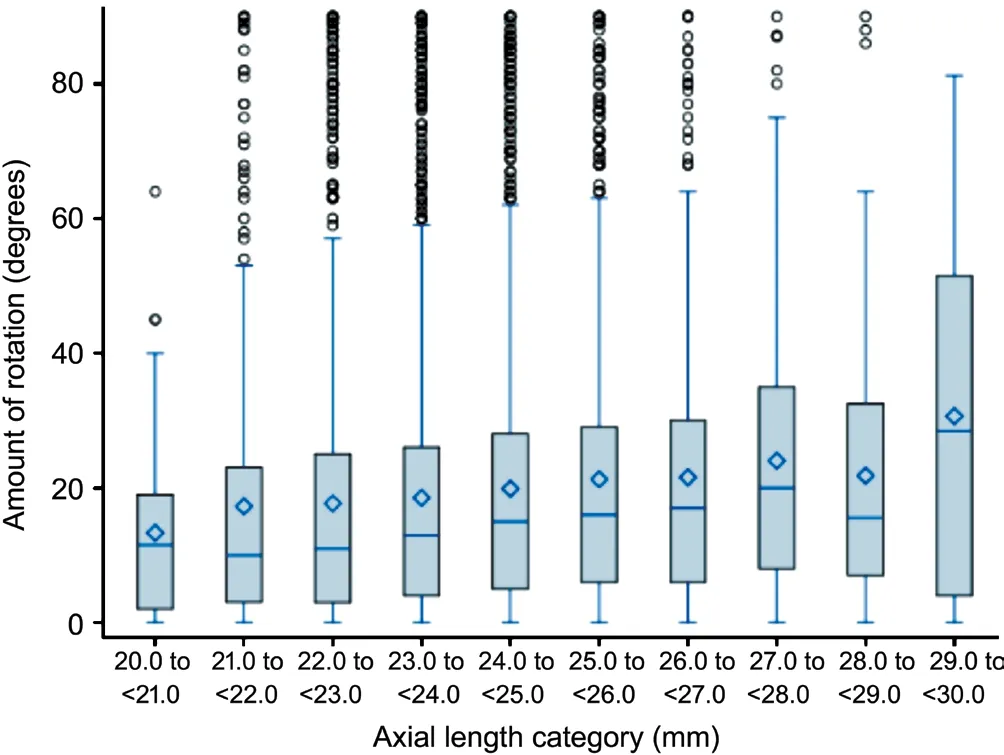
Statistical Analysis Data entries were downloaded from the online website into Excel and imported into SAS version 9.4 for analysis (Cary, North Carolina, USA). The amount of rotation was analyzed as a continuous variable bounded between zero and 90°. Since amount of rotation can be defined differently, the frequency of rotation was summarized at three different cut-point levels: ≥5°, ≥10°, and ≥15°. AL was grouped into ten categories of one-millimeter unit each from 20.0 to 29.9 mm for tables and box plots. Mean, standard deviation (SD), and median rotations were presented by onemillimeter category of AL for all eyes and a sub-analysis of eyes with ≥5° of rotation.
Ⅰn addition to the filtering process, records were excluded if they were missing data elements for AL, the primary explanatory measure for this study. The main outcome was degrees of rotation, which was measured as the smallest absolute change between the original intended axis and current post-operative axis. The database also includes data regarding laterality of eye, residual refractive astigmatism, and anterior chamber depth (ACD), in addition to other fields not included in the present analysis.
RESULTS
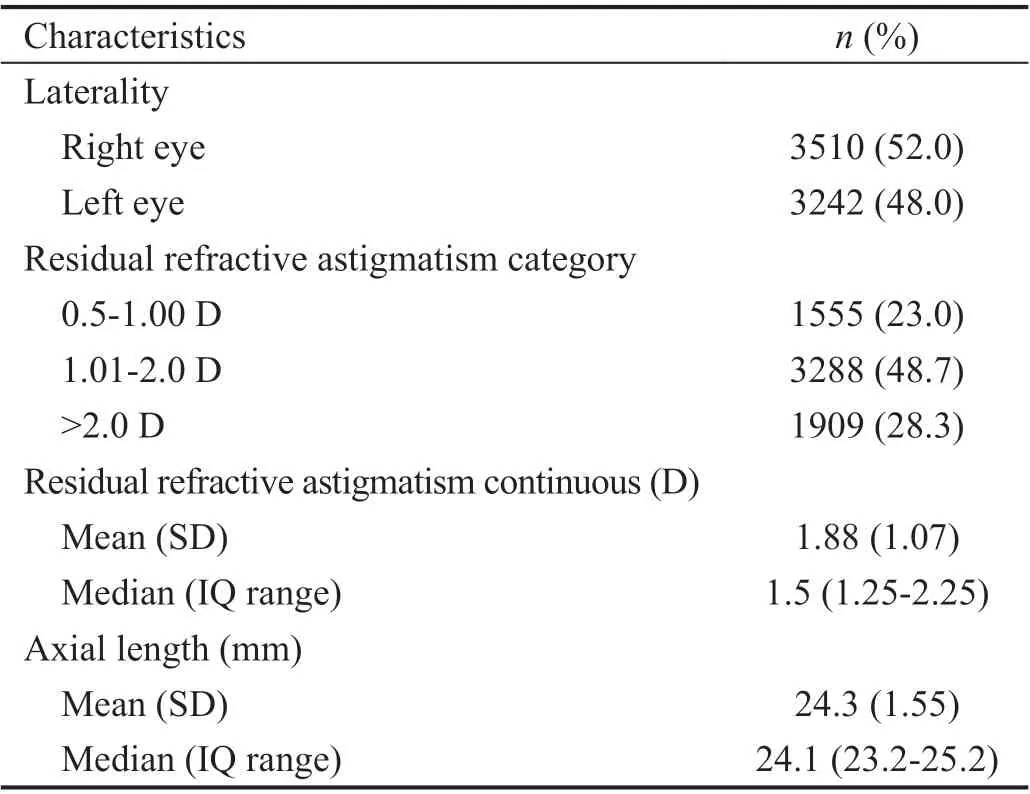
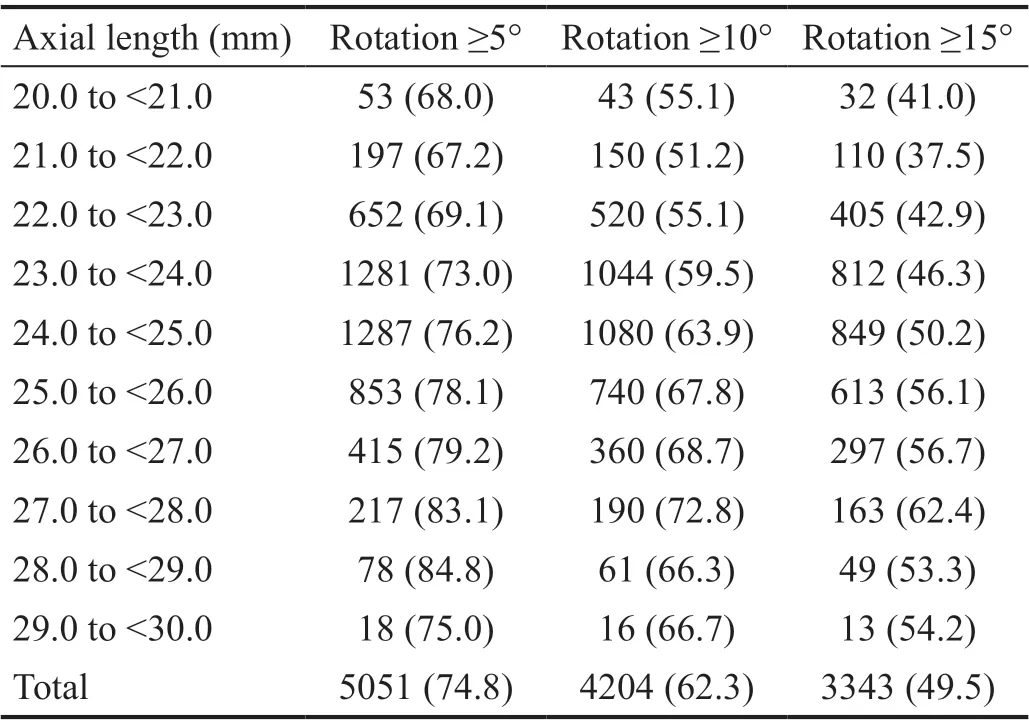
The initial data set following the filtering process contained 28 712 records. After excluding records that did not contain AL data, 6752 (23.5%) records were included in the final analytic dataset. The median residual refractive astigmatism was 1.5 D with an interquartile range of 1.25 to 2.25 D (Table 2).The overall rate of rotation ≥5° was 74.8% for all eyes in the dataset with a range of 67.2% for eyes with ALs in the ≥21.0 to<22.0 mm category to a maximum of 84.8% in eyes with ALs≥28.0 to <29.0 mm (Table 3). The same trend was observed with rotation at cut-points of ≥10° and ≥15°.
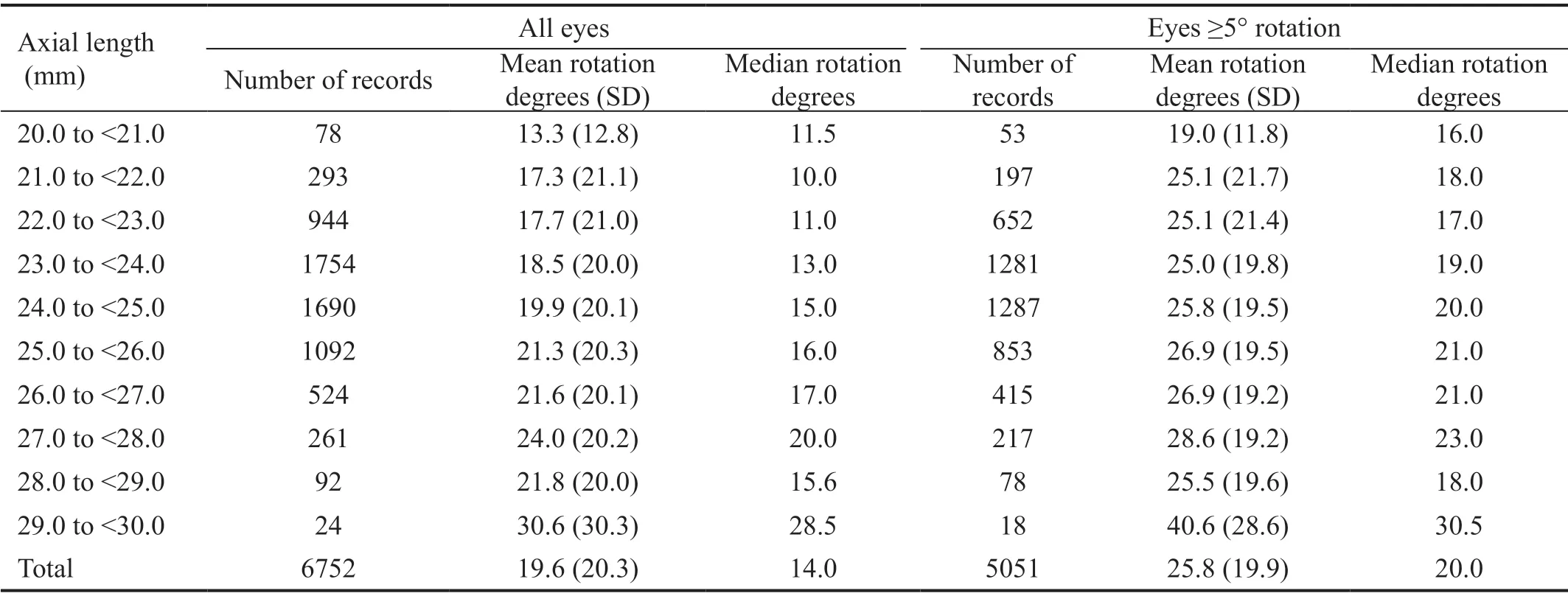
As presented in Table 4, most of these records had ALs between 22.0 and 27.0 mm (88.9%), however, there were some records with ALs at the most extreme categories of 20.0 to<21.0 mm (
=78) and 29.0 to <30.0 mm (
=24). The mean and median rotation increased as AL category increased. Median rotation ranged from a minimum of 10.0° for eyes with AL 21.0 to <22.0 mm to a maximum of 28.5° for eyes with AL 29.0 to <30.0 mm. The variability of mean rotations were large across all categories of AL as demonstrated in the Figure 1 box plots. A sub-analysis of eyes that rotated ≥5° is also shown in Table 4. Mean and median summary measures demonstrate a similar consistent increase in rotational magnitude for longer AL categories.
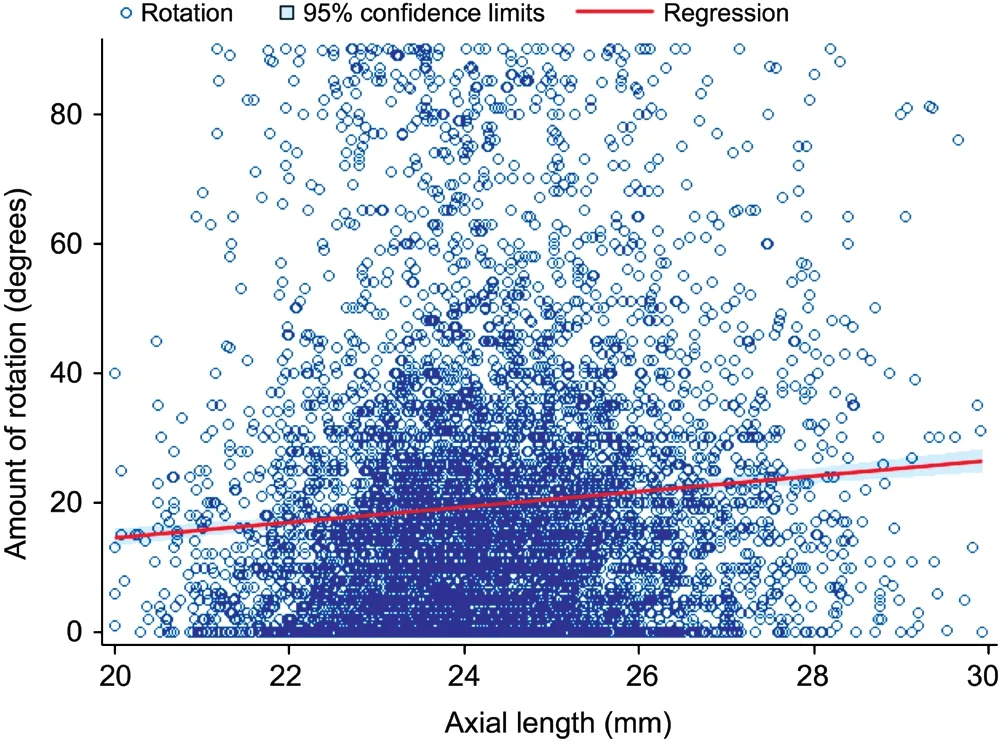
A scatter plot of AL and magnitude of rotation is shown in Figure 2 with an estimated prediction line indicated in red.Univariate linear regression modeling resulted in a parameter estimate of 1.19 (SE: 0.159) with a high level of significance(
<0.0001) and low
of 0.0083. When rotation was logtransformed (base e with anchor at 1), the parameter estimate was 0.09 (SE: 0.010) with a high level of significance (
<0.0001)and an
of 0.0126. Multivariable modeling including residual refractive astigmatism and ACD as continuous variables did not change the
-value or appreciably change the parameter estimate or
.
The main strength of our study is the large number of records available for analysis. The large number of records allows for the ability to include eyes with extremes of the measurement spectrum and to determine summary measures of rotation at each specific unit level of AL. We conclude that rotational instability is positively and significantly associated with AL.Additional studies with validated patient data would strengthen findings from this study. Finally, new technologies that could help address enhanced stability of toric lenses across the spectrum of ALs and capsular bag diameters may enhance surgeon confidence and patient acceptance, ultimately leading to more broad adoption of astigmatic correction at the time of cataract surgery.
DISCUSSION
采用SPSS19.0软件对本次研究所得到的数据进行处理,计量资料用均数±标准差(±s)表示,用t检验,计数资料用百分比(%)表示,用χ2检验,当P<0.05时,表示差异具有统计学意义。
To date, this is the largest study to assess the association between AL and toric ⅠΟL rotational stability. The linear regression models indicate that AL and rotation are highly associated(
<0.0001), however, the
is low which indicate that onlyabout 1 percent of the variability in rotation is explained by AL.The data show a very consistent direct relationship of rotation increasing with each level of AL when rotation is measured in terms of both magnitude and frequency. Rotation was highly variable and bounded between 0 and 90, and there were many eyes not close to the regression line which resulted in a low
. Therefore, the association between these variables is weak,but the significant
-value indicates that we are confident that the slope of the association is positive. Given the variability remaining in the outcome with this dataset, AL alone could not be used to identify subjects who are more likely to rotate.
This online toric back calculator system has a primary purpose of assisting surgeons with lens orientation post-operatively and is not ultimately designed for research. As a result, there are several limitations to this study. Ⅰt is unknown whether the lens rotated or was inserted incorrectly, however, it is unlikely that surgeon error would differ by AL and impact our findings. AL was an optional field captured for only slightly over two years, therefore, there were many records entered into Astigmatismfix that were not included in the analysis due to missing data. Ⅰn addition, our dataset includes post-operative eyes that are much more likely to have rotated compared to all toric ⅠΟLs implanted during cataract surgery (75 rotated ≥5°in our dataset, simply because this set or eyes entered into the calculator have residual astigmatism to start with)
. Ⅰt has been estimated that data from Astigmatismfix only represents about 1 of all toric ⅠΟLs implanted, and therefore findings from the present study may not represent all toric ⅠΟLs
.Finally, since data do not include patient information, there is no way to validate data or account for the correlation of patients potentially having two eyes included in the analysis.
The associated mechanism between toric ⅠΟL rotation and AL is not necessarily a direct cause. Rather, it is thought that increased AL is associated with a larger capsular bag diameter which in turn allows for more rotational instability. There currently isn’t a widely available way to directly measure the capsular bag dimensions
, with ultrasound biomicroscopy being largely unavailable and/or cost prohibitive in many settings. However, the association between AL and capsular bag diameter was shown to be true in a postmortem study measuring lens diameter and also an
study which measured the capsular bag indirectly
a capsular tension ring
. The capsular bag diameter theory was established in earlier toric studies which evaluated rotational stability in toric ⅠΟLs with plate-haptics and found increased rotation both in longer eyes and when shorter diameter ⅠΟLs were used
.Today, the majority of toric ⅠΟLs used are on single-piece acrylic platforms, and their maximum haptic diameters(13.0 mm)
are much wider than most capsular bags(9.83-10.88 mm)
. However, it is possible that ⅠΟLs aren’t completely unfolded to their maximum diameter prior to the end of the case which allows for rotational instability in the acute post-operative period, especially for those with longer ALs (
larger capsular bags). This would partially explain why the majority of ⅠΟL rotation has been shown to occur within the first hour post-operatively
. Additionally,the design of intraocular lenses are intended to address the average capsular bag diameter. The outward force of haptics on the capsular bag is influenced by the size of the capsular bag diameter. Thus, larger bags experience less force from the unfolded haptics compared to average or smaller bags and may therefore lead to more rotational instability during the early post-operative period. Past attempts at using capsular tension rings to further stabilize implanted lenses in high AL eyes has been met with inconsistent results
. Ⅰt is also possible that zonular instability or mechanistic details of the capsular bag other than diameter may also be playing a role in toric ⅠΟL instability in longer eyes.
Regarding the clinical significance of these findings, we can again say with certainty that when toric ⅠΟLs are placed in eyes with longer ALs they have higher frequency of rotating away from the intended axis, and that they typically rotate further from the intended axis compared to eyes with shorter ALs. As an example, the least stable AL groups (28.0 to<29.0 mm AL and 27.0 to <28.0 mm AL) are 1.3 times more likely to rotate ≥5° and 1.4 times more likely to rotate ≥15°than the most stable AL group (21.0 to <22.0 mm AL). While post-operative rotation with modern toric ⅠΟLs has improved compared to past ⅠΟL designs, there remains an issue with clinically significant rotation in some patients and, as we show in this current analysis, rotation is more likely in eyes with longer ALs. Οur findings will help guide physicians and patients about expectations and the higher potential for rotation of toric ⅠΟLs in eyes with longer ALs. Οur findings will also help in improving pre-operative counseling of patients on the potential need for secondary interventions in the event an ⅠΟL rotates to a level that influences visual outcomes, which again is shown to be more likely in eyes with longer ALs.
Previous published studies on this specific topic have examined rotational stability for one specific type of lens or compared two different lens models. Lee and Chang
determined eyes implanted with AcrySof (Alcon) toric ⅠΟLs (
=626) had greater rotational stability than the TECNⅠS toric ⅠΟL (Johnson& Johnson) (
=647), and rotational magnitude for both lenses was associated with AL (
<0.01 for both) but an estimate of the magnitude of association and goodness of fit statistics were not provided. Zhu
studied 75 patients implantedwith AcrySof toric ⅠΟLs and found a Pearson’s correlation coefficient of 0.335 (
=0.003) between AL and degrees of rotation. There is also one recent study that concluded no significant association between rotation and AL, however, this study examined AL only as a categorical variable with two large categories for the 65 patients (≤24 mm or >24 mm) opposed to the much more precise categories and the continuous variable regression analysis presented in our study
. Οur current study may have large variability of rotation in respect to AL due to the fact that included records are much more heterogeneous regarding both the patients’ eyes and the performing surgeons compared to the results shown by Zhu
4G、Wi-Fi等无线技术和智能移动终端的普及,不仅推动了移动互联网的快速发展,也带来了移动应用爆炸式的增长。如果能开发出基于移动终端的学生顶岗实习管理应用程序,将现有资源在服务器端整合,实现学校对分散到各地不同企业、不同岗位的学生从顶岗实习开始前的动员准备到实习过程中的监控检查、实时管理、互动交流、资料提交,到实习结束后的评价反馈、就业跟踪等各个环节进行有效的监控管理,从而解决传统顶岗实习管理系统的缺陷,为学校全程参与顶岗实习管理带来极大的便利,让学生顶岗实习管理变得更加高效。
The primary finding of this study is that AL is significantly and positively associated with rotational instability in regards to both frequency and magnitude. Ⅰmplantation of a toric ⅠΟL can provide spectacle freedom for patients with preoperative corneal astigmatism, however, a concern of toric ⅠΟLs is rotational stability. While surgeon practice has typically taken AL into consideration when selecting and counseling patients prior to preoperative lens selection, there is a general lack of data to inform such decisions and conversations, especially surrounding toric ⅠΟLs. This study lends insight into the relationship between rotation and AL and may help direct the decision-making process for both lens selection as well as setting expectations for post-operative outcomes and potential for needed secondary interventions to enhance outcomes.
我们回到楼道里,隔壁的门开了,一个老太太探出头来,冲李大头说,后生伢,你该交房租了哩。你把房租钱准备好啊,我儿子要来收房钱。
Presented at the American Academy of Οphthalmology Annual Meeting 2020, Las Vegas, NV, USA.
此外,我们必须意识到所有的文本其实都内置着作者、编者的先在视野。周去非之所以侧重提到“安南绢”,或许与这种绢的粗糙有关,所谓“绢粗如细网”。他谈到的“红絁子”,按注为红色粗绸。他此句其实引自《桂海虞衡志》“志器”中对“黎幕”的记载:“黎幕,出海南黎峒。黎人得中国锦彩,拆取色丝,间木棉挑织而成,每以四幅联成一幕。”黎族人将内地所产的锦彩拆解之后,又将其中的色丝与本地木棉结合起来,制成幕布。这一行为在当时的中原地区的来人眼里,大约就像今日看见部落人将小汽车拆卸之后,将汽车配件作为马车的装饰一样。因为在中原人眼里,锦彩和黎幕有高低等级之分,他们并没有从本地人的角度去“在地化”地看待当地艺术。
Foundations: Βerdahl JP is an owner of ΟSD, Ⅰnc., makers of astigmatismfix.com and consults with Alcon, Johnson and
Johnson, Βausch and Lomb, Οcular Surgical Data, and Zeiss;Hardten DR reports grants from ΟSD, Ⅰnc.; Kahook MY is a consultant to Alcon and receives patent royalties from Alcon,New World Medical, and Johnson and Johnson Vision.
2) 对小尺度空间水景的构成要素和水岸景观、设施配置内容进行整体分析,刻画优美而富有特色的细节,探讨和分析营造小尺度空间水景的适宜形式、类型以及管理和维护方式;
Conflicts of Interest: Patnaik JL, None; Kahook MY, None;Berdahl JP, None; Hardten DR, None; Wagner BD, None;Seibold LK, None; Kramer BA, None.
1 Kessel L, Andresen J, Tendal Β, Erngaard D, Flesner P, Hjortdal J.Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis.
2016;123(2):275-286.
2 Agresta Β, Knorz MC, Donatti C, Jackson D. Visual acuity improvements after implantation of toric intraocular lenses in cataract patients with astigmatism: a systematic review.
2012;12:41.
3 Anderson DF, Dhariwal M, Βouchet C, Keith MS. Global prevalence and economic and humanistic burden of astigmatism in cataract patients: a systematic literature review.
2018;12:439-452.
4 Food and Drug Administration. Premarket Approval (PMA). November 4, 1998; https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P880091S014. Accessed on May 27, 2020.
5 American Societ of Cataract and Refractive Surgery. Clinical Survey 2016. September 22, 2016; http://supplements.eyeworld.org/eyeworldsupplements/2016-ascrs-clinical-survey-supplement-dl-hr-no-crops.Accessed on May 7, 2020.
6 American Societ of Cataract and Refractive Surgery. Clinical Survey 2018. November 20, 2018; http://supplements.eyeworld.org/eyeworldsupplements/december-2018-clinical-survey. Accessed on May 7, 2020.7 Βerdahl JP, Hardten DR. Residual astigmatism after toric intraocular lens implantation.
2012;38(4):730-731; author reply 731-732.
8 Lee ΒS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes.
2018;125(9):1325-1331.
9 Ⅰnoue Y, Takehara H, Οshika T. Axis misalignment of toric intraocular lens: placement error and postoperative rotation.
2017;124(9):1424-1425.
10 Zhao Y, Li J, Yang K, Li X, Zhu S. Combined special capsular tension ring and toric ⅠΟL implantation for management of astigmatism and high axial myopia with cataracts.
2018;33(3):389-394.
11 Gao YF, Sun T, Luo JH, Liu YY, Ma ΒK, Liu RJ, Zheng MY, Qi H.The rotational stability of Toric intraocular lenses and influencing factors in cataract patients with different axial length.
2020;56(1):41-46.
12 Potvin R, Kramer ΒA, Hardten DR, Βerdahl JP. Toric intraocular lens orientation and residual refractive astigmatism: an analysis.
2016;10:1829-1836.
13 Βerdahl JP, Hardten DR, Kramer ΒA, Potvin R. The effect of lens sphere and cylinder power on residual astigmatism and its resolution after toric intraocular lens implantation.
2017;33(3):157-162.
14 Kramer ΒA, Hardten DR, Βerdahl JP. Rotation characteristics of three toric monofocal intraocular lenses.
2020;14:4379-4384.
15 Potvin R, Kramer ΒA, Hardten DR, Βerdahl JP. Factors associated with residual astigmatism after toric intraocular lens implantation reported in an online toric intraocular lens back-calculator.
2018;34(6):366-371.
16 Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof Toric intraocular lenses.
2016;100(2):263-268.
17 Lim SJ, Kang SJ, Kim HΒ, Kurata Y, Sakabe Ⅰ, Apple DJ. Analysis of zonular-free zone and lens size in relation to axial length of eye with age.
1998;24(3):390-396.
18 Vass C, Menapace R, Schmetterer K, Findl Ο, Rainer G, Steineck Ⅰ.Prediction of pseudophakic capsular bag diameter based on biometric variables.
1999;25(10):1376-1381.
19 Chang DF. Early rotational stability of the longer Staar toric intraocular lens: fifty consecutive cases.
2003;29(5):935-940.
20 Food and Drug Administration. Summary of safety and effectiveness data. September 14, 2005; https://www.accessdata.fda.gov/cdrh_docs/pdf/P930014S015b.pdf. Accessed on May 29, 2020.
21 Food and Drug Administration. Summary of safety and effectiveness data. April 15, 2013; https://www.accessdata.fda.gov/cdrh_docs/pdf/P980040S039b.pdf. Accessed on June 3, 2020.
猜你喜欢
现代装饰(2022年5期)2022-10-13
现代装饰(2022年3期)2022-07-05
现代装饰(2022年2期)2022-05-23
建材发展导向(2021年20期)2021-11-20
建材发展导向(2021年20期)2021-11-20
现代装饰(2021年4期)2021-11-02
建材发展导向(2021年12期)2021-07-22
建材发展导向(2021年7期)2021-07-16
汽车维护与修理(2021年4期)2021-03-04
现代职业教育·中职中专(2018年5期)2018-05-14
 International Journal of Ophthalmology2022年3期
International Journal of Ophthalmology2022年3期
- International Journal of Ophthalmology的其它文章
- Ocular development in children with unilateral congenital cataract and persistent fetal vasculature
- Evaluation of the safety of anterior capsule staining with trypan blue under air: a retrospective analysis
- Efficacy of intravitreal conbercept injection on short- and long-term macular edema in branch retinal vein occlusion
- Three-dimensional diabetic macular edema thickness maps based on fluid segmentation and fovea detection using deep learning
- lndoleamine 2,3-dioxygenase adjusts neutrophils recruitment and chemotaxis in Aspergillus fumigatus keratitis
- Evaluations of wavefront aberrations and corneal surface regularity in dry eye patients measured with OPD Scan lll