
Application of robotic technologies in lower gastrointestinal tract endoscopy: A systematic review
2022-01-04 09:44:04HarpreetKaurSekhonInderjitSinghEmilyRoseArmstrongSujayShahRezaMirnezami
Harpreet Kaur Sekhon Inderjit Singh, Emily Rose Armstrong, Sujay Shah, Reza Mirnezami
Harpreet Kaur Sekhon Inderjit Singh, Emily Rose Armstrong, Sujay Shah, Reza Mirnezami, Colorectal Surgery, The Royal Free Hospital, London NW3 2QG, Hampstead, United Kingdom
Abstract BACKGROUND Conventional optical colonoscopy is considered the gold standard investigation for colorectal tract pathology including colorectal malignancy, polyps and inflammatory bowel disease.Inherent limitations exist with current generation endoscopic technologies, including, but not limited to, patient discomfort, endoscopist fatigue, narrow field of view and missed pathology behind colonic folds.Rapid developments in medical robotics have led to the emergence of a variety of next-generation robotically-augmented technologies that could overcome these limitations.AIM To provide a comprehensive summary of recent developments in the application of robotics in lower gastrointestinal tract endoscopy.METHODS A systematic review of the literature was performed from January 1, 2000 to the January 7, 2021 using EMBASE, MEDLINE and Cochrane databases.Studies reporting data on the use of robotic technology in ex vivo or in vivo animal and human experiments were included.In vitro studies (studies using synthetic colon models), studies evaluating non-robotic technology, robotic technology aimed at the upper gastrointestinal tract or paediatric endoscopy were excluded.System ergonomics, safety, visualisation, and diagnostic/therapeutic capabilities were assessed.RESULTS Initial literature searching identified 814 potentially eligible studies, from which 37 were deemed suitable for inclusion.Included studies were classified according to the actuation modality of the robotic device(s) as electromechanical (EM) (n = 13), pneumatic (n = 11), hydraulic (n = 1), magnetic (n = 10) and hybrid (n = 2) mechanisms.Five devices have been approved by the Food and Drug Administration, however most of the technologies reviewed remain in the early phases of testing and development.Level 1 evidence is lacking at present, but early reports suggest that these technologies may be associated with improved pain and safety.The reviewed devices appear to be ergonomically capable and efficient though to date no reports have convincingly shown diagnostic or therapeutic superiority over conventional colonoscopy.CONCLUSION Significant progress in robotic colonoscopy has been made over the last couple of decades.Improvements in design together with the integration of semiautonomous and autonomous systems over the next decade will potentially result in robotic colonoscopy becoming more commonplace.
Key Words: Robotics; Colonoscopy; Endoscopy; Automation; Actuation; Propulsion
INTRODUCTION
Conventional optical colonoscopy represents the gold standard investigation for lower gastrointestinal (LGI) tract pathology including colorectal cancer (CRC), polyps and inflammatory bowel disease[1].Current generation colonoscopes consist of a semirigid flexible scope containing fibre optic bundles with a camera at the distal end allowing visualisation of the colonic lumen.The scope tip can be manoeuvred in two directionsviatwin-wheels located on the control shaft of the scope, where buttons controlling air insufflation, suction and irrigation mechanisms are also located.Passage of instruments through a working channel running along the body of the scope also allows the endoscopist to perform diagnostic and therapeutic interventions.Typically, a standard scope will have a diameter of 11-13 mm with a length of approximately 160 cm[2,3].Though this model has undergone subtle refinements in recent years, the basics of the technology remain largely unchanged.While being a familiar, well developed and effective tool for LGI tract diagnosis and therapy, current technologies in optical colonoscopy remain imperfect and are subject to a number of inherent limitations.These include the limited field of view, challenges identifying and treating mucosal lesions proximal to haustral folds, procedure-related pain, and risk of perforation.Pain during colonoscopy is multifactorial in origin, most often resulting from gas distension, looping of the scope and stretching of the mesocolon[4].Loop formation and mucosal scope trauma have the potential to cause significant iatrogenic injury to the bowel, especially in areas affected by disease[4,5] In addition, colonoscopy is associated with a long learning curve [typically > 200 procedures are required before 90% caecal intubation rates (CIR) are achieved[6,7]] and poor user ergonomics, which have been shown to result in musculoskeletal injury for the endoscopist[8].
Patient discomfort during LGI endoscopy is primarily responsible for 94.6% of colonoscopies being performed under intravenous sedation in Great Britain, and 96% in the United States[9].However sedation does not improve CIR, increases discharge times and is costly[10].Therefore, the development of better tolerated methods for endoscopic assessment of the large bowel with reduced sedation requirements is an urgent priority.The most serious complications associated with colonoscopy are perforation and bleeding, which occur with a frequency of 3-8per10000 and 1.6per1000 colonoscopies, respectively[1].Though these are infrequent endpoints, addressing current physical limitations with the optical colonoscope may help to further diminish their likelihood[11].Future technologies for colorectal tract assessment would ultimately benefit from being safer and better tolerated whilst simultaneously maximising on outputs in terms of key performance indicators such as achieving CIR ≥ 95% and adenoma detection rates (ADR) of ≥ 20%[1].Recent advances in medical robotics offer the potential to overcome the disadvantages of conventional colonoscopy, and engineers have been seeking to develop robotic prototypes capable of endoluminal exploration and visualisation since the early 1990s[12].In particular, the concept of ‘front-wheel’ actuation, in contrast to the ‘rear wheel’ pushing mechanism used in conventional colonoscopy has generated considerable interest, as this may possibly reduce procedural pain, the need for sedation and the incidence of iatrogenic colonic injury[13].Robotic systems may offer a wider field of view and implementation of higher degrees of motional freedom may enhance manoeuvrability and luminal views, leading to improved ADR.The introduction of semi-automated and even fully automated robotic endoscopic platforms has the potential to flatten the learning curve and minimise endoscopist fatigue[14].
The successful application of robotic devices in coronary artery bypass procedures or valvular surgery, and in advanced bronchoscopy, highlight the potential utility of this advanced technology in circumstances where the operator is performing fine tasks within a restricted working environment[15,16].The same should apply in endoscopy, though comparatively LGI endoscopy has been slow to embrace robotic technologies potentially because of perceived cost barriers, and a lack of understanding of how the technology can improve on the existing formula.Herein we provide a comprehensive narrative review of the state-of-the-art of robotics in lower GI endoscopy.
MATERIALS AND METHODS
Search strategy
Systemic review principles were adhered to in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines[17] An electronic literature search was undertaken using EMBASE, MEDLINE and Cochrane Central Register of Controlled Trials (CENTRAL) databases (from January 1, 2000 to January 7, 2021).The following MeSH terms were used: “robot”, “robotic”, “robot assist”, “colonoscopy”, “flexible sigmoidoscopy”, “proctoscopy”.Original work reviewing the use of robotic technology in lower GI endoscopy (colonoscopy, flexible sigmoidoscopy or proctoscopy) utilisingex vivoorin vivostudies in animal and human colons were included.There was no limitation on language and type of bowel pathology studied (polyp, CRC, inflammatory bowel diseaseetc.).Studies evaluating non-robotic technology, robotic technology aimed at the upper gastrointestinal tract, robotic-assisted endoscopy for minimally invasive surgery, robot assisting devices for conventional colonoscopy (such as the The EndoDrive®(ECE Medical Products, Erlangen, Germany) or the Endoscopic Operation Robot)[18] and paedia-tric endoscopy were excluded.
Data extraction
Two authors (HKSIS and EA) independently performed literature searches and determined eligibility of studies.Once consensus was reached on studies meeting predefined inclusion criteria, the following data were extracted from included studies: First author’s name, country in which the study was performed, month and year of publication, study design, components of the robotic endoscopic platform, size/length of the endoscopic capsule or flexible scope, illumination method, visualization method, actuation method, data transmission method, aim of robot intention (visualization, diagnosis, treatment, other), degree of robot navigational assistance, type of colon model and results were collected.
RESULTS
A total of 814 records were identified through initial literature searching.Duplicates and obviously irrelevant abstracts were excluded at title and abstract level, leaving 62 articles, which were reviewed fully.Twenty-five articles were further excluded because they were: Review articles (n= 13); studies evaluating robotic devices usingin vitrosynthetic colon/other (n= 4); assessing robot assistance devices coupled to a standard colonoscope (n= 2); evaluating swallowable wireless capsules without active actuation mechanisms (n= 4); evaluating surgical rather than endoscopic platforms (n= 2).A total of 37 studies were included in the final qualitative analysis (Figure 1).For ease of interpretation of this review, studies have been classified according to mode of actuation, that is the principle active method of robotic motion for each technology.Modes of actuation were defined as EM (n= 13), pneumatic (n= 11), hydraulic (n= 1), magnetic (n= 10) and hybrid (n= 2).
EM actuation
EM actuation is where electrical energy is used to bring about mechanical motion.This is usually brought about by a tether (containing wires) attached to the robotic device and to an external power source.Wireless devices without a tether will require an internal battery to provide power which takes up space.The tether will provide additional weight and friction as it slides along the mucosa which the robot will need to overcome.Either way considerable power is usually required[19,20].A summary of studies investigating this mode of actuation is provided in Table 1.

Table 1 Summary of the included studies reviewing robotic lower gastrointestinal endoscopy devices with electromechanical actuation
Two EM actuation robotic endoscopic systems were developed and received Food and Drug Administration (FDA) approval, though these are now no longer commercially available[19].The Invendoscope SC40 (Invendo Medical, Kissing, Germany) is a motorised colonoscope, controlled by a joystick and actuated by an inverted sleeve mechanism and a driving unit with 8 wheels.It is 18 mm in diameter and has a visualisation module and a 3.2 mm working channel (Figure 2).Two trials on humans have been carried out to evaluate this platform.The first, in 34 healthy volunteers showed a CIR of 82%, with 92% of patients ‘pain free’ and no acute complications were reported[21].The purported strength of this system was the combination of a highly flexible endoscope shaft with the proprietary 'inverted sleeve' technology, which the developers believed could permit potentially ‘painless’ colonoscopy, as no direct forces are applied against the intestinal walls while the device passes through narrow intestinal convolutions.Invendo medical Gmbh was acquired by Ambu A/S with plans to release a single use robotic colonoscope in 2021[19,22].Another study in 61 asymptomatic individuals with an average risk of CRC willing to undergo CRC screening found a CIR of 98.4%, with a median caecal intubation time (CIT) of 15 min.Only 4.9% of patients required sedation[23].The Neoguide Endoscopy System (Neoguide Endoscopy System Inc., Los Gatos, CA United States) has a scope diameter of 14-20 mm and consists of 16 actuator segments under EM control to bring about movement.It also contains a tip position sensor, an external position sensor and a 3.2 mm working channel.A trial on 10 individuals undergoing CRC screening or routine diagnostic colonoscopy showed a CIR of 100% with a median CIT of 20.5 min.Adenomas were successfully removed with snare or forceps and there was no evidence of complications at 30 d follow up[24].With this platform, the position and angle of the scope's tip are encoded into a computer algorithm.As the scope moves forwards, the algorithm directs each successive actuator segment to assume the same shape/position that the tip had for that given insertion depth.The insertion tube thus changes its shape at different insertion depths in a "follow-the-leader" manner, which should minimise discomfort.Neoguide Endoscopy System Inc.was acquired by Intuitive Surgical Inc.and the technology translated to robotic lung biopsy[19].Several other non-certified EM actuation devices have been developed and below these have been categorised further based on their distinct physical properties which bring about motion.
Legs:A 12-legged capsule was developed by Valdastriet al[25], comprising two motors, a bidirectional communication platform and a human machine interface (HMI) capable of semi-autonomous intrinsic EM actuation (Figure 2).The capsule measures 12.8 mm in diameter and 33.5 mm in length.The device was designed to strike a versatile balance between size and ability to traverse the bowel.The device was tested in a porcine gut model and was able to traverse the complete length of the colon (140 cm) at an average speed of 5 cm/min[25].Though a little slower in terms of pace, this device highlights the potential for miniaturisation of devices in robotic endoscopy.

learning algorithm (Q-learning and State-Action-Reward-State-Action)tube.In vivo: Swine colon–10 trials, 5 min each Average velocity with Q-learning (21 trials): 36.05 mm/min (P = 0.039).Robot with learned algorithms are more likely to pass through bends/tight passages.In vivo: Speed 11 mm/min.Best travelled distance is 55 mm.No acute mucosal damage Kim et al[28], 2010 (Korea) Paddling-based capsule endoscope: Capsule with camera module, DC motor and 6 paddles.Tether consisting of 4 cables extend from the capsule to the external controller Capsule: 15 mm in diameter and 43 mm in length.Tether: 2 m Electromechanical A camera module with 125 degree field of view and which transmits images at 10 frames per second Locomotion and safety Semiautonomous Ex vivo: Porcine colon set up in 2 positions (sloped 27.5 degrees, straight length 35 cm or sloped 37.5 degrees, straight length 62 cm).In vivo: 1 pig–8 trials Ex vivo: Velocity in sloped 27.5 degrees, straight length 35 cm colonic segment: 36.8 cm/min.Velocity in sloped 37.5 degrees, straight length 62 cm colonic segment: 37.5 cm/min.In vivo: Mean velocity: 17 cm/min over 40 cm length.Complications: Pinpoint erythema on colonic mucosa seen Wang et al[29], 2006 (China)Worm like robotic endoscope system consisting of a microrobot, controller and personal computer.The microrobot consists of a head cabin with the visualisation module and 3 mobile cells connected to the controller by an electric cable.Each mobile cell contains a linear electromagnetic driver 9.5 mm in diameter, 120 mm in length Electromechanical CCD camera and lights Locomotion Semi-autonomous Ex vivo: Porcine colon Robot travels the colon length (112 cm) in 7.3 min.Robot able to move forward, backward or remain static based on controller commands Wang et al[30], 2007 (China)Worm like robotic endoscope system consisting of a microrobot, controller and personal computer.The microrobot consists of a head cabin with the visualisation module and 3 mobile cells connected to the controller by an electric cable.Each mobile cell contains a linear electromagnetic driver.Additional deflection mechanism after the head cabin controls the camera’s pose 10 mm in diameter, 110 mm in length Electromechanical CCD camera and lights Locomotion Semi-autonomous Ex vivo: Porcine colon Robot travels the colon length (112 cm) in 7.3 min Wang et al[31], 2017 (China) Worm like robotic endoscope consisting of a head cabin and three independent segments; each segment is composed of a linear locomotor with micromotor, turbine-worm and wire wrapping-sliding mechanism.The robot is entirely covered by an external soft bellow 13 mm diameter, 105 mm in length Electromechanical Not described Locomotion and safety Semi-autonomous In vivo: Porcine colon Greater speed in straight rather than curved paths.Speed ranges from 1.62-2.2 mm/s.Robot travels the entire colon in 119 s.Distance is not specified.No breakage or damage to the colonic mucosa Naderi et al[32], 2013 (Iran)Robot with a camera, 2 clampers, 5 discs and 15 springs allowing bending and steerability, 3 motors; Driving kit, HMI in MATLAB and Joystick 19 mm in diameter, 180 mm in length.Electromechanical Camera Locomotion and safety Semi-autonomous Ex vivo: Sheep colon, 2 positions: Straight or with an 84 degree bend Velocity: Straight path: 18.4 cm/min.Curved path: 10.5 cm/min.No significant trauma Lee et al[26], 2019 (Korea)3 elastic PTFE caterpillars with worm gear, steering module, camera module, flexible shaft with steering knobs and wires, external motor and controller 130 mm in length, 55 mm maximum diameter Electromechanical LED lamps and camera Locomotion and visualisation Direct robot operation Ex vivo: 1 m excised porcine colon placed in an abdominal phantom.In vivo: 1 mini pig Ex vivo: Velocity of the robotic colonoscope: 3.0 mm/s; CIR is 50%; CIT is 8.55 min.In vivo: Failed caecal intubation with difficulty travelling through fluid and faecal material Formosa et Endoculus- treaded (4) robotic capsule CMOS camera with Locomotion, Direct robot Ex vivo: 40 cm excised Ex vivo: Able to move in forward/reverse 2 m tether Electromechanical

LEDs: Light emitting diodes; CMOS: Complementary metal-oxide-semiconductor; CIR: Caecal intubation rate; CIT: Caecal intubation time; CCD: Charged coupled device; HMI: Human machine interface.
A legged colonoscope consisting of six legs covered in silicone and a Bowden cable connecting the device to an external motor and control system was tested in excised porcine colon of varying paths to determine locomotive efficacy and safety.It was able to travel at decreasing velocities of 9.5 mm/s, 7.1 mm/s and 5.1 mm/s on straight, 30 degree curved and 60 degree curved paths, respectively.No mucosal damage or perforations were observed during testing[26].The diameter of the device is 16 mm without the legs deployed and 33 mm when they are.
Fins:A novel capsular device, 170 mm in length and 30 mm in diameter, consisting of a front body with a clockwise helical fin and rear body with an anti-clockwise helical fin was developed by a team in Japan.The bodies are connected by a DC motor and the device is computationally reinforced with learning algorithms to improve effectiveness of motion through iterative learning.It was tested inex vivoandin vivoporcine colon models andex vivotrials demonstrated improved movement performance with learned algorithms.In vivotrials showed an average speed of 11 mm/min with no acute mucosal damage[27].
Paddles:A tethered capsule endoscope containing a camera module, DC motor and 6 paddles measuring 15 mm in diameter was evaluated inex vivoporcine colon as well as in anin vivoporcine model (Figure 2).At a slope of 27.5 degrees (length: 32 cm) and 37.5 degrees (straight length: 62 cm), impressive forward motion speeds of 36.8 cm/min and 37.5 cm/min were achieved.The mean velocity reached in thein vivomodel over a distance of 40 cm was 17 cm/min.A degree of minor paddle-trauma was noted on the mucosa which may present a safety concern[28].
Worm-like:Wanget al[29,30] created two similar earth-worm like robotic endoscopes.The initial system consisted of a microrobot, controller and user interface.The microrobot in turn consists of a head cabin with the visualisation module and 3 mobile cells connected to the controller by an electric cable.Each mobile cell contains a linear electromagnetic driver[29,30].The microrobot was able to travel along the porcine colon length (112 cm) in 7.3 min[29,30].The worm-like device is pictured in Figure 2.

Figure 1 PRISMA flow diagram.
Later, a similar microrobot was created by the same team with two notable design adjustments: Each segment with this updated prototype is composed of a linear locomotor with its own micromotor, turbine-worm and wire wrapping-sliding mechanism, and the microrobot is entirely covered by an external soft ‘bellow’.The soft bellow acts to increase the friction gradient between the robot and the colonic mucosa which should improve locomotion ability.This device was tested inin vivoporcine experiments and demonstrated average speeds of up to 2.2 mm/s, with no mucosal damage reported[31].
A robot with a camera, two clampers, three motors, 5 discs and 15 springs was created to allow worm-like flexible movement.It could be driven using a joystick and is 19 mm in diameter and 180 mm long.Motion ability and safety were tested in sheep colon in a straight or curved (84 degree bend) path.The device travelled at 18.4 cm/min and 10.5 cm/min in straight and curved colonic segments, respectively.No mucosal trauma was seen[32].Overall worm-like devices appear safe with a variable speed.
Caterpillars:A robot with 3 elastic caterpillars, designed to expand the colonic lumen while causing little trauma was able to travel at 3 mm/s and achieve caecal intubation 50% of the time at 8.55 min in porcine colon placed within a human abdominal phantom[33].Unfortunately, in anin vivoexperiment, the robot failed to achieve caecal intubation as it had difficulty travelling through fluid and faeces[33].
Treads: A treaded (4 treads) robotic capsule with two motors, connectedviaa flexible tether to a control printed circuit board and laptop (Figure 2) was tested in excised porcine colon and was able to move in forward and reverse directions at 40 mm/s even with the bowel wall collapsed[34].The treads allow traction between the device and the colonic mucosa to allow effective locomotion.It was also able to pass tight haustra and make turns due to the presence of the second motor and resulting increased degrees of locomotion freedom.The device also had a visualisation module and channels for air, water and tools.Camera, insufflation, irrigation and biopsy tools all functioned effectively duringin vivoporcine testing[34].
Electropneumatic actuation
Electropneumatic (EP) actuation involves the use of pressurised gas to bring about motion.The Aer-o-scope (GI View Ltd, Ramat Gan, Israel), Endotics [ERA Endoscopy S.r.l., Peccioli (Pisa), Italy] and Sightline Colonosight systems (Stryker GI, Dallas, Tex, Haifa, Israel) are all examples of FDA approved EP robotic systems with a visualisation module and channels for insufflation, suction and irrigation.
The Aer-o-scope system works by generating a gas (carbon dioxide) pressure gradient between a rectal balloon inflated in the anus and a balloon located at the tip of the scope.Safety mechanisms ensure that the pressure in the colon does not exceed 54 m bar.The scope is only 5.5 mm in diameter (Figure 3).In vivostudies on healthy human volunteers (n= 12) or those requiring CRC screening (n= 56) have reported CIR ranging from 83%-98%, average CIT of 23 min and no acute complications other than mild mucosal petechiae in some instances[35,36].Four of twelve patients required sedation[35].In those undergoing CRC screening, the polyp detection rate was 87.5% and mucosal visualisation was rated as ‘excellent’ by participating endoscopists[30].The Aer-o-scope provides a 360 panoramic vision system in addition to a complementary metal-oxide-semiconductor (CMOS) camera which allows improved visualisation.In anIn vivostudy with 12 anaesthetised pigs with surgically simulated colonic ‘polyps’ the Aer-o-scope visualised 94.9% of polyps compared to 86.8% achieved with standard optical colonoscopy (P= 0.002)[37].

Figure 2 Examples of electromechanical robotic devices.

Figure 3 Examples of pneumatic robotic devices.
The Endotics system consists of a flexible probe with a head, body and tail, EP connector and a workstation (Figure 3).Two clampers located at the proximal and distal ends of the probe aid movement.Ex vivotesting using porcine colon has suggested that the stress exerted on the colonic wall using this device is 90% less than in standard colonoscopy[38].This should in theory translate into a reduced need for analgesia and sedation.In fact, two human trials showed that Endotics was less painful on a scale of 1 to 10 (0.9vs6.9)[38] and did not require any sedation (0%vs19.7%,P< 0.001)[39] compared to conventional colonoscopy[38,39].This device can achieve CIR as high as 92.7% within 29 min[40].Diagnostically, in individuals with a family history of CRC and/or polyps, the Endotics System showed a sensitivity, specificity, positive predictive value and negative predictive value of 93.3%, 100%, 100% and 97.7%, respectively[39].The Endotics system has also demonstrated a short learning curve: Two blocks of consecutive patients underwent LGI endoscopy using the Endotics platform with improvements in CIR (85.2%vs100%), intubation time (55 minvs22 min,P= 0.0007) and withdrawal time (21 minvs16 min)[40].Importantly, in an evaluation of 102 patients previously having undergone failed colonoscopy, 95 patients (93.2%) underwent successful caecal intubation with the Endotics system[41].
The Sightline ColonoSight system consists of a reusable scope covered by a disposable sleeve and connected to an air pressure engine[42].Shike and colleagues evaluated the performance of this system in 178 human study participants and reported a CIR of 90% with a mean CIT of 11.2 min.Scope advancement with this device is facilitated by self-propulsion of the instrument affected by an air-pressurepowered engine and LED illumination eliminates the need for fiber optics and an external light source.
Other non-certified EM actuation robotic devices include the “EndoCrawler” which consists of longitudinal and circumferential rubber bellow pneumatic actuators joined in four segments with a bending tube to allow steering between the first two segments[43].When pressurised air enters the bellow, it extends longitudinally.It has a central hollow cavity for insufflation, irrigation, suction and instrument channels as well as charged coupled device cables to pass through.It has undergoneex vivotesting in human cadaveric colon which demonstrated clear visualisation capabilities and an average speed of 200 mm/min.In vivoassessment using a live porcine model also demonstrated some encouraging findings, though difficulties were encountered when attempting to negotiate sharp bends.These issues notwithstanding, this early prototype again demonstrates the potential for self-propulsive, remotely controlled robotic devices for endoluminal assessment[43].
In 2017, a simple colonoscopy robot consisting of the robot (tip with camera, latex tubing and anal fixture) with an external pneumatic circuit was developed.Locomotion feasibility and safety was tested in porcine colon.The device was able to traverse the entire length of the colon in 71.4% of trials, able to traverse the entire length of colon with additional bends in 90.9% of trials, had an average speed of 28 mm/s with an average CIT of 54.2 s.The maximum propulsive force was 6 Ni.e., an acceptable pressure on the colonic mucosa however balloon rupture led to damage including tearing of the porcine colon[44].
A further pneumatic device consisting of three segments, each containing two soft pneumatic balloons and two rigid connectors was developed and tested in excised pig colon.The balloons are twisted in the proximal and distal gripper segments but linear in the middle propulsion segment.A camera and channels for air flow and instruments are built in.The unactuated device is 22 mm in diameter.The robot travelled at 1 mm/s and was able to clearly visualise the colonic mucosa[45].
A summary of all studies evaluating robotic EM actuation systems for LGI endoscopy is provided in Table 2.
Hydraulic actuation
Hydraulic actuation uses a pressurised fluid medium such as water to progress through the colon.A meta-analysis of randomised controlled trials has previously shown that water immersion colonoscopy does significantly decrease pain scores and sedation rates without affecting the diagnostic quality or completeness of colonoscopy when compared with air intubation[46].
The “Hydraulic Colonoscope” system consists of a colonic vehicle (CV) connected to external pumps and valvesviaa tether.The CV contains a magnetic tracker and is surrounded by a balloon which may be inflated or deflated to create an appropriate seal with the colonic wall.The pump system is used to pump water into the colon behind the CV.An anal port prevents water from escaping the colon.Motion ability was trialled in porcine colon and compared to conventional colonoscopy.The device was able to reach the caecum in all attempts.There was no difference in the CIT or caecal pressure between the device and colonoscopy.However, significant differences were found in the maximum force exerted on the colon (0.63 Nvs2.2 N,P= 0.004), maximum anal pressure (1.53 kPavs4.53 kPa,P= 1 × 10-7) and mean anal pressure (0.05 kPavs1.5 kPa,P= 0.0003) between the device and conventional colonoscopy, respectively[47] (Table 2).

Table 2 Summary of the included studies reviewing robotic lower gastrointestinal endoscopy devices with pneumatic or hydraulic actuation
Magnetic actuation
Magnetic actuation is brought about externally through magnetic fields created either by an external permanent magnet (EPM) or electromagnetic coils[48].Control of this field is crucial for locomotion as controlling the field allows movement of the device in a particular direction and orientation.The main advantage of external magnetic actuation is that it allows a ‘front-wheel’ motion without the need for large internal actuating motors.When an EPM is used, small internal permanent magnets (IPMs) incorporated into the luminal robot are required to generate the magnetic field.A power supply is generally not required.The resulting device is therefore less bulky and more likely to reduce pain and the need for sedation.Additionally, there is more scope to incorporate other subsystems.The EPMs can be moved manually and the magnetic field controlled directly by the user to cause luminal device movement.However, movement is non-linear and therefore complex.Other disadvantages include the ongoing need for insufflation and the continuous contact between the device and the colonic mucosa due to the continuous attraction between the EPM and IPM[48].The magnetic fields generated may also interfere with nearby equipment as they are permanent and cannot be turned on or off[3].Electromagnetic coils can improve control over the magnetic field however they do require a power supply[19].We have further classified these devices into whether or not they are wireless or tethered.

100%; Negative predictive value: 97.7%Trecca et al[40], 2020 (Italy) Endotics System [ERA Endoscopy S.r.l., Peccioli (Pisa), Italy]: Second generation system- Workstation with console and disposable flexible probe.The probe has 2 clampers to aid locomotion and a head (contains the camera, LEDs, chromoendoscopy and channels for suction, irrigation and insufflation) a body and a tail 23-37 cm in length, 17 mm in diameter Pneumatic LED light source, chromoendoscopy and CMOS camera with a field of view of 140 degrees Learning curve, visualisation and diagnostic accuracy, safety Semiautonomous In vivo: n = 55 Humans, requiring diagnosis, CRC screening or surveillance.Training progress was evaluated by comparing two consecutive blocks of patients i.e.group A (first 27) and group B (last 28)CIR is 92.7%.Median CIT is 29 min.Median withdrawal time is 18 min.Polyp detection rate: 40%; Adenoma detection rate: 26.7%; Advanced neoplasm: 0%; Complication: 1.8%-bleeding with polypectomy; Successful polypectomy and hot biopsy coagulation for bleeding.Mean VAS pain/discomfort: 1.8.Learning curve assessment, Group A vs Group B: CIR: 85.2% vs 100%.Median CIT: 55 min vs 22 min (P = 0.0007).Median withdrawal time: 21 min vs 16 min Tumino et al[41], 2017 (Italy) Endotics System (ERA Endoscopy S.r.l., Peccioli (Pisa), Italy): Workstation with console and disposable flexible probe.The probe has 2 clampers to aid locomotion and a head (contains the camera, LEDs and channels for suction, irrigation and insufflation) a body and a tail 25-43 cm in length, 17 mm in diameter Pneumatic LED light source and CMOS camera with a field of view of 110 degrees Visualisation and performance Semiautonomous In vivo: n = 102 Humans, previously failed caecal intubation on colonoscopy CIR was 93.1% and therefore had a 95% performance.Mean CIT was 51 min Shike et al[42], 2008 (Italy/Israel/United States)Sightline ColonoSight (Stryker GI, Dallas, Tex, Haifa, Israel): A reusable scope with LEDs and camera at the tip and steering dials proximally.Tips is covered by a disposable sleeve with 3 working channels for suction, irrigation, insufflation and instruments.Electropneumatic unit, control unit and video monitor Not described Pneumatic LED light source and camera Visualisation, diagnosis and treatment Semiautonomous In vivo: 2 pigs–To assess safety in terms of bacterial transmission to the reusable scope with a disposable sleeve covering.In vivo: 178 Humans, healthy volunteers and various clinical indications for colonoscopy In vivo, Pigs: E.coli and E.Fergusonii from scope handle, shaft and tip before the procedure: Nil growth.E.coli and E.Fergusonii from scope handle, shaft and tip after the procedure: Nil growth.E.coli and E.Fergusonii from sheath covering after the procedure: Heavy growth.In vivo, Humans: CIR is 90%.Mean CIT is 11.2 min.Diagnoses of diverticulosis, polyps, colitis, haemorrhoids, normal or other was given.Successful polypectomy, biopsy and argon plasma coagulation.No complications at 2 wk follow up Ng et al[43], 2000 (Singapore)EndoCrawler: Longitudinal and circumferential rubber bellow actuators joined in four segments with a bending tube to allow steering between the first two segments and vision module; Central hollow cavity for instruments, insufflation, irrigation and suction channels and CCD cables.These exit the proximal end as a flexible cable similar to a colonoscope; LabWindows user interface and joystick 28 mm in diameter, 420 mm length Pneumatic CCD camera and light source Locomotion and visualisation Direct robot operation Ex vivo- Cadaveric colon.In vivo-Pig Ex vivo: Clear visualisation of colonic wall.Speed: 200 mm/min however required external pushing and couldn’t progress beyond bends unless the head was deflected away from the colonic wall.In vivo: ‘Red out’ images throughout most of the robot’s journey.Average speed: 150 mm/min with external pushing.Unable to progress beyond an acute bend Able to traverse the entire length 71.4% (10/14 trials).Able to traverse the entire length with additional bends 90.9% (10/11 trials).Robot speed of 28 mm/s (5 trials).Average CIT is 54.2 s.(5 trials).Maximum propulsive force is 6 N (44 mmHg) which is less than the safe intraluminal pressure of 80 Dehghani et al[44], 2017 (United States)Pneumatically driven colonoscopy robot consisting of the robot (tip with camera, latex tubing, tethered camera and anal fixture) and external pneumatic circuit and electric circuit with laptop Not described Pneumatic Camera Locomotion feasibility and safety Semiautonomous Ex vivo: 1.5 m porcine colon in human phantom.Tests repeated 5-14 times depending on analysis performed

LEDs: Light emitting diodes; CMOS: Complementary metal-oxide-semiconductor; CIR: Caecal intubation rate; CIT: Caecal intubation time; CCD: Charged coupled device; HMI: Human machine interface; CV: Colonic vehicle.
Wireless capsules
A swallowable wireless capsule with the aim of therapeutic control of bleeding was developed[49].It consists of a surgical clip, 4 IPMs and a bidirectional communication platform and is able to actively locomoteviaa magnetic link generated by its interaction with an EPM.The EPM is mounted on a passive hydraulic arm that is moved manually by the user.A HMI under direction by the controller controls clip deployment.When tested 10 times inex vivoporcine colon, the clip release occurred 100% of the time and was instantaneous.Moving the capsule was effective and fast although it took 2-3 min to align it appropriately against the mucosa to be clipped.In vivoin a pig, ‘good’ movement and positioning of the device with the EPM was observed.The clip was released successfully onto the desired target and it remainedin situ.The amount of tissue grasped was also satisfactory.This capsule was 12.8 mm in diameter and 33.5 mm in length[49].
Another wireless capsule with a set of IPMs, inertial and vision sensors and vision module, with an EPM mounted on a robotic arm was created[50].The robotic arm was moved intelligentlyviaclosed loop steering and the HMI (Figure 4).Visualisation, motion feasibility and learning curve were tested in insufflated or collapsed porcine colon (500 mm) placed in a human abdominal phantom.In the collapsed colon, the device was only able to travel very short distances whereas there was a 100% success rate in traversing the whole length when the colon was insufflated with air.The average time required was 10 min.Novice medical doctors were able to drive the EPM in an effective way within 40 trials[50].Using a robotic arm to steer the EPM was shown to provide better manoeuvrability and lesion detection rates compared to manual steering of the EPM[51].
Carpi and colleagues used the readily available PillCam capsule created by Given Imaging Ltd, Israel to visualise the small bowel and covered it in a magnetic shell to create a simple wireless capsule capable of magnetic actuation.The magnetic link was created between the shell and two EPMs controlled by a magnetic navigation system (Niobe, Stereotaxis, Inc, United States).This navigation system is already clinically in use in the field of robotic cardiology.A remote computer workstation and mouse was used to navigate the capsule.In vivotesting in a pig showed simply that such a capsule is capable of travelling through the colon without causing damage[52].
The magnetic controlled capsule endoscopy (MCCE) system (Chongqing Jinshan Science & Technology Group Co, Ltd) consists of an ingestible colon capsule with IPM and battery, an external magnetic manipulator with EPM, and an image transmission system.The capsule measures 27.9 mm in length and 13.0 mm in diameter.It was tested in 52 volunteers for CRC screening.The average time to reach the caecum was 3.63 h.Manoeuvrability of the capsule was good (94.3%) or moderate (5.77%).It was capable of providing good-quality pictures and identified 6 positive findings (polyps, diverticulum) which were confirmed by colonoscopy.All volunteers were able to swallow the capsule and excreted the capsule within 2 d.Complications included 7 mild adverse events (abdominal discomfort, nausea, and vomiting) lasting 24 h only[53].
Tethered capsules
Using the technology from[51] the “Magnetic Air Capsule”, a device consisting of a capsule like frontal unit and a compliant multi-lumen tether was created[13].The incorporation of the multi-lumen tether allows for intervention in addition to basic colonoscopy functions.The frontal unit contains a vision module, an IPM, a magnetic field sensor, and two channels, one for lens cleaning and the other for insufflation/suction/irrigation or instrument passage.The capsule is 11 mm in diameter, 26 mm in length and the tether is 2 m in length.12 trials in 850 mm porcine colon placed in a human abdominal phantom with attached coloured beads (5 mm) mimicking polyps showed an 85% detection rate.100% of which were successfully removed with a polypectomy snare.The mean completion time (inspection of the colon as well as removal of the ‘polyps’) was 11.3 min.Six trials in anaesthetised pigs showed device ability to navigate around bends and folds, retroflexion capability and successful operation of the working channels without a loss of magnetic link.In addition, there was no mucosal damage[13].Using a similar prototype (Figure 5), visualisation and diagnostic ability was assessed 22 times in 850 mm of porcine colon and compared to that of colonoscopy.CIR for both was 100%.Compared to colonoscopy, pin detection rate was lower (80.9% withvs85.8%) and procedure completion time (visualisation and diagnosis) was significantly longer [556 svs194 s (P= 0.0001)].There was no difference in intuitiveness score[54].

Figure 4 An example of a magnetic device device by Ciuti et al[50].
Further advancement led to the “Magnetic flexible endoscope” (MFE).This tethered robot has a standard visualisation module and working channels for instruments, irrigation and insufflation.Additionally, it has a unique retroflexion control algorithm to improve this repetitive but technically challenging skill.Autonomous retroflexion ability was examined 30 times in an anaesthetised pig.Successful retroflexion manoeuvres with a mean time of 11.3 s were performed 100% of the time.No acute tissue trauma or perforation was seen[55].A comparison of different degrees of locomotion autonomy was performed recently using the MFE in two pigs[14].Completion times for Direct robot operationvsteleoperationvssemi-autonomous operationvscolonoscopy showed similar results over distances of 45 cm (9 min 4 svs2 min 20 svs3 mins 9 svs1 min 39 s) and 85 cm (unable to reach markervs8 min 6 svs9 min 39 svs3 min 29 s).Intelligent and semi-autonomous control had NASA Task Load Index[56] mean ratings lower/less demanding than colonoscopy or direct robot operation[14].
An Endoo capsule with a permanent magnet, visualisation module, tether with 4 working channels for suction, insufflation, irrigation and instruments was developed in Italy within a European H2020 project[57].The system consists of an external robot with EPM, a localisation system and medical workstation with a joystick.The workstation and joystick allow the user to control all functions of the Endoo capsule (Figure 5).In addition, the vision system contains 4 green/blue UV-LEDs.Compared to colonoscopy CIR was 67%vs100% at 9.5 minvs3.5 min respectively.Interaction forces between the Endoo capsule and colonic wall as well as polyp detection rates was lower than colonoscopy [1.17 Nvs4.12 N; 87%vs91% (P= 0.16)].The magnetic link was lost an average of 1.28 timespercomplete procedure, but it was restored in 100% of cases[57].All studies are summarised in Table 3.
Hybrid actuation
Hybrid actuation involves the combination of different propulsive mechanisms to achieve motion.A wireless endocapsule consisting of a 3 legged mechanism, DC motor, battery and small IPMs was created and tested by Simi and colleagues (Figure 6)[58].Magnetic and EM mechanisms are combined here: The IPMs interact with an EPM to primarily move and orient the capsule while the legged mechanism is used to extract the capsule out of collapsed areas of the colon when it might otherwise get trapped.Motion feasibility was examined 10 times on 20 cm porcine colon and in 4 anaesthetised pigs.In theex vivotrials, the average time taken to travel 20 cm and number of times the legs were activated was 4 min with 5 activations.The average speed was 5 cm/min.In thein vivotrials, the average time taken to travel 40 cm and number of times the legs were activated was 5 min with 5 activations.The average speed was 8 cm/min.The colon was not insufflated with air[58].In Japan, a selfpropelling capsule was created by attaching a silicon resin fin with micro-magnet to the commercially available Pillcam SB2 capsule (Covidien, Dublin, Ireland).In the presence of a magnetic field and water, the fin vibrates and propels the capsule.When placed in the rectum and descending colon of a human subject, it was shown to be able to swim forwards and backwards without causing damage to the mucosa however it had difficulty by-passing the bend of the sigmoid colon[59] (Table 3).

Figure 5 Examples of tethered magnetic robotic devices.
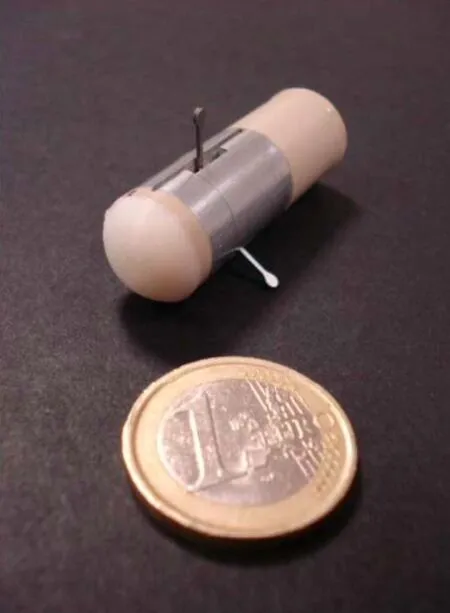
Figure 6 Hybrid robotic device by Simi et al[58].

Table 3 Summary of the included studies reviewing robotic lower gastrointestinal endoscopy devices with magnetic or hybrid actuation

visualised via colonoscopy 5 h after ingestion were confirmed by colonoscopy.78% reached the rectosigmoid colon in 25 min.All 57 volunteers were able to swallow the capsule and excreted the capsule within 2 d.Complications: 7 mild adverse events (abdominal discomfort, nausea, and vomiting) lasting 24 h.No complications at one week follow up Valdastri et al[13], 2012 (Italy)MAC consists of capsule-like frontal unit and a compliant multi-lumen tether.The frontal unit contains a vision module, an IPM, a magnetic field sensor, and two channels, one for lens cleaning and the other for insufflation/suction/irrigation or instrument passage.The IPM is controlled by an EPM mounted on a robotic platform.A control device allows the user to directly control the position of the EPM.The working distance is 150 mm.The tether connects to an external control box Capsule: 11 mm diameter, 26 mm in length.Tether: 5.4 mm diameter, 2 m length Magnetic CCD camera with 120 degree field of view and 4 white LEDs Diagnostic and treatment ability, safety, usability Intelligent teleoperation Ex vivo: 850 mm porcine colon in human phantom model–12 trials.In vivo: 2 Pigs–3 trials each Ex vivo: Mean percentage of 5 mm coloured beads (polyps) detected was 85%.100% successful removal (polypectomy loop) of identified beads.Mean completion time (inspection and bead removal) was 678 s.Mean bead removal time was 18 s.Good manoeuvrability, low friction from the tether on the colon wall and reliable feedback from the vision module.In vivo: No mucosal damage or perforation.Able to navigate around bends and folds, retroflexion of the camera and successful operation of the tools (loop, forceps, retrieval basket, grasper) without loss of magnetic link Arezzo et al[54], 2013 (Italy)Robotic arm with EPM controlled by HMI and controller; Wired capsule with 3 IPMs, camera, LEDs and magnetic sensor.The working distance is 150mm.The wired sheath allows transmission from the vision module and electric energy Capsule: 13.5 mm in diameter and 29.5 mm in length.Wired sheath: 2 mm in diameter Magnetic CCD camera with 120 degree view and 6 white LEDs Visualisation and diagnostic ability compared to colonoscopy Intelligent teleoperation Ex vivo: 850 mm porcine colon in human phantom model–22 trials each for capsule and colonoscope Robot vs colonoscopy: CIR: 100% for both.Pin detection rate: 80.9% vs 85.8%.Procedure completion time (visualisation and diagnosis): 556 s vs 194 s (P = 0.0001).No difference in intuitiveness score Slawinski et al[55], 2018 (United States/United Kingdom)MFE with IPM, camera, illumination module, working channel for instruments, channel for irrigation and insufflation, EPM on robotic arm and HMI.Additional sensing, retroflexion and software control systems Tip: 20.6 mm in diameter and 18.1 mm in length.Body: 6.5 mm in diameter Magnetic Camera and illumination module Retroflexion ability Intelligent teleoperation with task autonomy In vivo: 1 Pig–30 trials 100% successful retroflexion manoeuvres with a mean time of 11.3 s.No acute tissue trauma or perforation First porcine model–colon distance of 45 cm: Task completion times for direct robot operation, teleoperation, semiautonomous operation and conventional colonoscopy were 9 min 4 s, 2 min 20 s and 3 min 9 s and 1 min 39 s, respectively.Second porcine model-colon distance of 85 cm: Task completion times for, teleoperation, semi-autonomous operation and conventional colonoscopy were 8 min 6 s, 9 min 39 s and 3 min 29 s, respectively.It was not possible to reach the marker with direct robotic operation.Intelligent and semi-autonomous had Martin et al[14], 2020 (United Kingdom)MFE with an IPM, camera, an insufflation channel, irrigation channel, working channel for instruments and localisation circuit; A robotic arm with EPM; Robot operating system and joystick Capsule: 20.6 mm in diameter and 18.1 mm in length.Tether: 6.5 mm in diameter Magnetic Camera and LED Comparison of different degrees of autonomy for locomotion and novice usability Direct robot or intelligent teleoperation or semi-autonomous In vivo: 2 Pigs–3 trials for each MFE control and colonoscopy in the first pig and 4 trials for each in the second pig

IPM: Internal permanent magnet; EPM: External permanent magnet; HMI: Human machine interface; LEDs: Light emitting diodes; CMOS: Complementary metal-oxide-semiconductor; CIT: Caecal intubation time; CIR: Caecal intubation rate; CCD: Charged coupled device; MCCE: Magnetic controlled capsule endoscopy; MFE: Magnetic flexible endoscope.
DISCUSSION
Medical robotics is realising its potential in a variety of healthcare disciplines, and the last couple of decades have seen increasing demand for robotic platforms designed specifically for endoscopy.In terms of LGI tract ‘robo-endoscopy’, significant strides have been made over this period, with five devices receiving FDA approval.These devices represent a heterogeneous group in terms of actuation modality (EM or pneumatic), and many studies have been performed usingex vivomodels.These models, while able to demonstrate proof of concept, cannot effectively capture data onin vivomotion ability, pain perception or device safety.Nevertheless, the human data that is available suggests that the evaluated robo-endoscopic systems are able to locomote effectively (i.e., achieve CIR > 90%[23,24,36,40-42]), to locomote safely (i.e., be associated with mild if any mucosal disruption or complications[21,24,35,36,40,42])and to achieve endoscopic tasks with minimal associated pain[21,23,35,39].Reducing discomfort associated with LGI endoscopy represents a key directive in robotic endoscopy and in two trials, human participants gave the Invendoscope an average pain score of 1.96/6 and 2.6/6, which translated into 0% and 4.9% requiring sedation, respectively[21,23].When compared to colonoscopy, pain scores and sedation rates were also significantly lower with the Endotics system[38,39].Early data suggest that the Endotics system may even have superior diagnostic capabilities compared with conventional colonoscopy as indicated by its ability to detect lesions missed on colonoscopy[38].These reports are certainly encouraging, though overall it is important to appreciate that most devices presented in this review remain in the relatively early phases of translational application, and few have met the goal of clinical deployment outside of academic institutions.An inherent limitation lies in the fact that most systems provide primarily diagnostic functionality, with large scale trials evaluating therapeutic robotic LGI endoscopy currently lacking.
Improved reproducibility, enhanced procedural efficiency and a shorter learning curve have all been suggested as possible areas where robotic endoscopy could make a positive impact.In addition, they may offer a more comfortable system for the user, which may have potential to minimise fatigue and injury and ultimately this may equate to more years of professional service.More intuitive control and visualisation systems have the potential to shorten learning curves.For example, one trial evaluating a robotic endoscopic system suggested that only an average of 30 procedures was required for the user to achieve CIR, CIT and scope withdrawal time comparable to standard colonoscopy performed by an ‘expert’[40].
From a broader perspective, it is important to acknowledge that this review has focused entirely on the specific application(s) of robotic systems in LGI endoscopy.However, robotic advances in this area are not made in isolation from advances in other luminal organs such as the upper GI tract or in natural orifice transluminal endoscopic surgery.Thus, it is likely that advances in one field will complement another.
One can anticipate that in the future, as the technology becomes more sophisticated, it should be possible to exploit the ‘computational interface’ that robotic endoscopy provides further, with the potential for integration of AI based algorithms and novel augmented reality systems for ‘smart’ therapeutics.It is doubtful whether these nextgeneration technologies will work to their full capabilities if operating within anything other than a robotic system.It is an exciting time in medical robotics with recent reports confirming the potential for the development of ‘soft’ robotic systems with inbuilt autonomic functionality[60].Such systems are likely to represent the long-term direction of luminal robotics.In the near- to mid-term, the goal will be to continue to stimulate strong collaborative links between GI physicians and medical engineers in order to continue to refine design and functionality.
CONCLUSION
Robotic technologies have the potential to transform LGI endoscopy into a quicker, safer, more reliable and less painful procedure.In the long term, benefits for patients, endoscopists and the wider healthcare industry are foreseeable, though these have yet to be convincingly demonstrated in human trials.Most studies to date have employedex vivomodelling and high quality level 1 evidence is currently lacking in this field.Robotic technologies are evolving with such rapidity at the moment, that future roboendoscopic systems are likely to look and behave very differently to conventional master-slave systems currently in use.Exciting developments in 3D printing, soft robotics, autonomous functionality and augmented reality are likely to converge over the coming decade to lead to the development of truly next generation robotic endoscopy devices.
ARTICLE HIGHLIGHTS
Research background
Inherent limitations exist with conventional colonoscopy which may be overcome by a variety of next-generation robotically-augmented technologies.
Research motivation
Robotic technologies have the potential to transform lower gastrointestinal (LGI) tract endoscopy with long term, benefits for patients, endoscopists and the wider healthcare industry.High quality evidence is currently lacking in this field.
Research objectives
This review provides a comprehensive summary of recent developments in the application of robotics in LGI tract endoscopy.
Research methods
A systematic review of the literature was performed.Studies reporting on the use of robotic endoscopic technology in ex vivo colon models or in vivo animal and human experiments were included.
Research results
Of 37 studies were included of varying actuation modality.Five devices have been approved by the Food and Drug Administration, however the majority remain in the early phases of testing and development.Level 1 evidence is lacking at present, but early reports suggest that these technologies may be associated with improved pain and safety.
Research conclusions
Significant progress in robotic colonoscopy has been made over the last couple of decades.The reviewed devices appear to be ergonomically capable and efficient though to date no reports have convincingly shown diagnostic or therapeutic superiority over conventional colonoscopy.
Research perspectives
Future improvements in design together with the integration of semi-autonomous and autonomous systems over the next decade will potentially result in robotic colonoscopy becoming more commonplace.?
 World Journal of Gastrointestinal Endoscopy2021年12期
World Journal of Gastrointestinal Endoscopy2021年12期
- World Journal of Gastrointestinal Endoscopy的其它文章
- Efficacy and tolerability of high and low-volume bowel preparation compared: A real-life single-blinded large-population study
- Role of endoscopic ultrasound guided fine needle aspiration/biopsy in the evaluation of intra-abdominal lymphadenopathy due to tuberculosis
- When should we perform colonoscopy to increase the adenoma detection rate?
- Large polyps: Pearls for the referring and receiving endoscopist
- Primary prophylaxis of variceal bleeding in patients with cirrhosis: A comparison of different strategies
- Endoscopic ultrasound-guided biliary drainage-current status and future perspectives