
Role of endoscopic ultrasound guided fine needle aspiration/biopsy in the evaluation of intra-abdominal lymphadenopathy due to tuberculosis
2022-01-04 09:44:00HarshavardhanRaoPriyaNairKrishnaPriyaArchanaGeorgeVallonthaielDipuSathyapalanAnoopKoshyRamaVenu
Harshavardhan Rao B, Priya Nair, S Krishna Priya, Archana George Vallonthaiel, Dipu T Sathyapalan, Anoop K Koshy, Rama P Venu
Harshavardhan Rao B, Priya Nair, S Krishna Priya, Anoop K Koshy, Rama P Venu, Department of Gastroenterology, Amrita Institute of Medical Sciences, Kochi 682041, Kerala, India
Archana George Vallonthaiel, Department of Pathology, Amrita Institute of Medical Sciences, Kochi 682041, Kerala, India
Dipu T Sathyapalan, Department of Internal Medicine, Amrita Institute of Medical Sciences and Research Centre, Kochi 682041, Kerala, India
Abstract BACKGROUND Intra-abdominal lymphadenopathy due to tuberculosis (TB) poses a diagnostic challenge due to difficulty in tissue acquisition.Although endoscopic ultrasound guided fine needle aspiration/biopsy (EUS-FNA/B) has shown promise in the evaluation of mediastinal lymph nodes, its role in the evaluation of intra-abdominal lymphadenopathy is not clear.AIM To assess the role of EUS-FNA/B in the evaluation of intra-abdominal lymphadenopathy due to TB.METHODS This was a retrospective study where patients with intra-abdominal lymphadenopathy who underwent evaluation with EUS-FNA/B were included.TB was diagnosed if the patient had any one of the following: (1) Positive acid fast bacilli (AFB) stain/TB GeneXpert/TB-polymerase chain reaction/AFB culture of tissue sample; and (2) Positive Mantoux test and response to anti-tubercular therapy.EUS-FNA reports, clinical reports and imaging characteristics of patients were recorded for a detailed analysis of patients with TB.RESULTS A total of 149 patients underwent an EUS-FNA/B from lymph nodes (mean age 51 ± 17 years, M:F = 1.2).Benign inflammatory reactive changes were seen in 45 patients (30.2%), while 54 patients (36.2%) showed granulomatous inflammation with/without caseation.Among these, 51 patients (94.4%) were confirmed to have TB as per pre-defined criteria.Patients with TB were more likely to have hypoechoic and matted nodes [40 patients (67.7%)].EUS-FNA/B was found to have a sensitivity and specificity of 86% and 93% respectively, with a diagnostic accuracy of 88% in the evaluation of intra-abdominal lymphadenopathy due to TB.CONCLUSION EUS-FNA/B has a high diagnostic yield with a good sensitivity and specificity in the evaluation of intra-abdominal lymphadenopathy due to TB.However, the validity of these findings in populations with low prevalence of TB needs further evaluation.
Key Words: Endoscopic ultrasound; Lymph nodes; Tuberculosis; Mesenteric; Intraabdominal
INTRODUCTION
Intra-abdominal lymphadenopathy due to tuberculosis (TB) is a common clinical entity in regions endemic for the disease.The presence of concomitant lung parenchymal findings can aid in the diagnosis of these patients[1].However, isolated mesenteric lymphadenopathy usually poses a significant diagnostic challenge[1-3].Multiple factors including clinical scenario, number, size and imaging characteristics have been described that can help in the differential diagnosis of patients with intraabdominal lymphadenopathy[4].Moreover, a positive Mantoux test and/or adenopathy with peripheral rim enhancement with a low density center is supportive for TB at best with fungal infections, atypical mycobacteria and sarcoidosis also presenting with a similar clinical picture[5,6].The causes of mesenteric lymphadenopathy other than TB include sarcoidosis, lymphoma, metastatic deposits from other malignancies and other rare infectious causes[7].
Tissue acquisition is usually essential for establishing the diagnosis in patients with intra-abdominal lymphadenopathy.Earlier, tissue acquisition was accomplished by computed tomography guided/laparoscopy assisted biopsy.Currently, these modalities have largely been replaced by endoscopic ultrasound guided fine needle aspiration/ biopsy (EUS-FNA/B) over the last decade owing to superior reliability and safety profile and is now the modality of choice in the evaluation of intraabdominal and mediastinal lymphadenopathy.EUS has been reported to be capable of imaging and enabling tissue sampling from nodes as small as 5 mm[8].It has also been proven to be safe for tissue acquisition from lymph nodes with a reported complication rate of less than 0.5%[9].
EUS-FNA/B has been shown to be invaluable in the diagnosis of malignancy (primary/metastatic) during evaluation of intra-abdominal lymphadenopathy.There is also a growing body of evidence that highlights the role of EUS-FNA/B in the manage-ment of mediastinal lymphadenopathy[4-6,10].However, there is no clarity on the efficacy of EUS-FNA in the evaluation of intra-abdominal lymphadenopathy due to TB.In this study, we analyzed the patients who underwent EUS-FNA for intraabdominal lymphadenopathy, at a high-volume tertiary care center and assessed the diagnostic yield of EUS-FNA for TB in these patients.
MATERIALS AND METHODS
This was a single center retrospective study conducted in a large tertiary care hospital where patients with intra-abdominal lymphadenopathy referred for EUS-FNA/B between January 1, 2015 and December 31, 2019 were included.Institutional ethics committee clearance for data acquisition and analysis were obtained.All relevant data such as patient demographics (age, gender, comorbidities), procedure details (type of needle, number of passes, size of nodes, echogenicity) and post-procedure complications were noted.On retrospective analysis, TB was diagnosed if the patient had any one of the following: (1) Positive acid fast bacilli (AFB) staining of the tissue sample/ positive TB GeneXpert of the tissue sample/positive TB-polymerase chain reaction (PCR) of the tissue sample; (2) Granulomas with caseation; (3) Positive AFB culture; and (4) Positive Mantoux test and an adequate response to anti-tubercular therapy (ATT).EUS-FNA reports, demographics and imaging characteristics of patients with TB were studied in detail to determine the diagnostic yield of the procedure.
EUS procedure
All EUS-FNA procedures were performed by an experienced endosonographer.Institutional protocol was followed wherein procedures were performed under moderate or deep sedation which was provided by a dedicated anaesthetist.All patients received prophylactic antibiotics prior to the procedure asperprotocol.Initial diagnostic endosonographic evaluation was carried out using a linear array echoendoscope (Olympus GFUCT180, Tokyo, Japan) and upon identification of the lymph nodes, relevant imaging characteristics were noted.Only EUS-FNA/B results of abdominal lymph nodes were analyzed in the study.All procedures were performed with Rapid On-Site Evaluation (ROSE) by a dedicated cytopathologist.Depending upon the site of the nodes, gastric or duodenal approaches were considered.A 22 gauge needle was used for all procedures.A FNA needle (22G Cook EchoTip®, 22G Olympus EZ-shot 3) was used in most cases; while a fine needle biopsy needle (22G Boston Scientific Acquire™) was used in only 10 patients.The needle was passedviathe instrument channel and the node was targeted under sonographic guidance.The sharp tip of the needle punctured the node after unlocking the needle apparatus and multiple passes were made into the target node.Suctioning was reserved for cases where the initial few passes were inadequate as assessed by the on-site cytopathologist.The needle was passed multiple times into the node typically for 20-30 s each pass while continuously adjusting the position of the needle in a “fanning” pattern to maximize tissue volume.The needle was then removed from the endoscope, and the tissue was prepared for pathological examination.
Pathological examination
All the FNA material was placed onto glass slides and smears were made.Smears for ROSE were fixed in 80% isopropyl alcohol which was then rapidly stained with 1% Toluidine blue.The on-site cytopathologist evaluated the adequacy of tissue in each pass and also gave a preliminary opinion on pathological changes on the slide.The number of passes were determined on the basis of this information until a maximum of 5 passes were made.When staining was complete, all EUS-FNA specimens were evaluated for cytological diagnosis and cellular preservation by a pathologist.These slides were subsequently stained with Papanicolaou stain in the cytology laboratory for further evaluation.Visible core tissue was placed in formalin-alcohol mixture (formalin and 80% isopropyl alcohol in 1:1 ratio) and subsequently paraffin embedded to produce cell blocks.Sections from the cell blocks were stained with hematoxylin and eosin.The slides were meticulously observed to arrive at a final diagnosis.
On pathological examination, reactive nodes will exhibit a polymorphous lymphoid population including mature lymphocytes, germinal center cells and tingible body macrophages.Granulomatous inflammation was diagnosed when there were collections of epithelioid histiocytes forming an epithelioid cell granuloma with or without necrosis(Figure 1).In such cases, further sampling was performed with microbiological tests such as AFB staining, GeneXpert and TB culture.Diagnosis of lymphoma was applicable when the lymphoid cells were monomorphic populations of atypical lymphoid cells.Secondary malignant deposits in the node were identified when tumor cells were admixed with a reactive lymphoid population.
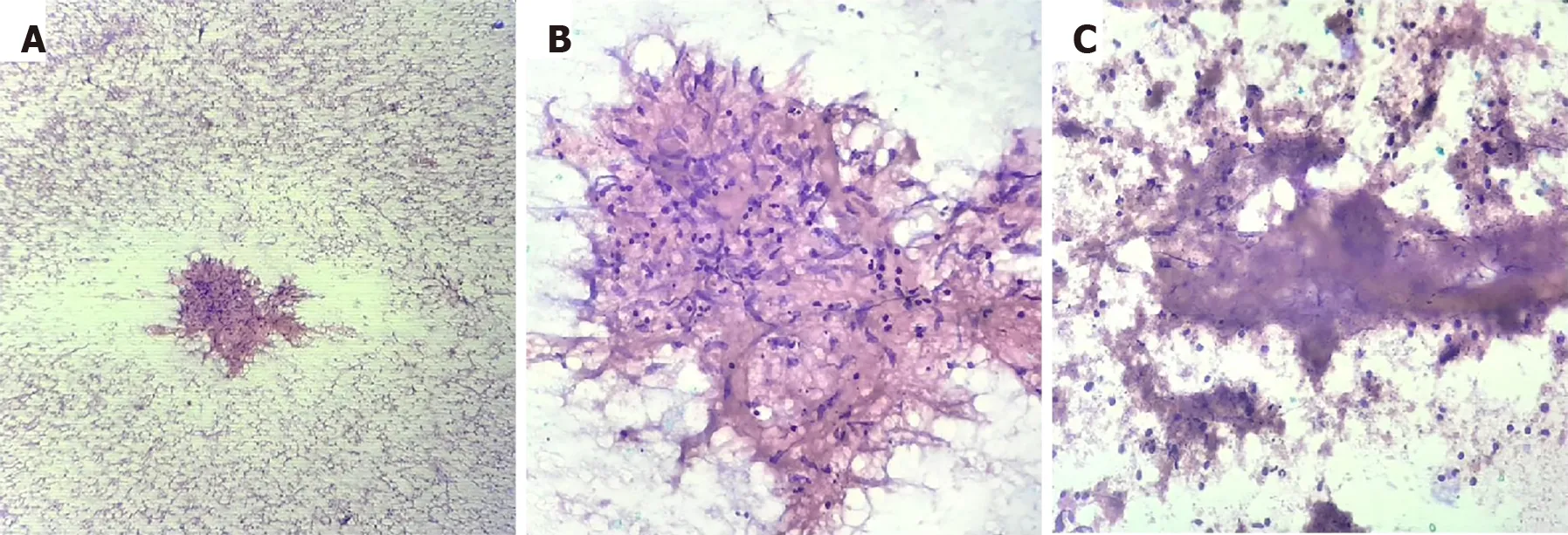
Figure 1 Histopathology findings on the fine needle aspiration sample of a patient with tuberculosis.
Diagnosis and follow-up
Patients with features of lymphoma or metastatic malignancy were treated with an appropriate chemotherapy regimen asperhospital protocol by the oncologist.Patients with TB as defined above, received ATT for 6 mo.Patients with sarcoidosis were treated with steroids.All patients were followed up 15 d after the procedure to discuss biopsy findings and treatment plan.All patients were followed up clinically every month for symptomatic improvement or drug side effects.
Statistical analysis
Statistical analysis was carried out using IBM SPSS software version 20.0.The pathology reports were correlated with clinical diagnosis in order to determine the diagnostic validity of EUS-FNA in the evaluation of intra-abdominal lymph nodes resulting from TB.A descriptive analysis of all patients with TB was carried out.Comparisons of means for continuous variables were carried out using the independent 2-samplettest and Mann Whitney U tests for parametric and non-parametric variables, respectively.Categorical variables were analyzed using Chi square test/Fisher’s Exact test.AP< 0.05 was considered statistically significant.
RESULTS
EUS-FNA/B in the evaluation of intra-abdominal lymphadenopathy
A total of 149 patients underwent EUS-FNA/B of lymph nodes.The mean age of these patients was 51 ± 17 years with a male to female ratio of 1.2.The most common clinical presentation was fever of unknown origin [78 patients (52.3%)], whereas, 48 patients (32.2%) underwent EUS-FNA of lymph nodes for staging of malignancy and the remaining 23 patients (15.5%) were incidentally detected to have abdominal lymphadenopathy.A total of 91 patients (61.1%) had only abdominal lymphadenopathy and the remaining 58 patients (38.9%) had both mediastinal as well as abdominal lymphadenopathy.Most of the patients (n= 139) underwent EUS-FNA using a 22G aspiration needle (22G Cook EchoTip®, 22G Olympus EZ-shot 3), while only 10 patients (6.7%) underwent the procedure using a 22G biopsy needle (22G Boston Scientific Acquire™).No differences in patient characteristics and procedures results were observed between the two needle types.All patients had adequate cellularity to make a diagnosis, from the samples taken from abdominal lymph nodes, as assessed by the on-site cytopathologist, in this study.The cytology results showed only reactive changes in 45 patients (30.2%), while 54 patients (36.2%) showed granulomatous inflammation with or without caseation.Malignant cells were seen in a total of 50 patients (33.6%), of which, features suggestive of lymphoma were seen in 11 patients (22%) and metastatic deposits were seen in 39 patients (78%) (Table 1).Among the 54 patients with granulomatous inflammation on EUS-FNA cytology, 51 patients (94.4%) were confirmed to have TB on the basis of confirmatory tests or response to ATT on follow-up; and 3 patients (5.55%) had elevated angiotensin I-converting enzyme levels along with systemic symptoms of sarcoidosis which was managed accordingly.On follow-up of patients with reactive changes on EUS-FNA cytology (n= 45), 30 patients (66.67%) showed non-specific inflammation which was managed conservatively, 8 patients (17.78%) had TB and were treated accordingly, 1 patient (2.22%) was diagnosed with sarcoidosis, while 3 patients (6.66%) showed malignant cells asperthe surgical histopathology report; 3 patients (6.66%) were lost to followup.
EUS-FNA/B in the evaluation of intra-abdominal lymphadenopathy due to TB
A total of 59 patients were diagnosed with TB during follow-up and were treated with standard anti-tubercular drugs.The baseline characteristics of these patients are shown in Table 2.Isolated abdominal lymphadenopathy was seen in 31 patients (52.5%), while 28 patients (47.4%) had both mediastinal and abdominal lymphadenopathy.All the patients presented with fever of unknown origin and a majority of them also had systemic symptoms such as weight loss and night sweats [40 patients (67.7%)].
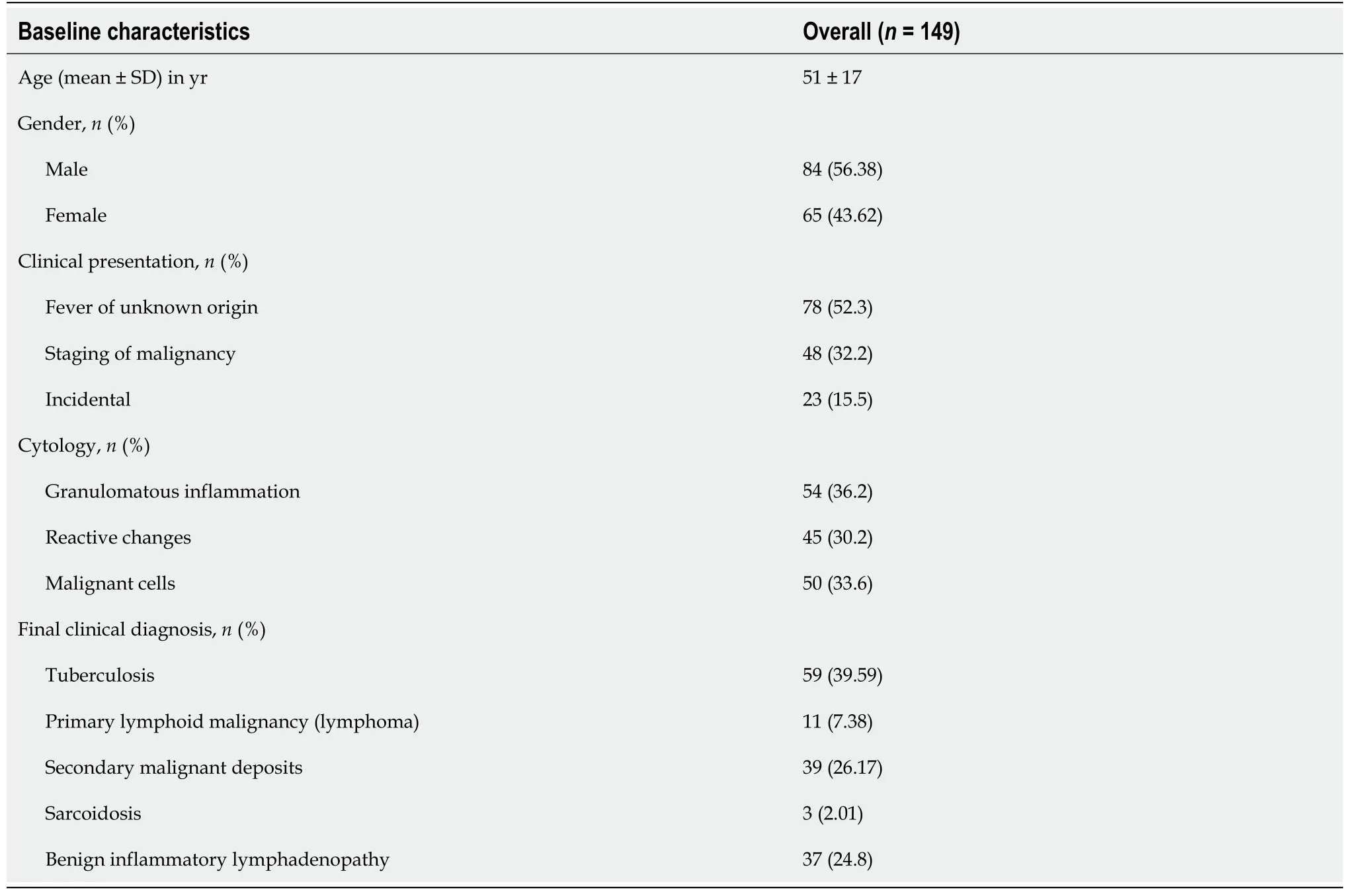
Table 1 Baseline characteristics of patients who underwent endoscopic ultrasound fine needle aspiration/biopsy for abdominal lymphadenopathy

Table 2 Characteristics of patients diagnosed with tuberculosis (n = 59)
Patients with TB were more likely to have hypoechoic nodes [37 patients (62.7%)], while 22 patients (37.3%) had heteroechoic nodes on endosonographic examination (Figure 2).A majority of these patients also had matted nodes forming a conglomerate lymphnodal mass [40 patients (67.7%)].All patients underwent EUS-FNA using an aspiration needle except for 2 patients (3.4%) in whom a biopsy needle was used.TB GeneXpert of the biopsy sample was performed in a total of 34 patients (57.6%), of which only 14 patients (41.1%) had a positive result and the remaining 20 patients (58.9%) had a false negative result.Samples from a total of 38 patients were sent for TB culture.Of these, only 12 samples (31.6%) grewMycobacterium tuberculosis, while the remaining 26 samples (68.4%) did not show any growth of organisms.

Figure 2 Endoscopic ultrasound.
Among the patients with confirmed TB, EUS-FNA/B showed granulomatous inflammation with or without caseation in 51 patients (86.4%), while the remaining patients showed non-specific reactive changes [8 patients (13.5%)].EUS-FNA/B was found to have a sensitivity and specificity of 86% and 93%, respectively, with a diagnostic accuracy of 88% in the evaluation of mesenteric lymphadenitis due to TB.
DISCUSSION
Extrapulmonary TB accounts for 15%-20% of all cases of TB[11,12].TB presenting with isolated lymphadenopathy is common in endemic areas and poses a significant diagnostic challenge[13].In the absence of characteristic symptoms or pathognomic radiographic features, isolation of the bacilli and/or identification of caseous granulomas from biopsy samples remains the gold standard.Therefore, accurate and reliable tissue acquisition from these nodes remains the cornerstone in the diagnostic evaluation of these patients.However, intra-abdominal lymphadenopathy poses unique challenges and this is where EUS-FNA/B can potentially prove invaluable in establishing a correct diagnosis.Historically, FNA cytology in conjunction with the presence of AFB, caseating necrosis and granulomas can usually provide the diagnosis in most patients.However, the sensitivity of these findings are less than ideal[14-16].In one study, 272 patients with a proven diagnosis of tubercular lymphadenopathy had AFB positivity only in 30% of direct and concentrated smears.Moreover, TB cultures were positive only in 49% with only a marginal improvement when combined with cytologic necrosis (63%)[14].In another study which included 390 patients with tubercular lymphadenopathy, only 24% were positive for AFB on the smear and cultures yielded a positive result in 35%[17].These findings highlight the poor sensitivity of tests that rely on identification of the bacilli in FNA samples.
EUS-FNA/B has seen tremendous progress in the last decade with improved image resolution, increased experience with therapeutic interventions and unique biopsy needles that can increase the quantum of tissue obtained and thereby potentially address existing pitfalls of FNA cytology in establishing a diagnosis of TB.EUS-FNA has also already been evaluated for mediastinal lymphadenopathy with an overall accuracy of 93%, sensitivity of 71% and specificity of 100% for the diagnosis of TB in the Indian population[7].However, the role of EUS-FNA/B in the evaluation of intraabdominal lymphadenopathy due to TB remains an area that merits further evaluation.The results of the present study provide valuable evidence of the validity of EUSFNA/B in the evaluation of TB presenting with intra-abdominal lymphadenopathy.Granulomas were seen in a total of 54 samples (36.2%) and the finding of granulomatous inflammation in the biopsy specimens correlated well with the diagnosis of TB in this study, with only 3 patients diagnosed with sarcoidosis.Only a minority of patients [8 patients (13.5%)] with TB (based on follow-up data and response to treatment) did not show granulomas on the FNA/B sample.Overall, EUS-FNA/B was found to be a safe and reliable modality in the evaluation of intra-abdominal lymphadenopathy due to TB with a diagnostic accuracy of 88% and a reasonable sensitivity and specificity for TB.Based on the findings of this study, an approach for the evaluation of intra-abdominal lymphadenopathy is proposed in Figure 3.
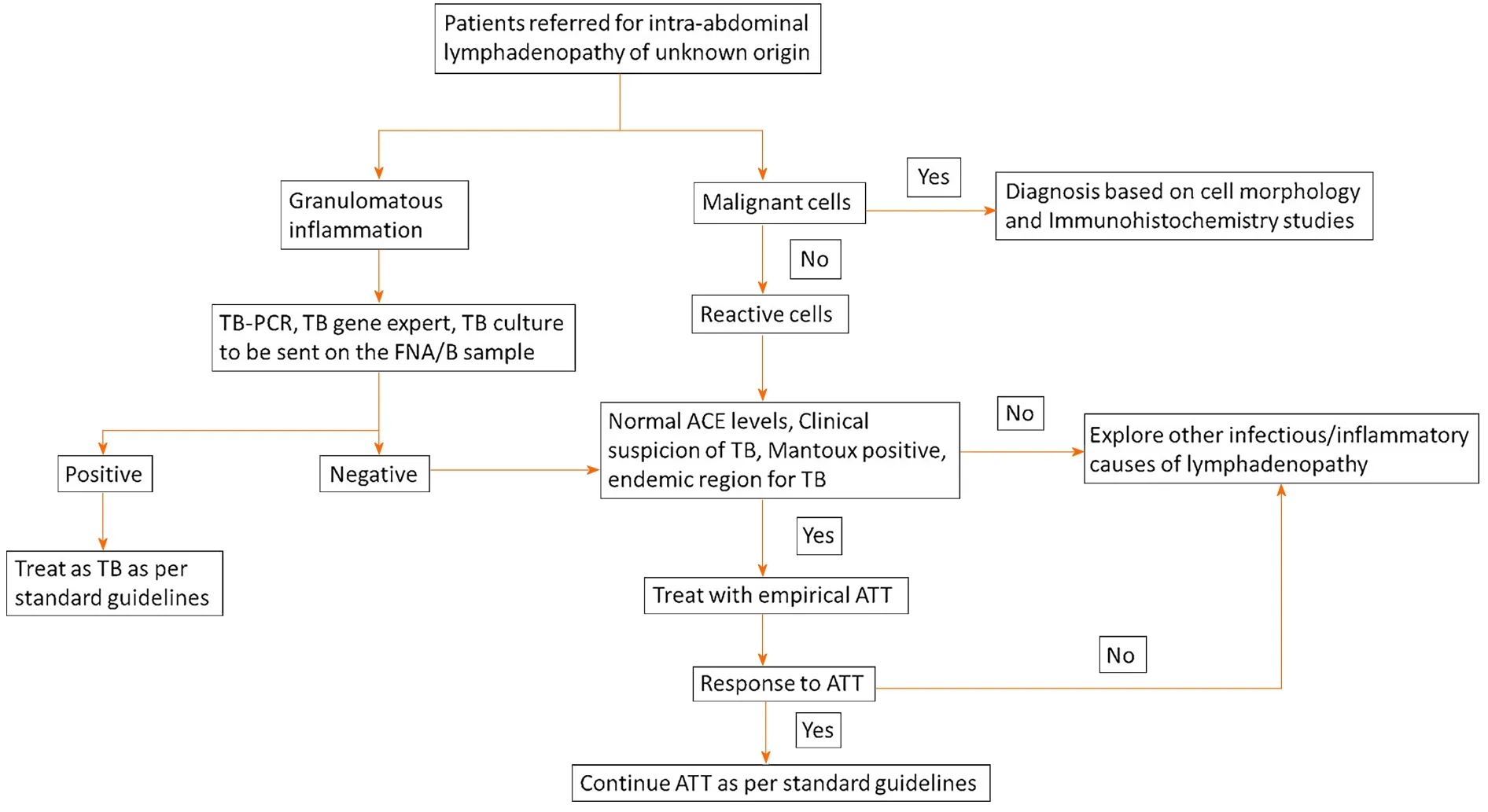
Figure 3 Proposed approach to intra-abdominal lymphadenopathy in a region endemic for tuberculosis.
In general, the quantum of tissue samples obtained from lymph nodes after EUSFNA have been found to be sufficient in most indications[4].Ancillary techniques such as applying suction and slow withdrawal have been evaluated in the setting of pancreatic lesions.However, the utility of these techniques in the setting of lymph nodes needs further clarity.In our experience, we have found no added benefit with these ancillary techniques.A thorough endosonographic evaluation prior to FNA with emphasis on choosing an ideal node that is adequately enlarged and with sharp borders, with/without matting is essential to ensure a high yield.Particular attention should be paid to the morphology of the lymph node wherein hypoechoic areas which might indicate necrosis should be avoided.Sampling of peripheral tissue within the node has yielded better tissue samples in our experience.However, this requires further validation in larger studies.
There are a few limitations in the present study.This study was performed in an area endemic for TB.Therefore, the pre-test probability of TB would be high and as such, the findings of this study would be applicable only in similar demographic groups.In addition, a definitive diagnosis of TB requires a positive culture/GeneXpert and/or PCR for tubercular bacilli.A proportion of our study population could not undergo these tests due to financial considerations and poor patient compliance.Empirical ATT is a practice followed in most regions endemic for TB, but carries with it a high risk of treatment failure and can even pose a risk for the emergence of resistant organisms.Tissue acquisition in these cases can provide valuable information and dictate therapy.Moreover, a high pre-test probability of TB, a positive Mantoux test and granulomas on the FNA sample has been shown to be a reasonable approach to start a patient on ATT[18].Moreover, all the patients who were treated with ATT using this approach showed good response to treatment on follow-up.
CONCLUSION
In conclusion, EUS-FNA/B has a high diagnostic yield with a good sensitivity and specificity in the evaluation of intra-abdominal lymphadenopathy in patients with a clinical suspicion of TB.The procedure is safe, performed with moderate sedation and can potentially prevent further invasive testing in this subgroup of patients.However, the utility of this procedure in populations with a low prevalence of TB needs more clarity.In addition, a protocol-based approach with additional tests such as TB culture, AFB stain, TB-PCR or GeneXpert in specific subgroups of patients at risk for TB needs to be developed and evaluated in future studies.
ARTICLE HIGHLIGHTS
Research background
Intra-abdominal lymphadenopathy due to tuberculosis (TB) poses a diagnostic challenge due to difficulty in tissue acquisition.
Research motivation
Endoscopic ultrasound guided fine needle aspiration/biopsy (EUS-FNA/B) has shown excellent results in patients with mediastinal lymphadenopathy.However, its role in the evaluation of abdominal lymphadenopathy due to TB needs further clarity.
Research objectives
The utility of EUS-FNA/B in the evaluation of intra-abdominal lymphadenopathy was assessed by evaluating the diagnostic yield in patients with confirmed TB.
Research methods
This was a single center retrospective study conducted in a large tertiary care hospital where patients with intra-abdominal lymphadenopathy referred for EUS-FNA/B were studied.The diagnosis of TB was confirmed and EUS-FNA/B results including cytology, pathological diagnosis, ancillary test findings (TB culture, GeneXpert) and demographics in these patients were carefully analyzed.
Research results
This study showed that EUS-FNA/B has a high diagnostic yield with good sensitivity(86%), specificity (93%) and diagnostic accuracy (88%) in the evaluation of intraabdominal lymphadenopathy in patients with a clinical suspicion of TB.Morphological findings on EUS evaluation of intra-abdominal lymphadenopathy include hypoechoic/heteroechoic nodes, with sharp borders, with/without matting.
Research conclusions
EUS-FNA/B is a viable, reliable and safe procedure, which can be performed with moderate sedation and can potentially prevent further invasive testing in this subgroup of patients.
Research perspectives
This study provides vital information that can guide the approach and management of patients with intra-abdominal lymphadenopathy.A management algorithm that highlights key points during the management of these patients is provided.However, the utility of this procedure in populations with a low prevalence of TB needs more clarity.In addition, a protocol-based approach with additional tests such as TB culture, acid fast bacilli stain, TB-polymerase chain reaction or GeneXpert in specific subgroups of patients at risk for TB needs to be developed and evaluated in future studies.
 World Journal of Gastrointestinal Endoscopy2021年12期
World Journal of Gastrointestinal Endoscopy2021年12期
- World Journal of Gastrointestinal Endoscopy的其它文章
- Application of robotic technologies in lower gastrointestinal tract endoscopy: A systematic review
- Efficacy and tolerability of high and low-volume bowel preparation compared: A real-life single-blinded large-population study
- When should we perform colonoscopy to increase the adenoma detection rate?
- Large polyps: Pearls for the referring and receiving endoscopist
- Primary prophylaxis of variceal bleeding in patients with cirrhosis: A comparison of different strategies
- Endoscopic ultrasound-guided biliary drainage-current status and future perspectives